
The Denial Loop Is Breaking Healthcare: What Both Sides Are Paying and What Has to Change
Denials cost the industry $262 billion annually and are now driving contract terminations. The math no longer works for payers or providers.
On April 8, Jefferson Health filed suit against Aetna in federal court. The allegation is specific and damaging: Aetna's new inpatient payment policy was classifying a 72-year-old stroke patient admitted to an ICU, intubated, experiencing renal failure, as "low severity." The health system was paid at an observation rate. Only after the stay extended past five days and Jefferson followed up with additional clinical documentation did Aetna reclassify the case.
That is not a billing dispute. That is the payer-provider relationship in 2026.

Square infographic on navy background showing $262 billion lost annually to healthcare claim denials with the note that 86 percent are avoidable.
Finance leaders on both sides of this equation are watching the denial loop accelerate. Denial rates from private payers rose from 8% to 11% between 2021 and 2023. The MGMA reported that 60% of medical groups saw higher denial rates in 2024 than the year before. HFMA's 2024 CFO Pain Points survey found that 82% of health system CFOs believe payer denials have increased significantly since pre-pandemic levels, and 90% cite denials as their top revenue cycle challenge. The Advisory Board's April 2026 proprietary survey confirmed what most finance leaders already know: the administrative burden of denials is now fueling clinician burnout, eroding provider-plan trust, and driving the kind of contract terminations that shrink network adequacy for the patients both sides are supposed to serve.
The question worth asking is not who is winning. Nobody is winning.
What the Numbers Actually Cost Each Side
The industry-level figures are large enough to be numbing. U.S. hospitals spend an estimated $19.7 billion annually just on appeals and overturning denied claims. Each reworked denial costs between $25 and $118 in administrative expense. Roughly 65% of denied claims are never resubmitted at all, meaning that revenue is permanently lost.
For providers operating on margins in the 2% to 3% range, the math is brutal. A practice submitting 1,000 claims monthly at an average $200 reimbursement, with a 10% denial rate and 50% successful appeal rate, loses $10,000 per month, $120,000 per year, before accounting for the staff cost of working those denials. For a hospital system with tens of thousands of monthly claims, the scale of that loss is a strategic threat, not a billing inconvenience.
What the headline numbers obscure is what happens on the payer side. Providers denied often do not fight. They absorb the loss or they redirect resources. But over time, those same providers make contracting decisions based on which plans are worth the administrative friction. The plans with the most burdensome denial processes are the ones losing network participation, facing litigation, and spending more on their own internal appeals management than the original denial saved. The Jefferson lawsuit is not a one-off. It is part of a growing pattern of providers deciding that court is the more efficient path than the appeals queue.
The Real Burden: Time, Trust, and Clinical Staff
Advisory Board's survey data, published this month (paywalled), puts specific numbers on a problem finance leaders often describe in general terms. Treating clinicians spend up to 90 minutes per week just on submitting prior authorization requests. The claims denial appeal process consumes additional time across nine distinct steps, with peer-to-peer review and appeal letter writing among the most time-intensive.
The steps providers find most burdensome are not the administrative ones. Investigating the cause of a denial was identified as particularly burdensome by 50 to 52% of provider staff surveyed, across both prior authorization and claims denial processes. Writing letters of appeal came in at 38 to 41%. These are not tasks that a front-desk coordinator handles. These are tasks that pull clinicians and senior staff away from patient care and productivity metrics.
The human cost compounds the financial one. A 2025 AJMC survey found that 89% of clinicians report prior authorization requirements contribute to burnout. When physicians feel that their clinical expertise is being second-guessed by algorithmic denials or non-specialist reviewers, the frustration is not merely operational. It is professional. Advisory Board's qualitative interviews captured this directly, with one provider describing the experience as being told to explain coding rationale to claims reps with no clinical background, while being kept on hold and unable to reach anyone with the knowledge to help.
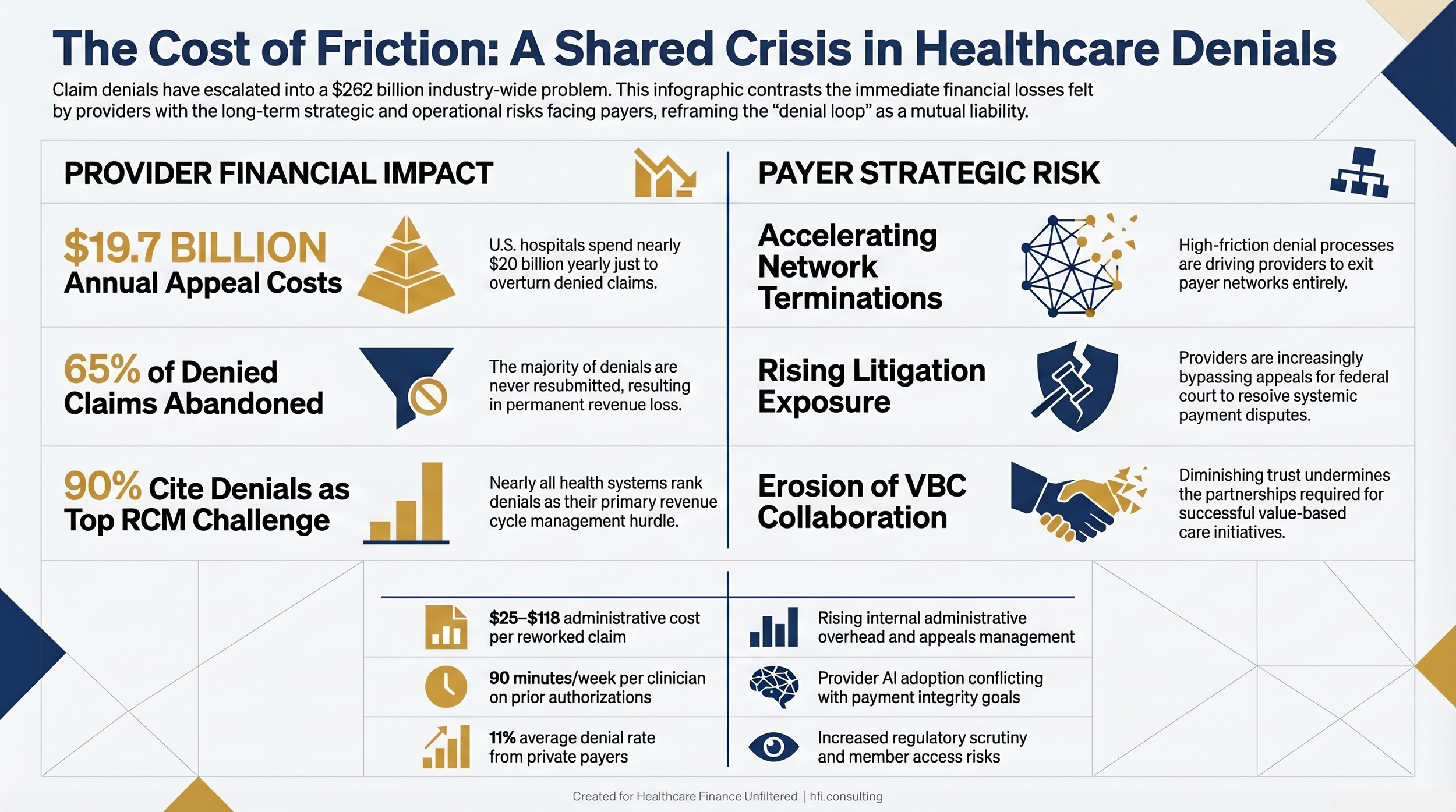
Landscape comparison table contrasting provider financial impact of denials against payer strategic risk from denial-driven provider friction and network instability.
What Is Driving Escalation
The structure of the problem has changed. Three dynamics are accelerating the denial loop in ways that make the old approach of absorbing the friction unsustainable.
Automated denials without clinical context. Payers are increasingly using algorithmic tools to reject claims at volume, often without the kind of clinical review that a complex case warrants. Aetna's downcoding policy is a formalized version of this logic applied to inpatient severity classification. The policy was designed, Aetna says, to expedite approvals. Jefferson's lawsuit says it pays inpatient stays at observation rates regardless of clinical complexity, unless the stay extends past five midnights. A stroke patient in the ICU does not stop being a high-severity case because she was discharged before day five.
Avoidable administrative failures on both sides. Approximately 86% of denials are avoidable, according to Becker's Hospital Review. The most common drivers are coding errors, missing prior authorization, and eligibility issues that could have been caught at the front end. These are process failures, not clinical disputes, and they consume the same appeals infrastructure as legitimately contested clinical decisions. The result is a system where genuine clinical disagreements are buried under a volume of preventable administrative errors that neither side has adequately solved.
The appeals abandonment calculation. When the cost to rework a claim exceeds the reimbursement value, providers write it off. Health systems frequently absorb denial losses not because the denial was correct, but because the rework window closed before anyone could get to it. This is not a reflection of clinical accuracy. It is a staffing and workflow problem that payers have historically benefited from financially. The Advisory Board's report is direct on this point: if plans do not address provider friction, providers will build their own AI-driven revenue cycle tools specifically designed to combat plan payment integrity strategies.
That is not a future scenario. It is already underway.
From the Inside: What Working the Problem Actually Looks Like
The narrative that payers simply do not care about provider friction is not accurate at every organization, and it matters for finance leaders to understand that. During my time on the payer side at Florida Blue Medicare, we identified a systemic technical issue driving a significant denial backlog. It was not a policy decision. It was a process failure that compounded over time until the volume was undeniable.
Leadership recognized it. We assembled a cross-functional team: IT, Utilization Management, Case Management, and Business Operations. We made the case for dedicated resources, received funding, and spent three months working through the backlog while simultaneously fixing the underlying process issues. It was not glamorous work. But it happened because people inside the organization looked at the data, acknowledged the problem, and were given the latitude to address it.
That model, internal accountability combined with cross-functional authority and executive support, is exactly what the Advisory Board's report recommends. The plans that will rebuild provider trust are the ones that invest in this kind of internal infrastructure, not as a regulatory response, but as a strategic imperative.
On the provider side, the documentation burden for complex clinical conditions is a category of its own. Neurological conditions in particular require providers to systematically rule out multiple diagnoses before arriving at the correct one. The prior authorization process frequently requires documentation of that entire ruling-out sequence, generating paperwork volume that has nothing to do with whether the care was appropriate and everything to do with whether the plan's internal criteria were met. Clinicians manage this burden as a cost of doing business. Finance leaders who have not looked closely at what their clinical staff spends on this category of authorization work should.
For revenue cycle leadership, that AI in Revenue Cycle Management framework we covered earlier this year is directly relevant here. The organizations building AI-assisted prior auth and denial response tools are not doing it to be innovative. They are doing it because the manual process is no longer financially sustainable.
What Finance Leaders Can Do Now
The Advisory Board report identifies five root causes of provider frustration that plans must address. They translate into specific operational decisions that finance leaders on both sides can influence.
For payer CFOs and VPs of Finance:
Denial activity that saves money on individual claims but generates provider network instability, appeals overhead, and litigation exposure is not actually saving money. The Jefferson lawsuit will cost Aetna in legal fees, management attention, and network relationship capital regardless of how the case resolves. Finance leadership should be asking their utilization management teams to quantify the fully loaded cost of contested denials, not just the claim-level savings.
Prior authorization volume reduction is a direct financial lever. Fewer authorizations required for high-approval-rate services means less internal administrative overhead, less provider friction, and faster care delivery. This is not a concession to providers. It is an efficiency calculation.
Peer review matching matters operationally. When a cardiologist's admission is reviewed by a non-specialist and denied, the resulting peer-to-peer request, rescheduling, and repeat review consume more administrative time than a first-time match with appropriate specialty credentials would have. The Advisory Board recommends specialty matching as a specific process improvement.
For provider CFOs and revenue cycle leaders:
Denial write-offs due to missed rework windows are a workflow problem with a workflow solution. Organizations that have not audited their denial rework timelines by payer and denial category are likely leaving recoverable revenue on the table. The revenue cycle diagnostic framework we outlined in our 340B analysis applies here as well. The question is not whether your denial rate is acceptable. It is whether your rework rate reflects your actual recoverable revenue opportunity.
Front-end investment in eligibility verification and prior authorization management reduces the volume of avoidable denials that consume the same staff resources as complex clinical disputes. Clean claim rates matter. A 99% clean claim rate is not a success metric if 30% of claims are still denying post-submission.
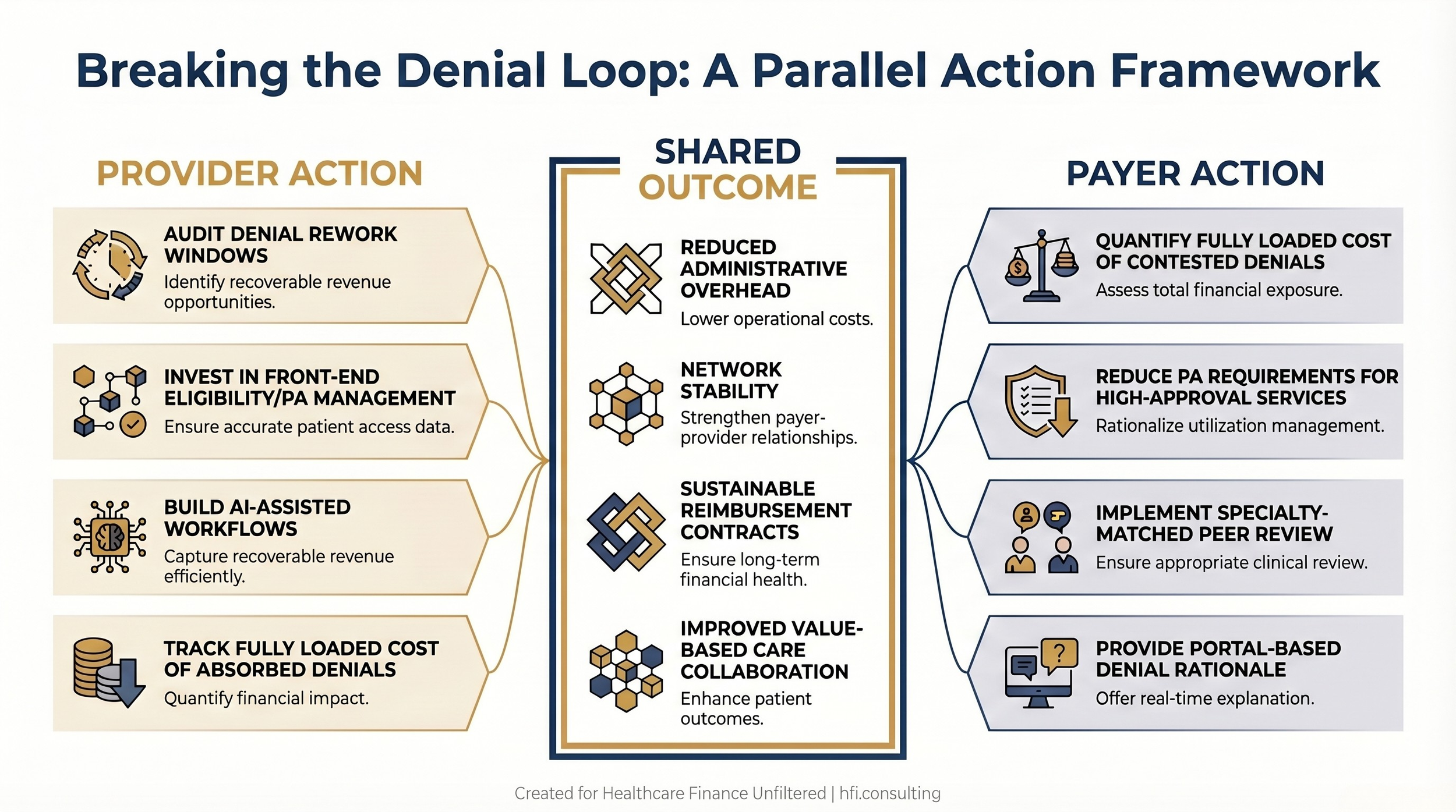
Landscape process flow diagram showing parallel provider and payer action tracks converging on shared outcomes including reduced administrative cost, network stability, and sustainable contracts.
The Trust Gap Is a Finance Problem
Advisory Board's conclusion is worth sitting with: AI revenue cycle solutions may improve efficiency, but they cannot solve the trust gap between plans and providers. The underlying problem is relational, and relationships in healthcare contracting have direct financial consequences.
Network terminations reduce member access and trigger regulatory scrutiny. Litigation consumes resources and management attention that neither side has to spare. The denial loop, left unaddressed, drives both sides toward increasingly adversarial postures that make the value-based care partnerships both sides need operationally impossible.
The Kaiser $556 million Medicare Advantage settlement we analyzed earlier this year was a visible consequence of systemic process failures allowed to compound over time. The Jefferson lawsuit is another. Finance leaders at both payers and providers should be asking whether their current denial processes, if examined at that level of scrutiny, reflect the relationship they want to be defending in court.
If your organization is actively working through a denial rate spike or a specific payer friction issue, I want to hear what you are seeing on the ground. Hit reply and tell me which category of denial is consuming the most resources on your team right now.
What Both Sides Owe Each Other
The math on denials has changed. The cost to rework a claim, the volume of auto-denials, the willingness of providers to litigate rather than absorb, and the regulatory pressure on Medicare Advantage plan behavior have all shifted in ways that make the old equilibrium unsustainable.
Finance leaders are not positioned to solve the trust gap unilaterally. But they are positioned to ask better questions internally: What is the fully loaded cost of this denial category? What is the rework window utilization rate on these payer contracts? What would it cost to invest in front-end prevention versus back-end rework?
Those are not clinical questions. They are finance questions. And the organizations that answer them honestly will be in a better position to build the kind of payer-provider relationships that actually survive the next contract negotiation.
Healthcare Finance Unfiltered covers the operational and financial decisions that CFOs are navigating in real time. If this kind of analysis is useful to your work, subscribe and share it with a colleague who is dealing with the same pressures.
Subscribe to Healthcare Finance Unfiltered
P.S. What is the single denial category consuming the most administrative time on your team right now? Prior auth, clinical necessity, coding, or something else entirely? Hit reply and tell me. I am building a follow-up piece specifically on the categories where finance leaders say the ROI on fighting denials is clearest, and your input shapes what goes in it.
Source note: The Advisory Board "Hidden Cost of Denials" report cited in this article is a proprietary, paywalled publication from April 2026.