
CMS Claims Attachments Final Rule 2026: The CFO's Budget Guide to Eliminating Fax Machines
CMS just mandated the end of fax and mail for claims documentation. Here's what it costs, what it saves, and how to plan your transition.
CMS just issued a final rule that gives covered entities two years to stop sending claims documentation by fax and postal mail. The projected industry savings are $781 million annually. The compliance deadline is May 26, 2028. If your organization is still running claims attachments through a fax machine, the clock is now officially ticking.
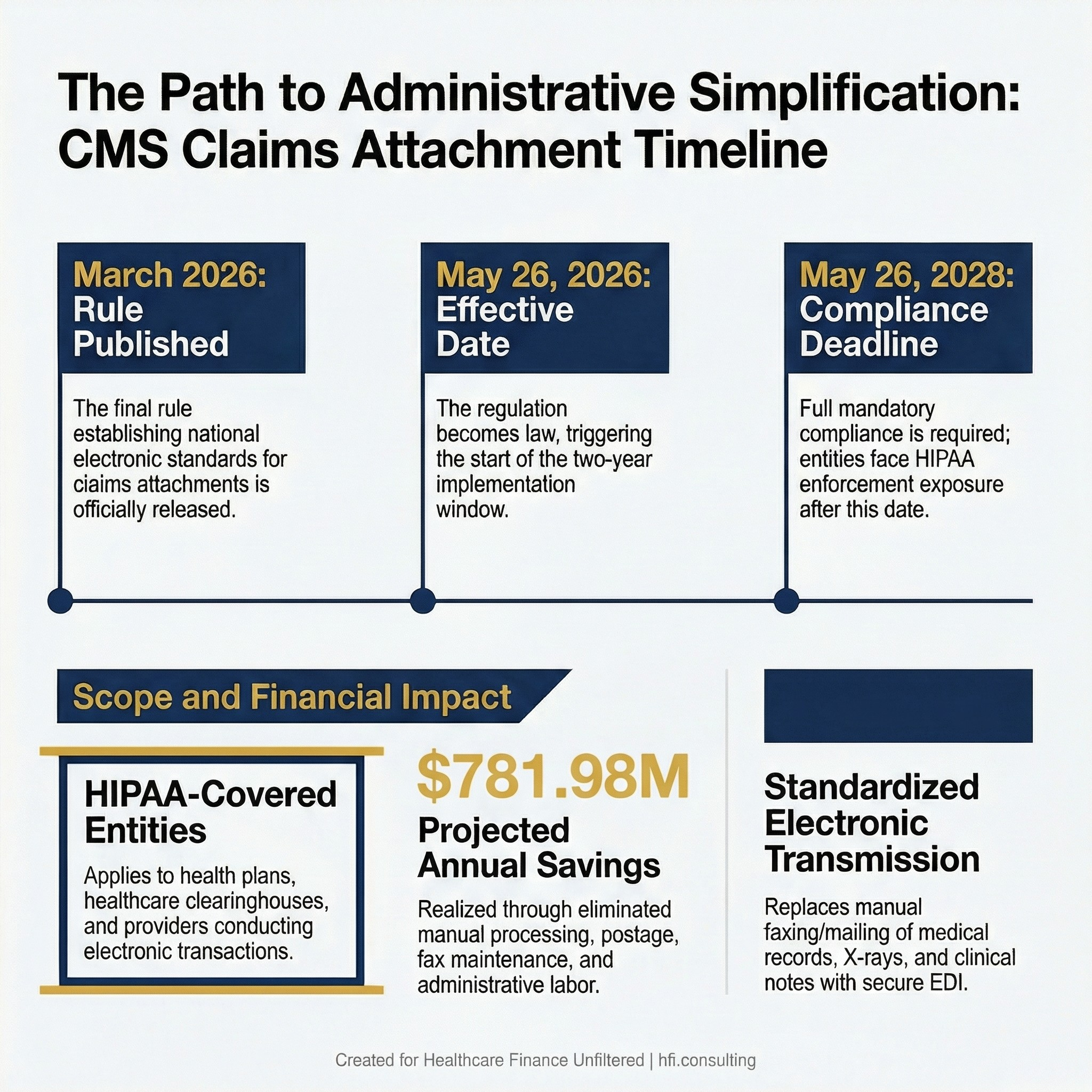
CMS Administrative Simplification Final Rule 2026 compliance timeline showing effective date May 26, 2026, and mandatory compliance deadline May 26, 2028, with $781 million projected annual savings
What the Rule Actually Does
The Administrative Simplification; Adoption of Standards for Health Care Claims Attachments Transactions and Electronic Signatures Final Rule was released March 20, 2026. It becomes effective May 26, 2026. Covered entities have until May 26, 2028 to fully comply.
The rule applies to all HIPAA-covered entities: health plans, healthcare clearinghouses, and healthcare providers that conduct electronic transactions. If your organization submits or processes claims, this rule applies to you.
The practical change is straightforward. Historically, when a health plan requested additional documentation to support a claim, providers responded by faxing or mailing medical records, X-rays, clinical notes, telemedicine visit documentation, and lab results. This rule establishes a national electronic standard for transmitting that same documentation. It also adopts standards for electronic signatures to ensure secure, authenticated transmission.
The $781 million in projected annual savings comes from eliminating manual processing costs, postage, fax line maintenance, and the administrative labor tied to managing paper-based documentation requests across the system.
Why This Time Is Different
CMS has been trying to kill the fax machine since at least 2018, when then-Administrator Seema Verma publicly called for providers to stop using fax at an ONC Interoperability Forum. That call generated headlines and little else.
What is different in 2026 is the regulatory infrastructure behind the mandate. The Advancing Interoperability and Improving Prior Authorization Final Rule established binding data exchange requirements. This week's rule layers claims attachment standards on top of that existing framework. The combination creates actual enforcement leverage rather than aspirational guidance.
The other difference is the format. This is a final rule, not a request for comment, not a proposed standard, and not a voluntary framework. Covered entities that fail to comply by May 26, 2028 face HIPAA enforcement exposure under the administrative simplification provisions.
For finance leaders who have fielded "we should really get off fax" conversations in planning meetings for years, the time horizon just became concrete.
The Budget Reality: Two Years to Transition
Two years sounds like ample runway. It is not, given the typical pace of healthcare technology procurement and implementation.
Most health systems will need to assess, procure, implement, and test electronic claims attachment solutions across all payer relationships before the May 2028 deadline. For organizations running multiple EHR platforms, managing legacy clearinghouse contracts, or operating across multiple states with varied payer mix, two years is workable but not comfortable.
From my work at Ascension across seven hospitals, I know firsthand how uneven technology adoption looks inside a multi-entity health system. The flagship facility may already have electronic transaction workflows in place. The smaller community hospitals on legacy platforms often do not. A compliance deadline that applies uniformly to the entire HIPAA-covered entity does not care about which campus is furthest behind.
Here is how to think about the budget planning in three categories.
Category 1: Technology Assessment and Procurement
If your organization does not already have an electronic claims attachment solution integrated into your revenue cycle workflow, you need one. This likely means evaluating your clearinghouse's current capabilities, your EHR vendor's roadmap for the new attachment standards, and whether any middleware solutions are necessary to bridge gaps.
Budget conservatively for implementation costs, staff training, interface build time, and testing against your top payers. Organizations that have recently navigated Epic or other major EHR upgrades will recognize this cost structure immediately.
Category 2: Staff Transition and Training
Eliminating fax does not eliminate the underlying workflow. Billing staff, HIM teams, and clinical documentation specialists who currently manage paper-based attachment requests will need retraining on electronic submission workflows. This is not purely a technology cost; it is a labor and change management cost.
For revenue cycle departments already managing tight staffing ratios, plan for a transition period where productivity dips before it improves.
Category 3: Vendor Contract Review
Your existing clearinghouse and claims processing vendor contracts may need renegotiation. Some vendors will charge implementation fees to enable new attachment standards. Others may require contract amendments. Review your current agreements now, before vendors are flooded with transition requests in 2027.
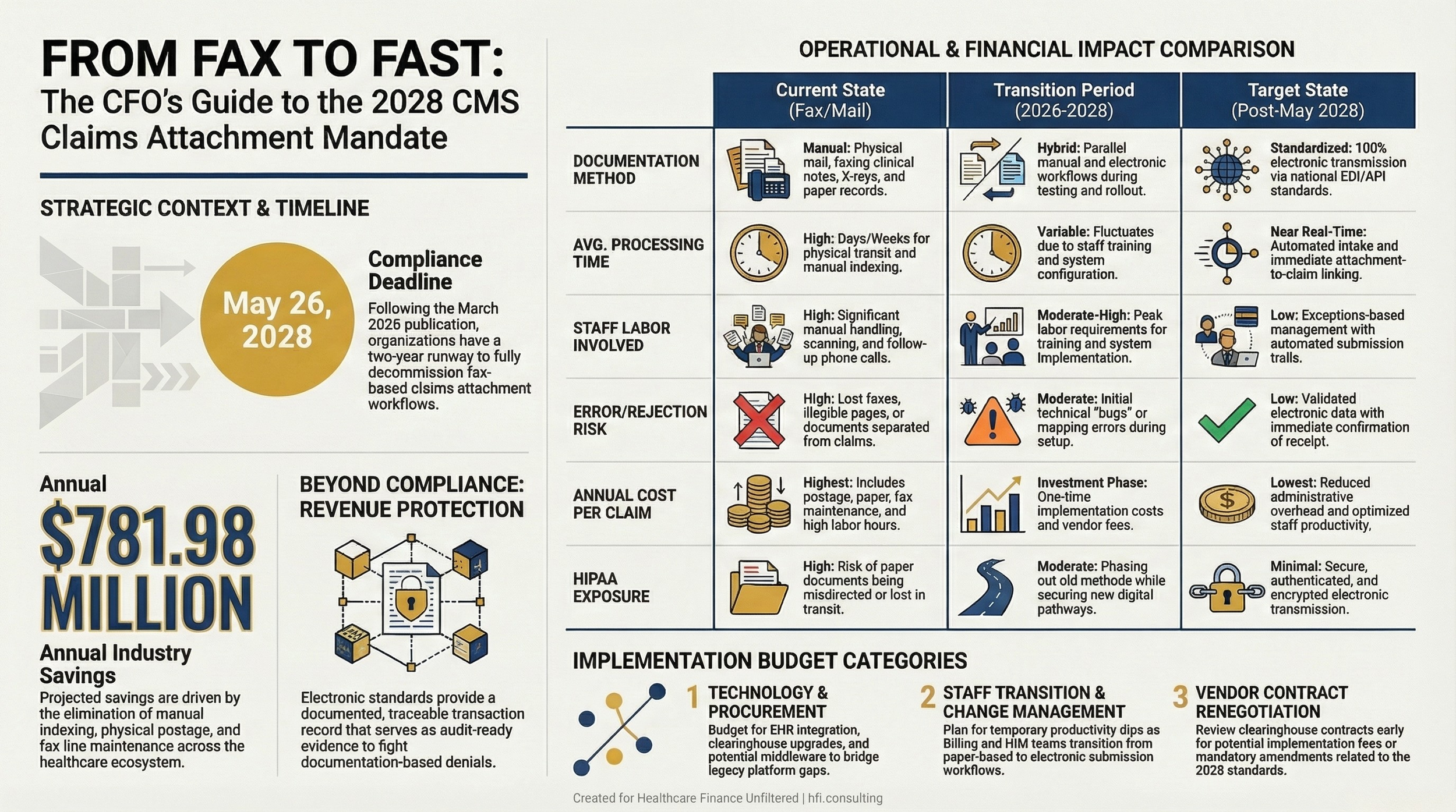
Comparison table showing current fax-based claims attachment process versus electronic standards-compliant process after CMS 2028 compliance deadline.
The Revenue Cycle Opportunity Inside the Mandate
Most of the public coverage of this rule focuses on the cost-saving headline. The more operationally interesting story is what happens to claims denial rates when attachments become electronic and standardized.
Fax-based attachments fail in ways that are difficult to track systematically. A fax goes to the wrong number. A document arrives partially. A clinical note gets separated from the claim it was meant to support. These failures generate denials, delay reimbursement, and create write-off risk that sits quietly in your AR aging without a clear root cause.
Electronic attachment standards create a documented, traceable transaction record. When an attachment is transmitted electronically under the new framework, there is a confirmation trail. That traceability changes your denial management posture because you can prove what was sent, when, and to whom.
For revenue cycle teams currently fighting payers on documentation denials, this shift creates both an opportunity and a higher-stakes environment. If your attachment process is clean and electronic, you have audit-ready evidence. If your process is not compliant by 2028, you have HIPAA exposure on top of your existing denial volume.
The math here matters for your CFO narrative. This is not just a compliance spend. It is a revenue protection investment.
What Payer Finance Leaders Need to Plan For
The mandate runs in both directions. Health plans must also comply with the new electronic claims attachment standards by May 2028.
For payer-side finance and operations leaders, this means updating member adjudication workflows to accept and process standardized electronic attachments, training clinical review teams on new documentation formats, and ensuring your technology vendors are building toward the new standards.
From my time at Florida Blue Medicare, I can tell you that the administrative cost of processing paper documentation through a utilization management workflow is substantial. The manual handling, imaging, indexing, and routing of faxed clinical records is labor-intensive in ways that are easy to underestimate when you are looking at it line-item by line-item on a staffing report.
The $781 million in projected savings is an industry-wide figure. The distribution of those savings will be uneven based on how much fax-based documentation volume your organization currently handles. Organizations with high prior authorization volume, large Medicare Advantage membership, or complex specialty referral workflows stand to capture disproportionate savings if they execute the transition well.
If you are building the internal business case to fund your claims attachment transition, I want to help.
Reply to this email with your biggest planning question — whether that is how to structure the vendor evaluation, how to present the ROI to your board, or where to start the gap assessment. I read every reply and respond.
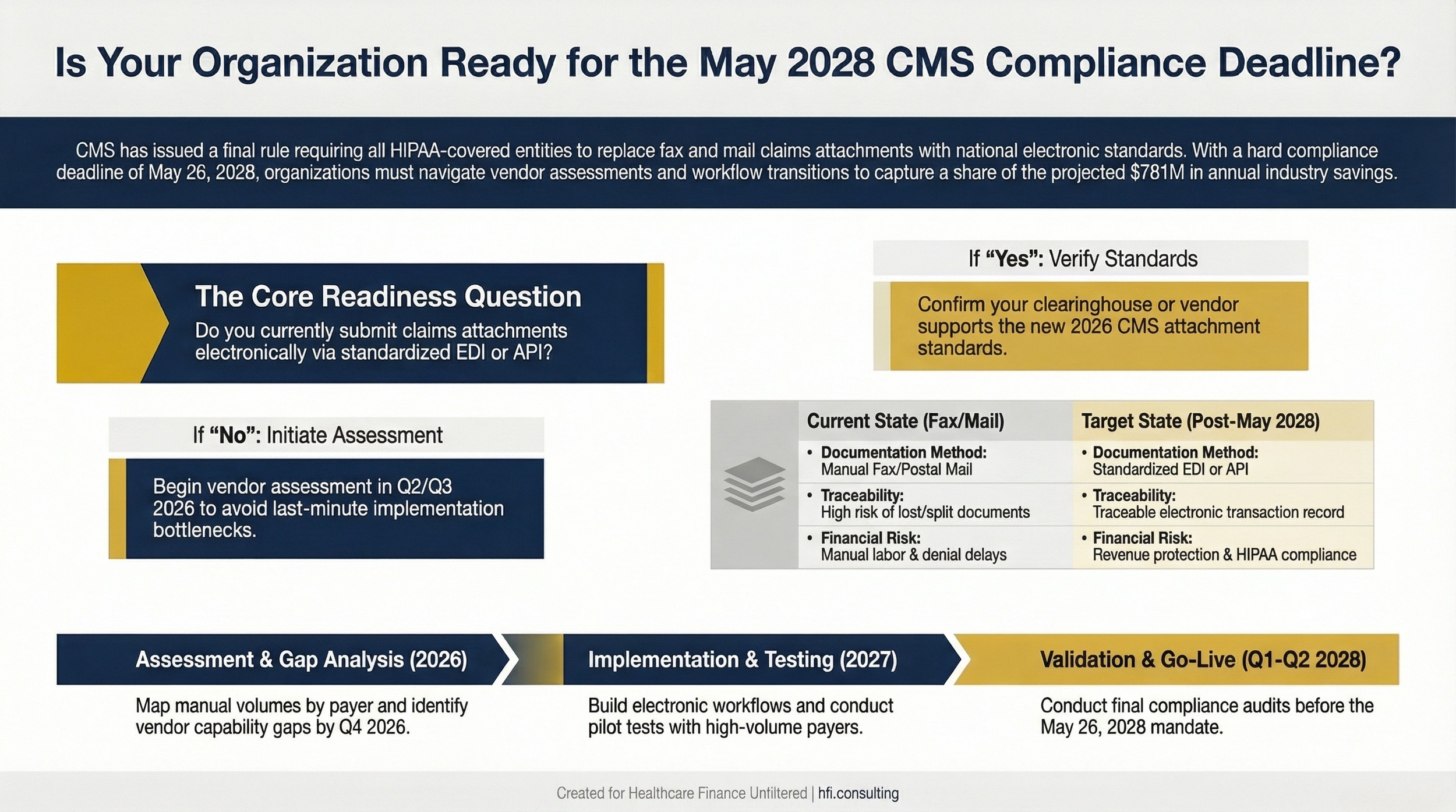
Decision flowchart helping hospital CFOs assess readiness for CMS claims attachment electronic standard compliance by May 2028.
A Practical Implementation Roadmap for Finance Leaders
The two-year window breaks down cleanly into four phases. This is a planning framework, not a vendor prescription. Your organization's specific technology environment and payer mix will determine the actual task list.
Phase 1: Assessment (Q2-Q3 2026)
Map your current fax and mail-based claims attachment volume by payer, service line, and facility. Identify which workflows are generating the most paper-based documentation requests. This is your baseline.
Engage your EHR vendor and clearinghouse to understand their current capabilities and their roadmap for the new attachment standards. Ask specifically: are they planning updates, and when? Get timelines in writing.
Review your top 10 payer contracts for any language related to documentation submission requirements. Flag any that could create friction during the transition.
Phase 2: Gap Analysis and Vendor Selection (Q4 2026)
Using your assessment baseline, identify the gaps between your current state and the new standards. This is where you build the budget request. Be specific: number of transactions affected, estimated labor hours currently spent on manual processing, technology costs to close the gap.
If your clearinghouse or EHR vendor cannot meet the standard by 2028, this is the phase where you evaluate alternatives. Do not wait until 2027 to have this conversation.
Phase 3: Implementation and Testing (2027)
Build, configure, and test the electronic attachment workflows with your major payers before going live broadly. Prioritize your highest-volume payers first. Document every test result.
Train your billing, HIM, and clinical staff. Build in a transition period where both old and new workflows run in parallel so you can catch problems before the fax workflow is decommissioned.
Phase 4: Compliance Validation and Go-Live (Q1-Q2 2028)
Before May 26, 2028, conduct a compliance audit. Confirm that all covered transactions are processing through electronic attachment workflows, that your signature standards are met, and that your documentation is audit-ready.
Build a post-go-live monitoring plan for the first 90 days to catch denial patterns that may indicate transmission failures.
For more on managing technology transitions in revenue cycle, see my earlier analysis of AI-Powered Revenue Leakage Prevention: The CFO's Implementation Guide for 2026.
The Broader Signal for Healthcare Finance
The CMS administrative simplification agenda is not finished with this rule. The prior authorization electronic mandate, the interoperability rules, and now the claims attachment standards are pieces of a connected regulatory framework designed to force the administrative layer of healthcare onto modern electronic infrastructure.
For CFOs building multi-year capital and operating budgets, the question is no longer whether healthcare will be forced off legacy administrative technology. It is when and at what cost.
The organizations that build electronic transaction infrastructure proactively, rather than reactively at mandated deadlines, will have lower transition costs and fewer operational disruptions. They will also have better data, because every electronic transaction creates a record that paper never could.
The fax machine's operating costs are easy to measure. The revenue cycle inefficiency it creates is harder to quantify but substantially larger. This final rule is, ultimately, a forcing function for a transition that most finance leaders already know needs to happen.
For context on how CMS compliance mandates affect broader financial risk, see my recent piece on CMS Medicaid Fraud Crackdown 2026: What Hospital Finance Leaders Must Do Now. The pattern of increased CMS enforcement activity in 2026 runs across multiple rule areas simultaneously. Finance leaders who treat each mandate as an isolated event are underestimating the cumulative compliance investment required this cycle.
Healthcare Finance Unfiltered covers regulatory changes like this one with a focus on what they mean for your budget, your operations, and your risk profile. If this analysis was useful, consider upgrading to a paid subscription for deeper dives, frameworks, and direct access.
P.S.
What is your organization's current state on claims attachment automation? Are you already running electronic workflows, or is the fax machine still grinding in the background? Hit reply and tell me where you are — I am genuinely curious how far along the industry actually is versus how far along CMS thinks we are.