
The RCM Consolidation Paradox: A CFO's Framework for Avoiding the Platform Trap
When vendor simplification hurts net collection rates more than it helps, here is how to build an RCM tech stack that actually holds up under payer pressure.
The latest RCM vendor reports have landed across health system finance offices, and the pressure to consolidate is real. Denial rates are climbing, AI-powered payer algorithms are getting sharper, and the operational chaos from recent clearinghouse disruptions proved that a fragmented vendor stack is a liability no organization can afford.
The question is not whether to modernize your revenue cycle technology. The question is whether consolidation actually solves the problem, or creates a more expensive one hiding inside a cleaner org chart.
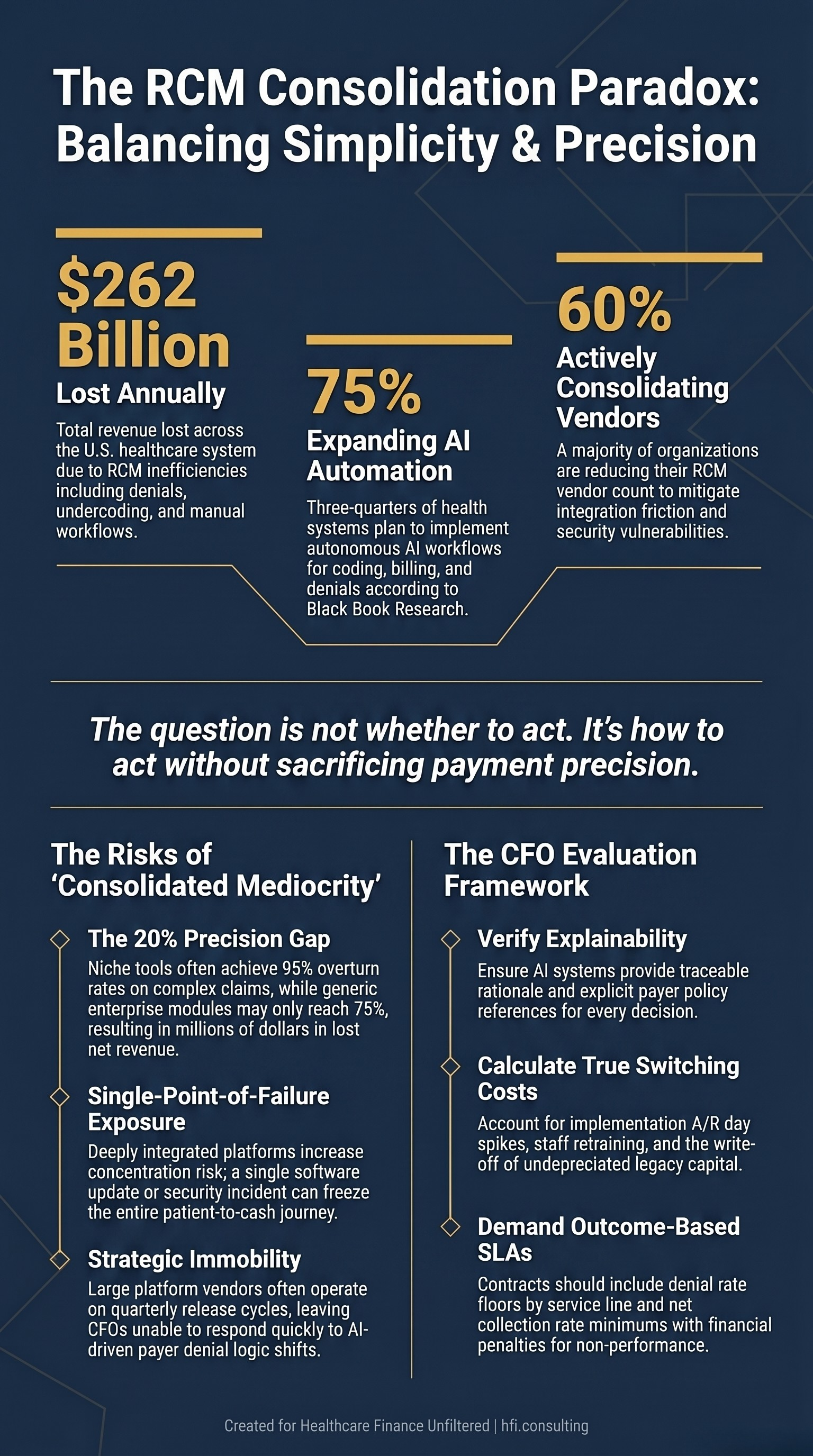
Navy stat card with gold accents showing three key RCM data points: $262B annual revenue cycle losses, 75% AI expansion plans among health systems, and 60% active vendor consolidation rate, with a prompt on protecting payment precision.
The Consolidation Case Is Partially Right
The business case for vendor simplification is not manufactured. U.S. healthcare organizations lose over $262 billion annually to revenue cycle inefficiencies, including denials, undercoding, delayed follow-ups, and manual workflows that belong in a prior decade. Managing 15 to 25 active RCM point solutions creates real administrative drag: separate contracts, separate SLAs, separate security compliance cycles, and integration friction that compounds with every EHR upgrade.
The market is responding accordingly. According to Black Book Research, over 75% of U.S. health systems plan to expand AI-driven RCM automation, with autonomous workflows across coding, billing, and denials ranking as the highest priorities. Nearly 60% are actively reducing their vendor count.
But the vendor reports tend to understate one critical variable: consolidation is a capital decision with a direct line to your net collection rate, and the math on that trade-off does not always favor simplification.
The Four Anxieties Finance Leaders Are Not Saying Out Loud
CFOs who have been through RCM platform transitions understand the strategic goal of simplification. Where they hesitate is the execution risk that vendor presentations gloss over.
The first concern is consolidated mediocrity. Point solutions became market leaders because they solve specific, high-dollar friction points at a level of precision that generalist platforms struggle to match. A niche denial tool purpose-built for complex cardiac or orthopedic claims may achieve a 95% overturn rate on those encounters. A broad enterprise platform with a generic denial module may perform at 75% on the same claims. That 20-point gap does not feel significant until you run it across a high-volume service line with $15M in annual net revenue at stake. The administrative savings from eliminating one vendor contract disappear fast.
The second concern is switching cost and stranded capital. RCM transitions are notorious for spiking A/R days during implementation windows. Staff are learning new workflows, clearinghouse connections must be remapped, and parallel operation burns resources that thin-margin organizations cannot spare. Finance leaders also face the accounting reality of writing off prior technology investments that have not fully depreciated. That write-off is visible on the income statement in a way that vendor consolidation "savings" often are not.
The third concern is single-point-of-failure exposure. The major clearinghouse disruptions of recent years were a brutal education in operational concentration risk. A fragmented vendor stack has a built-in hedge: if your prior authorization module fails, your coding and back-end billing systems continue to process claims. A deeply integrated enterprise platform means a botched software update or a security incident can freeze the entire patient-to-cash journey within hours. The cybersecurity risk alone warrants a separate conversation with your CFO-CIO leadership team, particularly given the escalating sophistication of attacks on healthcare administrative infrastructure. For a deeper look at that exposure, see the recent framework on healthcare cybersecurity financial risk planning at Healthcare Phishing Attacks Are Bypassing MFA: The CFO and CIO Operational Resilience Playbook.
The fourth concern is vendor lock-in and payer agility. Payers modify their denial logic constantly, often using AI-driven algorithms that evolve faster than enterprise platform roadmaps can accommodate. Niche vendors can rewrite their claim scrubbing logic in days to counter a new tactic. Large platform vendors typically operate on quarterly release cycles at best. The CFO who consolidates onto a single mega-platform may discover they have traded technical debt for strategic immobility at exactly the moment payer behavior shifts.
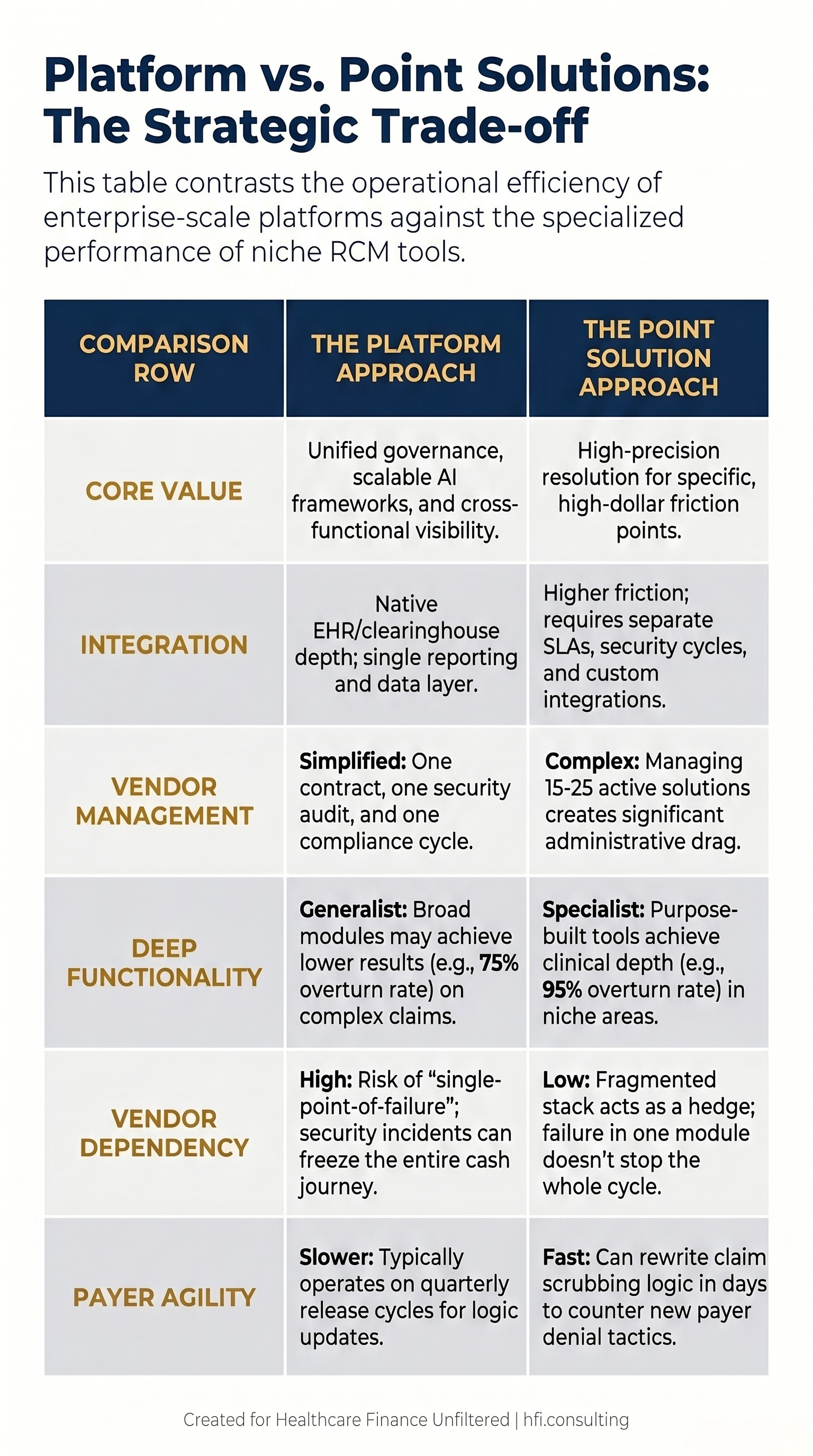
Two-column comparison table contrasting enterprise RCM platform approach versus point solution approach across six dimensions including core value, integration depth, vendor management burden, functionality depth, dependency risk, and payer agility for healthcare CFO vendor decisions.
What the Vendor Landscape Actually Reflects
The current RCM vendor market reflects exactly this tension between breadth and precision.
Enterprise-scale platforms compete on integration depth, unified governance, and scalable AI frameworks. They are best positioned for large health systems that need consistent performance across a diverse case mix and a single reporting layer across the full revenue cycle. Their AI architecture, particularly the emerging category of agentic AI systems that can plan, execute, and learn across RCM workflows, is producing measurable results. Advanced deployments are showing 30 to 60% reductions in RCM-related FTE workload and 20 to 40% denial rate reductions.
Point solutions win because they solve one problem at near-clinical depth that generalist platforms cannot replicate at scale. The market includes specialized capabilities for patient financial experience, hybrid AI-plus-human coding delivery, and advanced analytics focused on charge capture and denial root-cause analysis. These tools exist because health systems consistently found that enterprise platforms left specific high-dollar friction points unresolved.
The honest reality is that vendor marketing reflects best-case deployments, almost by definition. The 40 to 50% cash acceleration figures that appear in platform materials represent optimized implementations at organizations that invested heavily in change management, data governance, and staff retraining. Finance leaders need a framework that stress-tests those claims against their own operational context.
For a detailed look at the denial dynamics driving this urgency, the analysis at The Denial Loop Is Breaking Healthcare: What Both Sides Are Paying and What Has to Change provides the financial case for why no RCM stack can afford mediocrity in this environment.
The Progressive Hybrid: What the Market Has Actually Settled On
The consensus among health systems that have navigated this decision successfully is not full consolidation and it is not preserving a fragmented point solution ecosystem. It is a progressive hybrid model.
Health systems are anchoring core revenue cycle operations onto a centralized enterprise platform to establish automated governance, baseline AI claim scrubbing, and cross-functional visibility. They then deploy specialized point solutions selectively, only in high-ROI, high-complexity areas where the enterprise platform demonstrably underperforms. Complex specialty denials. Advanced clinical documentation improvement for high-cost DRGs. Prior authorization for specific payer populations with aggressive audit behavior.
This is a governance discipline problem as much as a technology decision. The progressive hybrid only works if finance leadership maintains rigorous criteria for what qualifies as a point solution exception, and enforces those criteria against both vendor salespeople and internal champions who have built relationships around their current tools.
In consulting work across health system contributions margin and implant cost analysis, the same pattern appears consistently. Organizations with the tightest vendor governance frameworks end up with fewer tools, better integrated data, and lower total cost of ownership, not because they blindly consolidated but because they required each vendor to demonstrate specific, measurable performance against a defined baseline before staying in the stack.
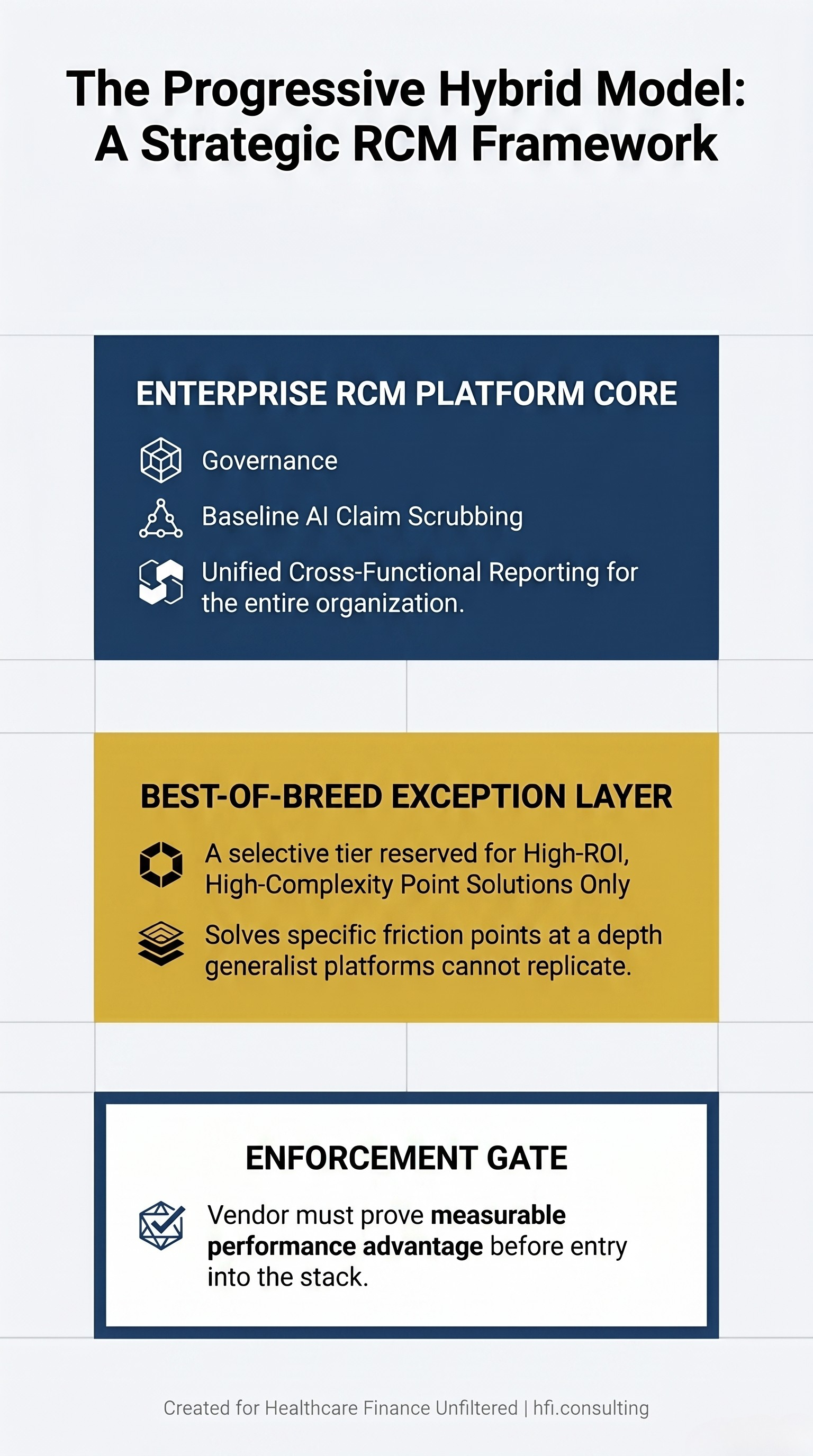
Three-layer architecture diagram illustrating the Progressive Hybrid RCM model with an enterprise platform core at top, a best-of-breed exception layer in the middle, and a performance enforcement gate at bottom, designed for healthcare CFO vendor governance planning.
A Seven-Dimension CFO Evaluation Framework
When the vendor decision lands on your desk, the goal is not to select the most impressive platform demonstration. The goal is to protect net operational income. That requires structured evaluation across seven dimensions.
Accuracy and explainability. The system must provide traceable rationale for every coding, billing, and denial decision. Payer policies and guidelines should be explicitly referenced in the output. Platforms that prioritize processing throughput over explainability create compliance risk that offsets operational gains.
Specialty and payer coverage depth. Vendor performance in one service line does not predict performance across your full case mix. Require demonstration results in your specific high-complexity specialties and across your actual payer population, not aggregate averages.
Integration architecture depth. Native EHR and clearinghouse integrations matter more than API documentation. Push for specifics: does the platform operate within existing clinical workflows without manual workarounds? Is real-time data exchange live in the current version, or dependent on batch processing with a 24-hour lag?
Implementation timeline and change management support. Time-to-value is a finance metric. Platforms requiring 18 months to full implementation carry an opportunity cost that rarely appears in the vendor's ROI model. Require pilot programs with defined measurement windows and exit provisions if performance benchmarks are not achieved.
ROI clarity and benchmarked metrics. Require vendors to present expected ROI based on comparable deployments, not directional projections. The specific metrics that matter: denial rate improvement by service line, appeal overturn rates, A/R days impact during and after implementation, and net revenue capture change versus a documented baseline.
Vendor financial stability and AI roadmap specificity. A vendor that cannot articulate a detailed AI innovation roadmap aligned with current payer market trends is a vendor you may need to replace within three years. That future migration cost belongs in the current decision model.
Operational scale fit. The right platform for a 300-bed regional system is not the right platform for a seven-hospital network. Evaluate whether pricing scales reasonably with your claim volume and whether governance controls match your actual compliance infrastructure.
The pattern of healthcare finance leaders quietly walking back over-automated AI investments after vendor promises failed to translate into net collection rate improvement is worth understanding before signing a contract. That dynamic is explored in detail at The AI Automation Trap: Why Healthcare Finance Leaders Are Quietly Walking Back Their Biggest Bets.
If you are building the internal business case for an RCM vendor evaluation or working through the financial model for a platform transition, I can help. Connect with me directly at hfi.consulting or reply to this email.
What Ironclad SLAs Should Actually Specify
The CFO's mandate in any RCM vendor decision is payment precision, not vendor simplicity. That means every consolidation or platform addition must be governed by contracts that protect the organization when performance falls short of what was promised in the sales process.
The SLA provisions that matter are not standard uptime guarantees. They are denial rate floors by service line with financial penalties for non-performance. They are net collection rate minimums that trigger contract remedies. They are explicit commitments to payer policy update timelines measured in days, not quarters. They are business continuity provisions that specify exactly what happens to cash flow during an extended platform outage.
Health systems that navigate RCM transitions successfully treat vendor contracts as financial instruments, not operational documentation. The SLA is where platform promises become enforceable obligations.
If a vendor declines to commit to outcome-based performance metrics in writing, that is a material finding. Most RCM transition failures involve contracts that protected vendor revenue while leaving performance risk entirely on the health system's balance sheet.
Before the Next Vendor Presentation
Three questions are worth answering internally before a vendor reaches your calendar.
First, what is your current denial rate by payer and by service line, and which of those rates is each vendor specifically claiming they can move, with what timeline, and with what contractual accountability?
Second, what is your true switching cost, including A/R days impact during implementation, staff retraining investment, and the stranded capital write-off from prior technology that has not fully depreciated?
Third, what does your current vendor contract language actually commit each vendor to deliver, and have you enforced it? Most health systems have not.
The market is moving toward RCM vendors that execute autonomously, not just report efficiently. The organizations that win this transition will be the ones that held vendors to performance standards before signing, not after. Your net collection rate cannot absorb the difference between a vendor's demo results and their contractual minimums.
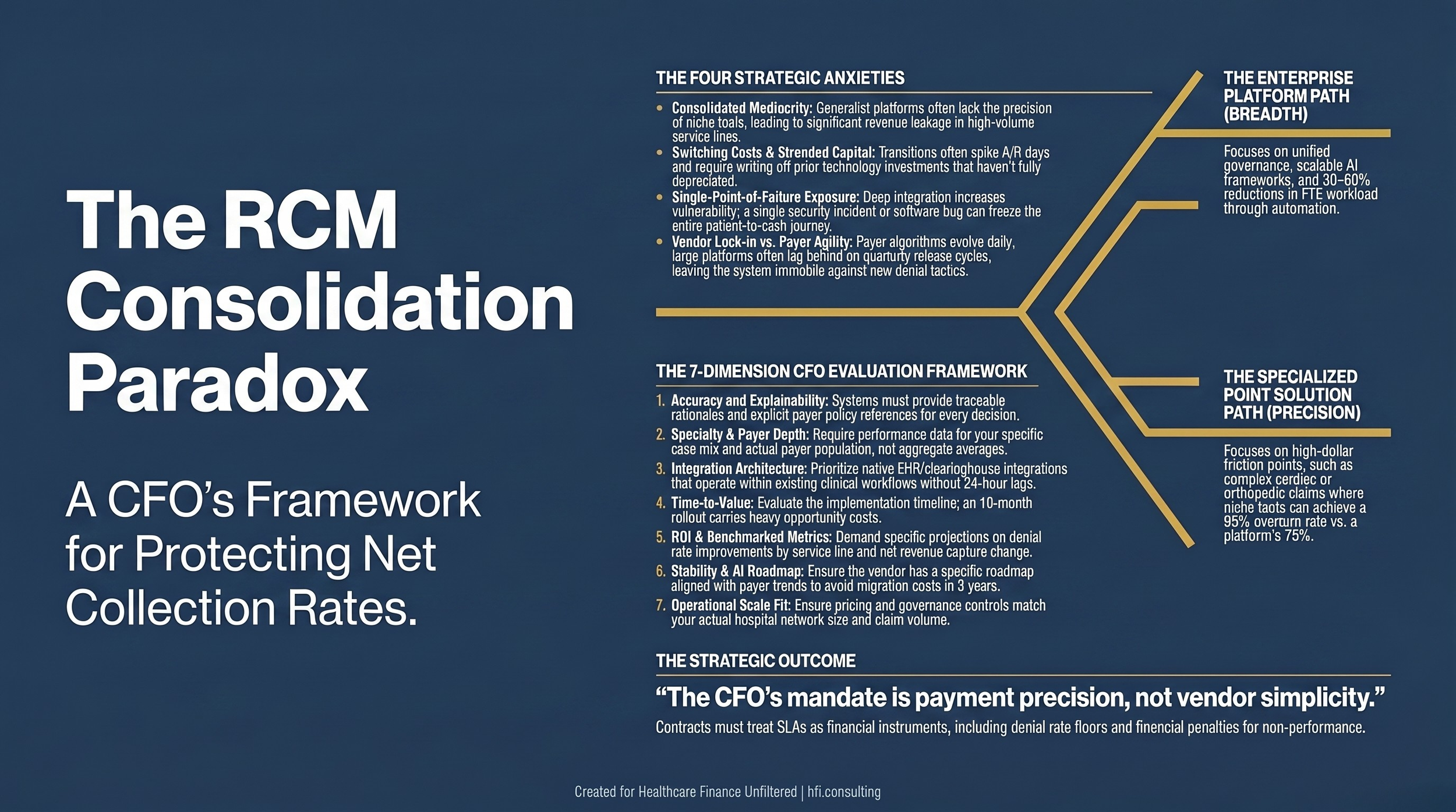
Navy landscape card with gold accent lines showing the title "The RCM Consolidation Paradox: A CFO's Framework for Protecting Net Collection Rates" with hfi.consulting branding for healthcare finance article sharing.
Subscribe to Healthcare Finance Unfiltered for weekly frameworks on the revenue cycle decisions that protect margin and position your organization ahead of the next market shift. If your team is working through an RCM vendor decision, reach out at hfi.consulting.
P.S. What is the biggest gap you have seen between what an RCM vendor promised in the sales process and what actually showed up in your net collection rate after go-live? Hit reply and tell me. The patterns across organizations are worth a follow-up piece, and I am genuinely curious where the biggest disconnects are landing right now.