
Healthcare Phishing Attacks Are Bypassing MFA: The CFO and CIO Operational Resilience Playbook
Healthcare led all industries in a 35,000-user phishing campaign that bypassed MFA. Here is the CFO and CIO response framework.
Microsoft Threat Intelligence issued a formal warning on May 4, 2026 that healthcare was the most targeted industry in a large-scale, multistage phishing campaign that reached more than 35,000 users across over 13,000 organizations, primarily in the United States. The attack used adversary-in-the-middle (AiTM) techniques to intercept authentication tokens in real time, enabling attackers to bypass multifactor authentication entirely and gain direct account access.
That last detail is the one that should command your full attention. MFA was supposed to be the floor. For healthcare organizations, it is no longer sufficient on its own.
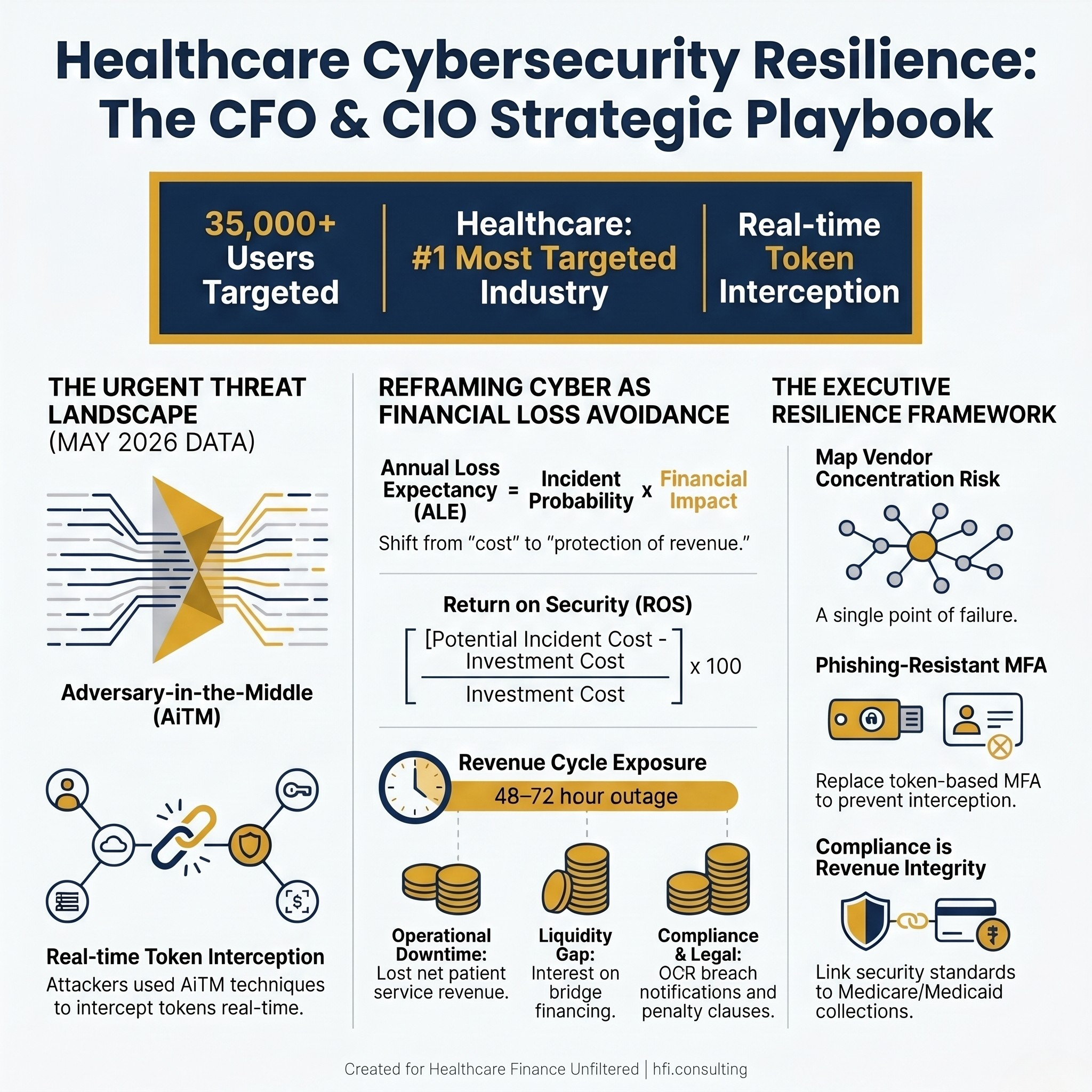
Stat card showing Microsoft May 2026 phishing campaign data: 35,000 users targeted across 13,000 organizations, adversary-in-the-middle technique bypasses standard multifactor authentication
This Is a Finance Problem, Not Just an IT Problem
The framing that cybersecurity belongs entirely to the CIO has been expensive for healthcare organizations. When a phishing campaign successfully bypasses MFA and gains access to billing systems, claims processors, and revenue cycle platforms, the financial exposure is immediate and compounding.
Scott Gee, the AHA's deputy national director for cybersecurity and risk, made the stakes explicit in the May 2026 advisory. The risk is not limited to protected health information. The more direct threat is the shutdown of critical systems and the cascading impact on patient care and financial operations.
Finance leaders who lived through a Change Healthcare-style disruption know exactly what that shutdown looks like on a cash flow statement. Lost net patient service revenue, bridge loan interest, manual claims processing labor, and delayed reimbursements do not wait for an IT remediation timeline. And unlike a payer dispute or a regulatory penalty, a ransomware event or credential compromise hits every revenue stream simultaneously.
Healthcare remains a persistent target precisely because the sector combines three conditions that attackers seek: high-value sensitive data, operational pressure that creates response time advantages for attackers, and complex technology ecosystems with multiple vendor access points. The Microsoft alert is not an anomaly. It is a confirmation that the pattern has not changed, and the techniques are getting more effective.
Reframe Cybersecurity as Loss Avoidance
The most productive conversation a CFO can have with a CIO right now is not about budget line items. It is about Annual Loss Expectancy (ALE) and what a 48-hour revenue cycle outage costs your specific organization.
The calculation is straightforward: multiply the probability of a significant incident by the financial impact if one occurs. The result shifts the conversation from "How much does this security tool cost?" to "What is the cost of not having it?" That framing makes cyber investment defensible in a board presentation in a way that a threat briefing rarely does.
A more precise measure for healthcare leadership is Return on Security (ROS):
ROS = (Cost of Potential Incident minus Cost of Security Investment) / Cost of Security Investment x 100
A $1 million investment that prevents a $10 million ransomware disruption represents a 900% ROS. That is a capital allocation argument, not an IT budget request.
Modeling your organization's cyber financial exposure:
Lost net patient service revenue for 48 to 72 hours of revenue cycle downtime
Interest on any bridge financing required to cover the cash flow gap
Manual claims processing labor and temporary staffing costs during system recovery
Payer notification requirements and potential contract penalty clauses
OCR breach notification and patient notification compliance costs
The organizations that have built this model tend to approve security investments faster. The ones that have not tend to discover the real number during an incident rather than before one.
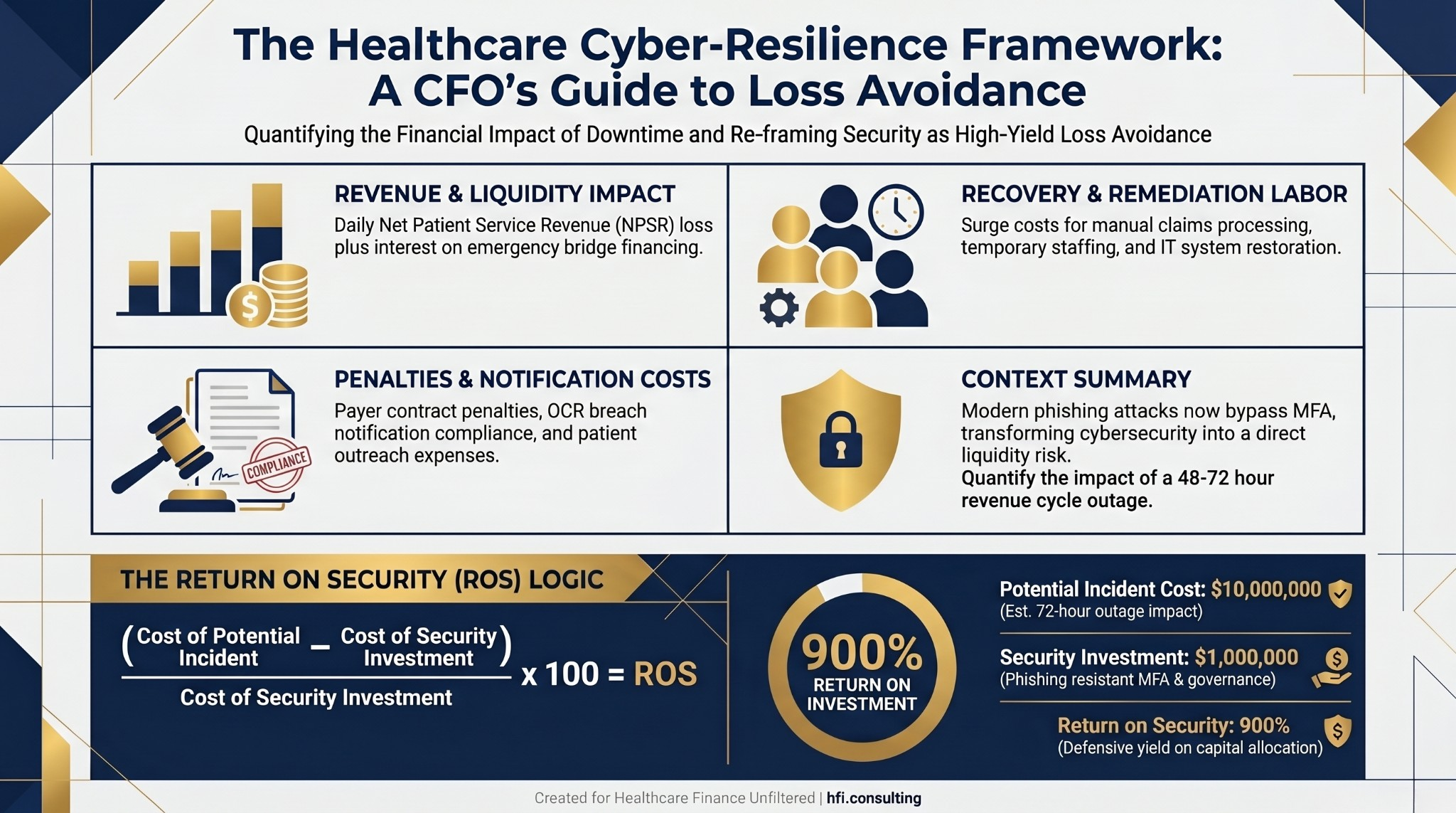
Financial framework diagram showing four components of healthcare cyber incident cost and the Return on Security formula with a worked example
The Digital Supply Chain Is Your Biggest Vulnerability
The May 2026 phishing campaign targeted credential theft at scale. But the larger and more persistent risk for most health systems sits in the vendor ecosystem, not the internal network.
If a single vendor manages 80 percent of your claims processing, a breach at that vendor is not a technology incident. It is a liquidity crisis. That lesson from Change Healthcare has still not been fully absorbed into how most finance teams think about third-party concentration risk.
Working with your CIO on vendor governance starts with specific contract questions, not general security assessments. Right-to-audit clauses should be standard in any revenue cycle or claims processing agreement. Contracts with third-party billing and cloud vendors should include explicit cybersecurity performance requirements, breach notification timelines of 24 to 72 hours (not 60 days), and indemnification for OCR penalties and patient notification costs.
Concentration risk analysis is a finance function, not an IT function. If you do not know which vendors are single points of failure for your revenue cycle, that answer needs to come from a joint CFO-CIO review. It should not surface for the first time at the next board risk committee meeting.
In my work supporting Medicare Advantage operations at Florida Blue Medicare, vendor data flow disruptions were never abstract events. Claims adjudication, risk adjustment submissions, and quality reporting all depend on clean, timely data exchange with external partners. When one upstream vendor changed a data format without advance notice, it affected downstream accuracy in ways that took weeks to fully identify. No alarm triggered. The pipeline appeared to run normally. The data just did not reconcile. Concentration risk compounds quietly, and it surfaces at the worst possible time.
Zero Trust Principles Apply to Finance Operations, Too
Zero Trust architecture gets discussed primarily in IT contexts, but the underlying principle, never trust and always verify, is exactly how internal audit has always worked. Finance leaders should be advocating for it because it protects the specific systems they own and the transactions they are responsible for.
Network segmentation between the financial network (payroll, accounts payable, ERP) and the clinical network is a concrete deliverable. If a nurse's workstation is compromised through a phishing email, the attacker should not be able to reach wire transfer systems or vendor payment instructions. That is a solvable architectural problem, but it requires finance leadership to ask for it specifically.
Multifactor authentication for internal movements, not just at login, matters as much as perimeter MFA. Changing vendor payment instructions, accessing high-value financial databases, and approving large disbursements should each require secondary verification. These are exactly the transaction types that wire fraud and business email compromise attacks target.
The May 2026 phishing campaign bypassed standard MFA by intercepting authentication tokens before the authentication process completed. Phishing-resistant MFA, such as hardware security keys or passkey-based authentication, closes that gap because there is no token to intercept. That is a technology decision, but the finance team needs to understand the distinction before accepting a cost-saving alternative that preserves the vulnerability.
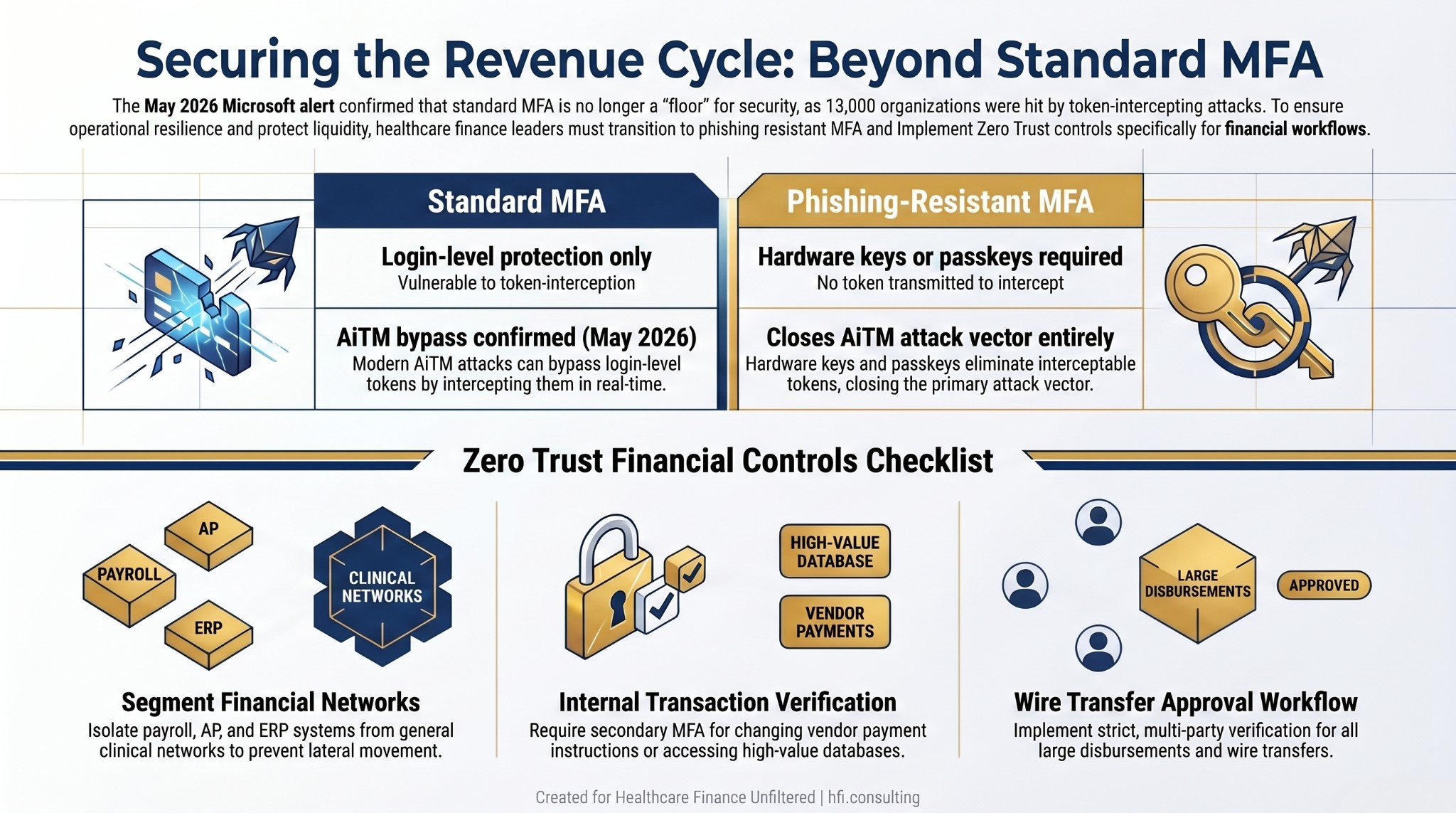
Comparison table of standard MFA versus phishing-resistant MFA capabilities and a Zero Trust financial controls checklist for healthcare CFOs
This is also where the broader question of IT governance accountability becomes a finance leadership responsibility. The CFO's role in IT risk has been covered in depth in IT Governance Is Now a Finance Problem for Health System CFOs. The phishing alert from Microsoft makes the case for that seat at the table more clearly than any governance framework document can.
If You Work With HFI Consulting
Healthcare cybersecurity risk is not going to decrease. If your organization does not have a current CFO-CIO risk quantification model, that is the starting point. HFI Consulting works with finance teams to build the financial exposure framework and vendor governance structure that makes cyber investment decisions defensible at the board level. Learn more at hfi.consulting.
Cyber Insurance Has Changed. Your Attestation May Not Have.
The cyber insurance market in 2026 is restrictive in ways that most CFOs have not fully mapped to their renewal process. Finance leaders often sign the attestation forms. The CIO typically provides the technical answers. The gap between what the application says and what the organization actually has in place is where denied claims happen, and it does not have to involve any intentional misrepresentation.
Every "yes" on a cyber insurance renewal application should be backed by documented evidence. If the form asks whether endpoint detection and response tools are deployed on all endpoints, that answer needs to come from verified inventory, not from the assumption that the CIO would have flagged a gap. Policy denial during a breach investigation is a far more expensive discovery than a gap found during renewal review.
A dedicated cyber contingency reserve is worth modeling. Insurance covers what it covers. Deductibles, uncovered losses, reputational remediation, and productivity recovery often fall outside the policy. A reserve specifically allocated for cyber-recovery liquidity applies the same logic that finance teams already use for self-insured medical stop-loss programs. The mechanics are familiar. The application to cyber is still underutilized.
Compliance Is Revenue Integrity
HHS and OCR have introduced more rigorous Cybersecurity Performance Goals (CPGs) in 2026, and the enforcement framing has shifted from penalty-after-breach to reimbursement linkage. Meeting baseline security standards is increasingly tied to the ability to collect Medicare and Medicaid payments.
That reframe matters for how cybersecurity investments get classified and prioritized in budget conversations. A firewall upgrade is a cost. A control that protects your ability to collect $40 million in government reimbursements per quarter is revenue integrity infrastructure. The budget conversation changes when the classification changes, and finance leadership is the right team to make that argument internally.
Tabletop exercises for finance are not optional preparation. When the EHR is down, finance leaders need documented answers to specific questions: How are charges tracked? How is payer communication managed? What manual processes exist to keep cash flowing during an extended outage? At Ascension, working across seven hospitals, downtime scenarios were planned events, not reactive scrambles. The organizations that practiced recovered faster and documented losses more accurately, which mattered for both insurance claims and regulatory reporting.
The operational context for this kind of data dependency is detailed in Healthcare Process Automation: CFO Guide to FHIR, AI Workflows, and Operational Intelligence. The automation frameworks that make revenue cycle operations more efficient also create data dependencies that require specific attention in business continuity planning.
Our earlier piece, Healthcare Cybersecurity 2026: The CFO's Financial Risk and Budget Planning Guide, covers the foundational budget planning framework in depth. This article builds on that foundation with the specific CFO-CIO accountability structure that the current threat environment requires.
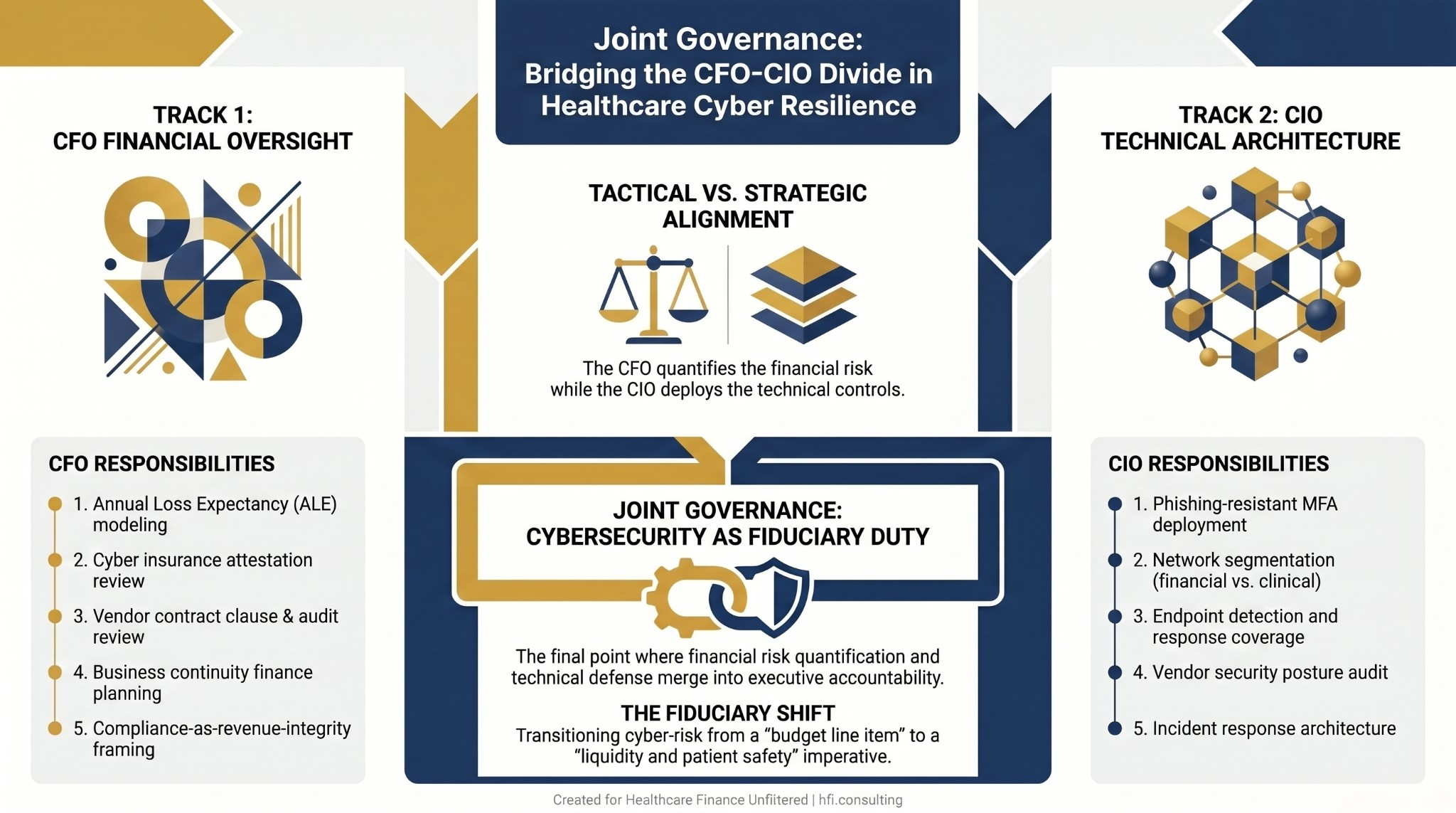
Process flow diagram showing parallel CFO and CIO cybersecurity responsibilities converging into joint governance model with cybersecurity framed as fiduciary duty
The CFO and CIO Accountability Split
The AHA's framing is useful here: training and vigilance address the how. But the why matters just as much in building workforce readiness. Employees who understand that a compromised credential can shut down the revenue cycle, delay patient care, and trigger regulatory review respond differently than employees who receive another mandatory phishing awareness email.
That message carries more weight when it comes from finance leadership reinforcing the financial stakes, not from IT sending a reminder about suspicious attachments.
The accountability structure that works in healthcare organizations with mature cyber resilience is clear. The CFO provides the financial risk quantification and business impact framing. The CIO provides the technical controls and architectural response. Neither can do the other's job effectively. Both have to show up for the same conversation, not separate briefings that never get reconciled into a unified strategy.
The Microsoft warning from May 2026 is not a one-time event to note and file. Healthcare will remain the most targeted sector because it combines sensitive data, operational pressure, and complex vendor ecosystems in a way that creates persistent opportunity for attackers. The question is not whether another campaign is coming. It is whether your organization has the joint finance-IT framework to respond before the next incident becomes a liquidity event.
The Framework in Practice
Step 1: Build the loss avoidance model. Calculate ALE and ROS for your specific organization before the next budget cycle, not after an incident.
Step 2: Map vendor concentration risk. Identify which vendors are single points of failure for revenue cycle operations and update contracts with right-to-audit, breach notification SLA, and indemnification clauses.
Step 3: Verify your zero trust controls. Confirm network segmentation between financial and clinical systems, and ensure phishing-resistant MFA is in place for high-value financial transactions.
Step 4: Review your insurance attestation. Reconcile every "yes" on your cyber policy renewal with documented evidence. Know your deductible exposure and model a contingency reserve accordingly.
Step 5: Run a finance-specific tabletop exercise. Test your manual charge capture, payer communication, and cash flow continuity processes before you need them.
If your organization is evaluating cyber risk quantification, vendor governance frameworks, or CFO-CIO alignment on security investment strategy, the team at HFI Consulting can help structure that conversation. Visit hfi.consulting to learn more.
P.S. When a phishing campaign bypasses your MFA and reaches your billing system, what is the first call you make? Is it to IT, legal, finance, or the payer? Hit reply and tell me what your incident response protocol looks like from the CFO's chair.