
ACA Subsidy Expiration Is Reshaping Your Community Benefit Strategy: A 2026 CFO Playbook
When 1 in 10 marketplace enrollees lose coverage, your charity care budget and Schedule H obligations shift overnight.
A new KFF survey confirms what finance leaders should already be modeling: one in ten people who had ACA marketplace coverage in 2025 are now uninsured. That is not a rounding error. At a time when your operational margins are under sustained pressure, your charity care volume is about to move, and your IRS Schedule H obligations will reflect it.
This article is a planning framework for CFOs who need to connect national coverage trends to local budget impact and community benefit strategy, before the Q3 board meeting asks why uncompensated care is up.
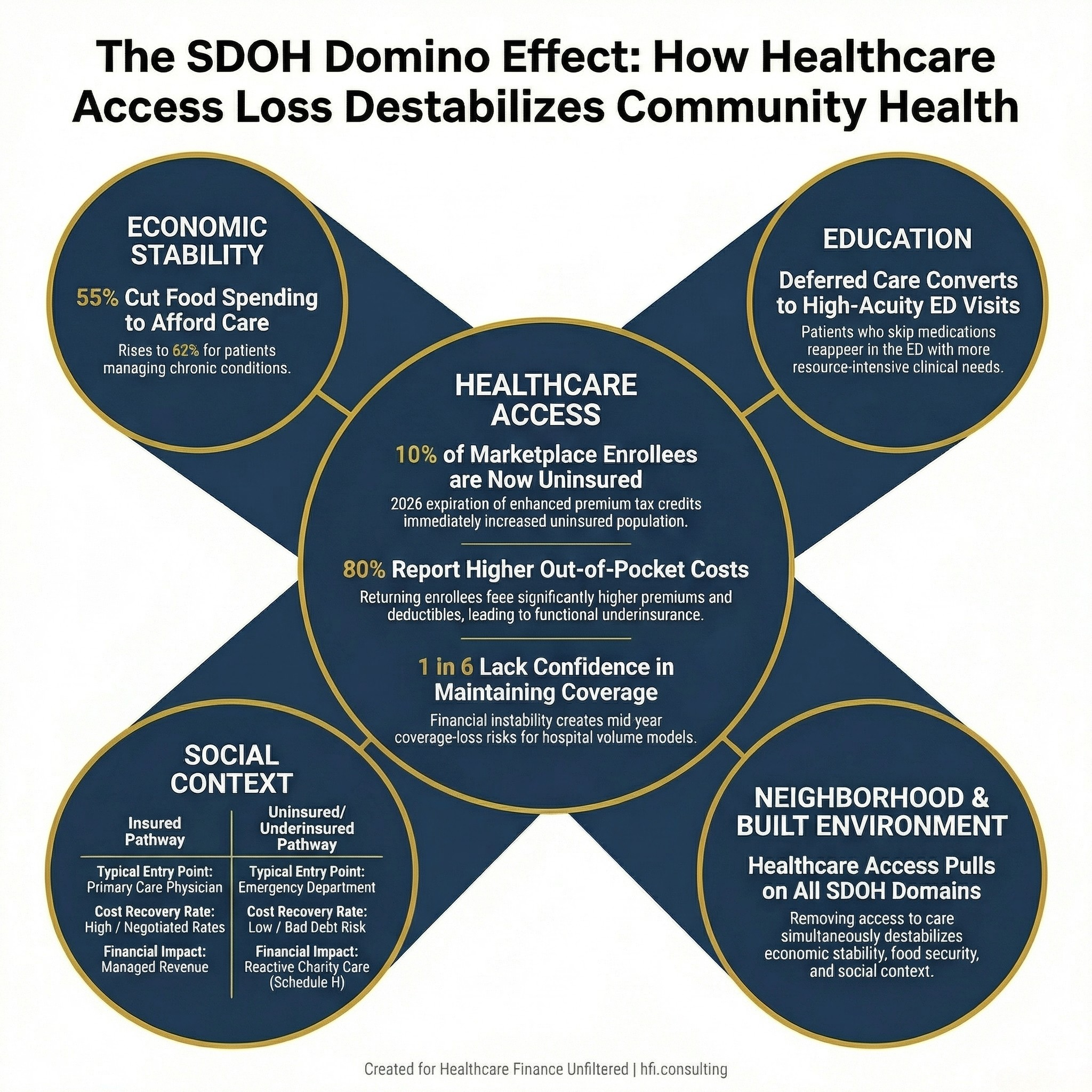
Diagram showing the five Healthy People 2030 social determinants of health domains with healthcare access highlighted to show cascade effects on other domains
The Coverage Cliff Is Already Behind Us
The enhanced premium tax credits that kept ACA marketplace premiums artificially lower expired at the end of 2025. Congress did not extend them. The result was immediate and measurable.
According to the KFF survey, 80 percent of returning marketplace enrollees report that their 2026 plan premiums, deductibles, or cost-sharing are higher than last year. One in six, representing 17 percent, say they are not confident they can afford their monthly premium for all of 2026.
That last figure should land hard for hospital finance leaders. A person who is uncertain they can keep their coverage all year is not a reliably insured patient. They are a coverage-loss risk in months four, six, or nine of the fiscal year.
The behavioral response is already visible in the data. A quarter of returning enrollees downgraded from Silver to Bronze plans to lower their premium. Bronze plans carry materially higher deductibles and out-of-pocket maximums. For a CFO modeling bad debt, this is not neutral. A patient with a $7,000 deductible on a Bronze plan is functionally underinsured for most elective and semi-elective services.
When Coverage Disappears, SDOH Doesn't Wait
Social determinants of health are the conditions in the environments where people are born, live, learn, work, and age, conditions that shape health outcomes at least as much as clinical care itself. Healthy People 2030 organizes SDOH into five domains: economic stability, education access and quality, healthcare access and quality, neighborhood and built environment, and social and community context.
Healthcare access is one domain. But it does not operate in isolation.
The KFF data makes the cascade visible. Among returning marketplace enrollees, 55 percent say they are cutting back spending on food or basic household items to afford their coverage and care. For those managing chronic conditions, the number climbs to 62 percent.
Food insecurity is an SDOH. Housing instability is an SDOH. A person who stops buying medications to pay a premium, or skips a follow-up visit because the deductible has reset, does not simply disappear from the healthcare system. They reappear later, sicker, in your emergency department, where cost recovery is structurally more difficult and clinical stabilization is more resource-intensive.
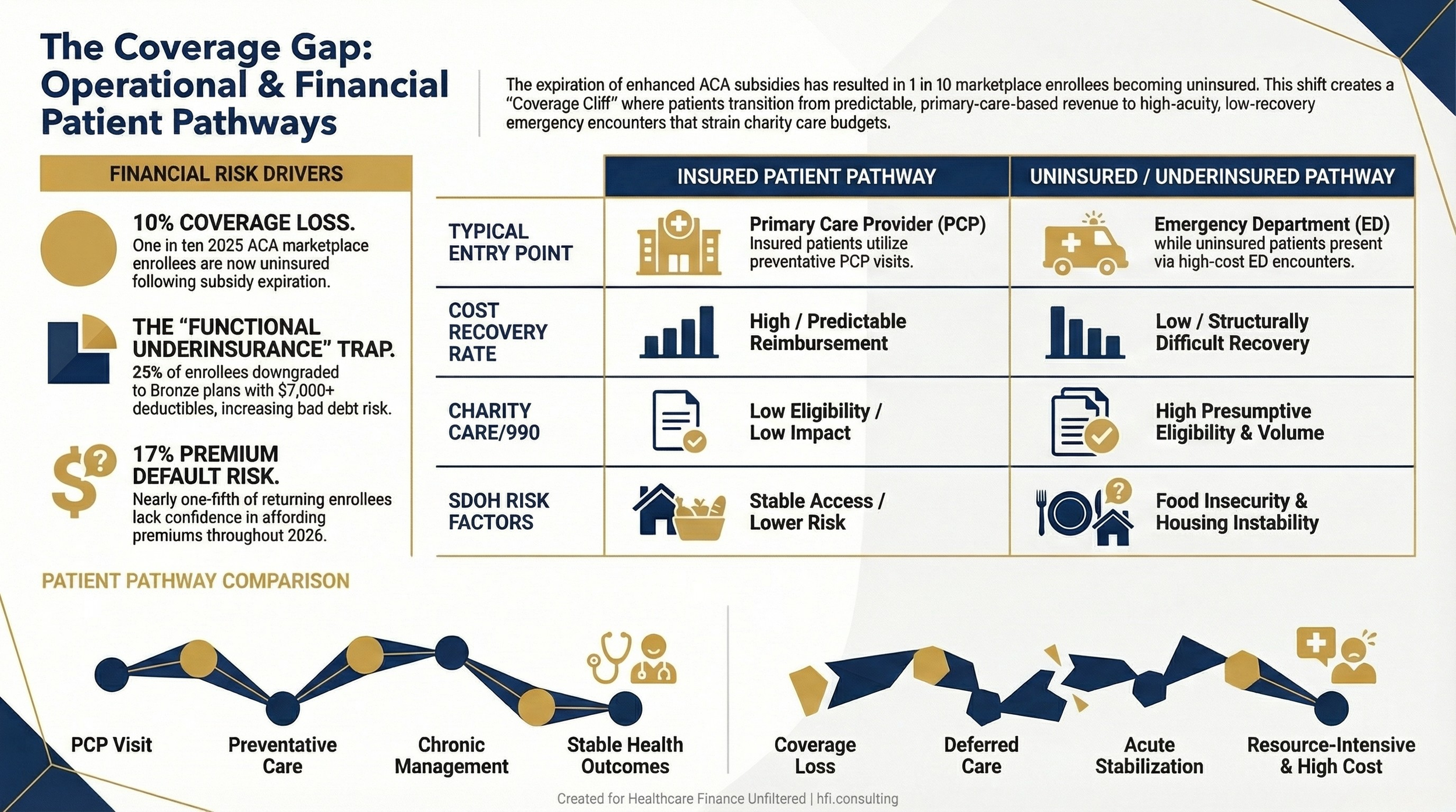
Comparison table showing the financial and clinical pathway differences between insured patients accessing primary care versus uninsured patients presenting to the emergency department
What This Means for Community Benefit Obligations
Every nonprofit hospital files IRS Form 990, Schedule H. Community benefit reporting is not voluntary. The categories are defined: charity care at cost, community health improvement services, health professions education, subsidized health services, research, and cash and in-kind contributions to community organizations.
What often gets managed reactively is charity care volume. When coverage rates in your service area decline, charity care applications increase. Your financial counselors field more Medicaid presumptive eligibility requests. Your charity care policy comes under scrutiny from state regulators and, increasingly, from CMS.
The current environment creates two distinct planning problems.
The near-term problem is volume. The 10 percent of 2025 ACA enrollees who are now uninsured did not stop having healthcare needs. They deferred them. Deferred primary care converts to higher-acuity presentations. Deferred diabetes management converts to DKA admissions. Deferred hypertension follow-up converts to stroke. These are predictable clinical and financial patterns, and your volume model should reflect them.
The medium-term problem is strategy.** Community benefit that is purely reactive, documenting what was spent on charity care after the fact, is a compliance posture, not a strategy. Health systems that are building durable community benefit programs are investing upstream in SDOH interventions that reduce future utilization.
At Florida Blue Medicare, I watched how gaps in food security, transportation, and social support directly drove MA member utilization patterns. Members who lacked stable housing or consistent food access were significantly more likely to generate high-cost encounters, often preventable ones. That dynamic does not change when the patient is on a marketplace plan instead of Medicare Advantage.
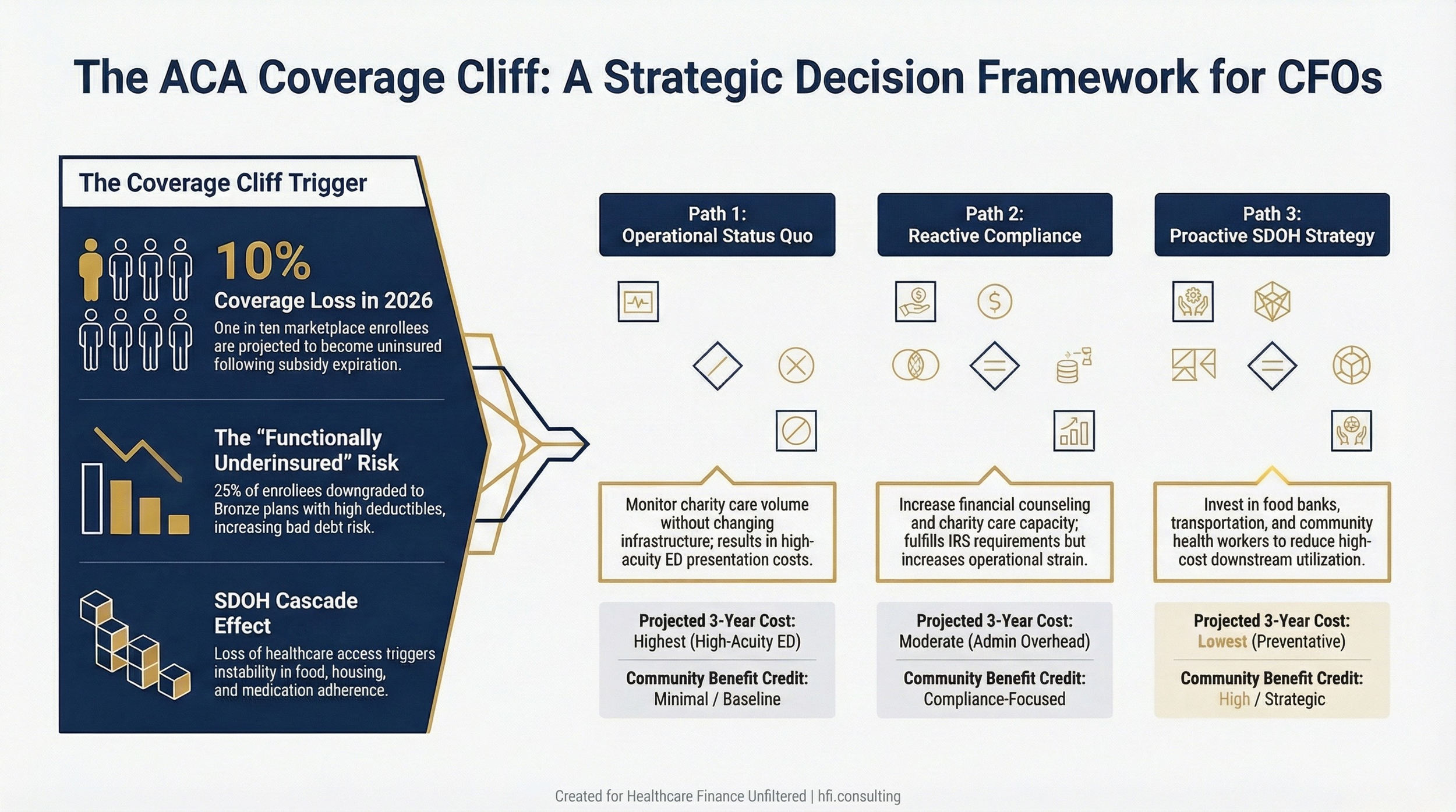
Decision flowchart showing three strategic pathways for hospital CFOs responding to ACA coverage loss in their service area, comparing reactive and proactive community benefit approaches
Rethinking Schedule H as a Strategic Tool
Most finance teams approach Schedule H as a documentation exercise. The goal is to demonstrate that the organization's community benefit spend justifies its tax-exempt status. That framing is defensible but limited.
The organizations that use Schedule H most effectively treat it as a strategic planning input. The question is not just "what did we spend?" but "what did we spend it on, and is that allocation matched to the SDOH profile of our service area?"
A hospital in a county where 15 percent of the population recently lost ACA coverage, where food insecurity rates are elevated, and where transportation to primary care is limited, has a clear argument for allocating community benefit dollars toward community health improvement services rather than concentrating them in financial assistance programs alone.
Community health improvement services, including community health education, health screenings, and subsidized community health worker programs, carry full Schedule H credit. They also generate data. Structured SDOH screening programs, embedded in patient registration workflows or run through community health worker outreach, create the documentation trail that supports both your community health needs assessment and your regulatory position.
This matters right now because the IRS has increased scrutiny of nonprofit hospital community benefit reporting, and several state legislatures are revisiting the standards for what qualifies as adequate community benefit in exchange for property tax exemption.
The CFO's Near-Term Checklist
Before the end of Q2, your finance team should have answers to the following questions.
How many patients in your service area are projected to have lost ACA coverage between 2025 and 2026? State insurance department data, KFF county-level estimates, and your own payer mix trend will triangulate to a reasonable number. Build it into your volume model for the back half of fiscal year 2026.
Is your charity care policy aligned with the current environment? A policy calibrated for a higher-coverage environment may screen out patients who now qualify. Review your Federal Poverty Level thresholds and your presumptive eligibility workflow.
What is your SDOH screening penetration rate? If you are operating an SDOH screening program and it is capturing fewer than 50 percent of eligible patients, you have a documentation gap and a care coordination gap simultaneously. Both carry financial consequences.
Are your community benefit dollars aligned with your community health needs assessment findings? The CHNA is required every three years. If yours is more than 18 months old and your service area's coverage profile has shifted materially, you have a narrative problem if regulators ask why your community benefit spending does not reflect community need.
What the Next 12 Months Look Like
The 17 percent of returning enrollees who are not confident they can maintain coverage all of 2026 represent a mid-year risk. Coverage lapses tend to accelerate when renewal periods arrive or when a financial shock, a job loss, an unexpected medical bill, forces a choice. Your volume projections should include a mid-year scenario where uninsured presentation rates increase 8 to 12 percent in the second half of fiscal year 2026.
On the payer side, this environment creates a renegotiation opportunity that finance leaders should not overlook. Several regional insurers and managed Medicaid plans are actively expanding their Medicaid and community-based care models. If your health system is not already in those conversations, the ACA coverage cliff creates a natural entry point for discussions about community health partnerships, value-based arrangements, and care management contracts that carry a community benefit dimension.
In my work across multiple health systems, the CFOs who navigated coverage volatility most effectively were the ones who had built relationships with their regional insurance counterparts before the crisis, not during it.
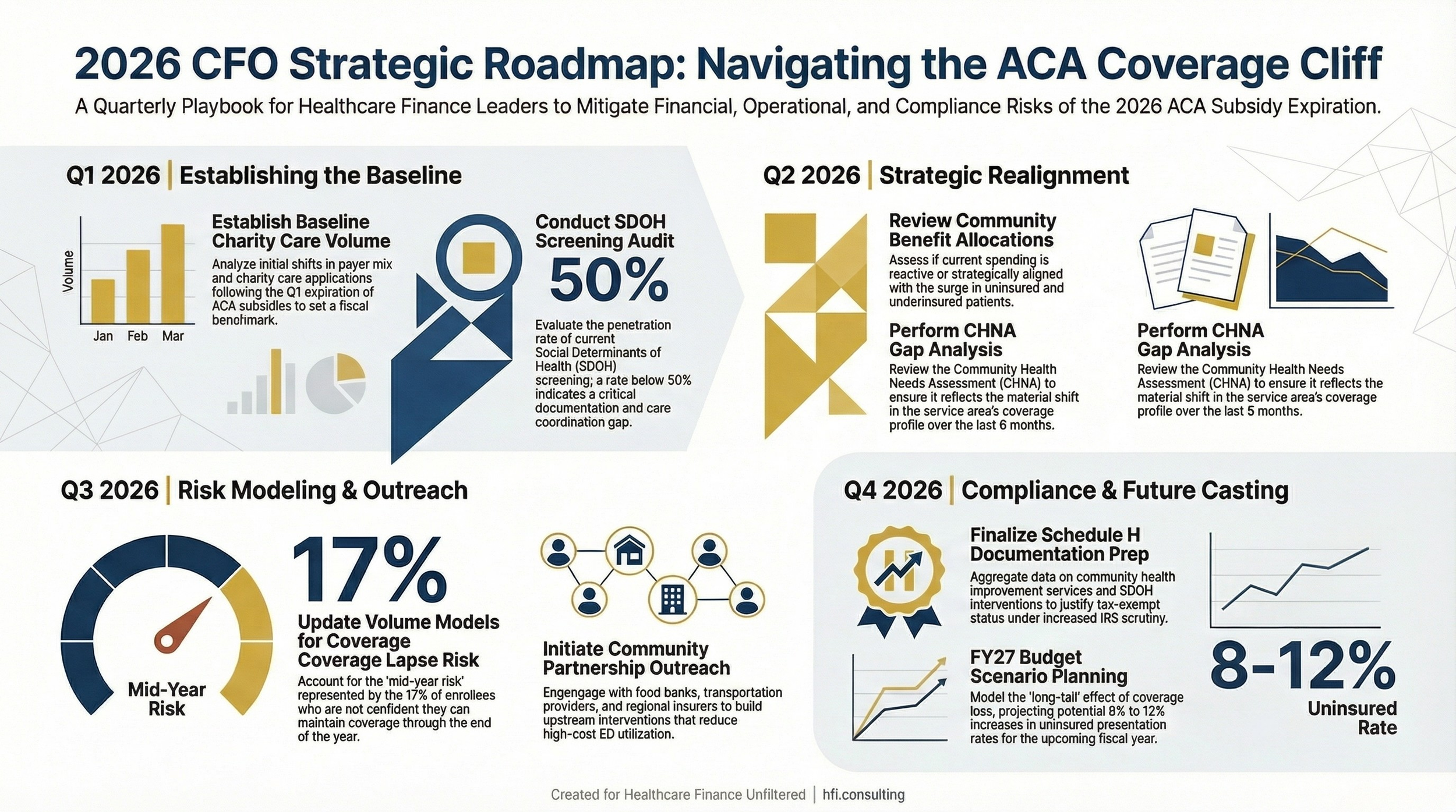
Twelve-month planning timeline showing quarterly milestones for hospital CFOs managing the community benefit and volume impact of ACA subsidy expiration through fiscal year 2026
The Bigger Picture for Healthcare Finance Leaders
The ACA subsidy expiration is one data point in a larger pattern. Medicaid redeterminations removed millions from coverage over the past two years. The enhanced premium tax credits are gone. Legislative proposals for alternative coverage vehicles, including health savings account expansions and the framework outlined in the Great American Healthcare Plan, are not yet enacted and carry significant uncertainty.
What is not uncertain is the SDOH mechanism. Research consistently shows that removing one determinant of health, access to coverage, produces measurable downstream effects across other domains within 12 to 24 months. Food insecurity increases. Housing instability increases. Behavioral health utilization increases. Chronic disease management deteriorates.
For your patients, this is a health equity issue. For your balance sheet, it is a volume, payer mix, and bad debt issue. For your Schedule H, it is a strategic alignment issue. The CFOs who treat all three as connected, rather than managing them in separate workstreams, will be better positioned when the audit comes and when the board asks why uncompensated care is up.
For more context on how the ACA subsidy expiration is affecting revenue cycle planning, see Alternative Health Plans After ACA Subsidy Expiration: Revenue Cycle Impact Guide and The ACA Subsidy Reckoning: When Government Spending Meets Financial Reality. For CFOs managing coverage volatility alongside Medicaid uncertainty, Rural Hospitals Already in the Red: How Medicaid Changes Will Push Them to the Brink and Hospital Facility Fees Under Siege: CFO Playbook for the $172 Billion Medicaid Cut provide complementary planning frameworks.
If you are building a community benefit strategy for 2026 and want a framework for aligning Schedule H spend with SDOH data in your service area, reply to this email and tell me what you are working with. I will send back a short framework tailored to your situation.
This Is Not a Policy Debate. It Is a Planning Requirement.
Finance leaders who are waiting for legislative clarity before updating their community benefit strategy or volume models are taking on unnecessary planning risk. The coverage data is current. The SDOH research is settled. The Schedule H filing is annual.
The question is not whether your uninsured volume will increase. It is whether your operational plan is built around that reality.
If you are a CFO at a safety net or community hospital with a high Medicaid and uninsured mix, the projections are more acute. If you are at a regional health system with a diversified payer mix, the effect is smaller but not absent. In either case, the community benefit strategy should reflect what the data now shows.
Build the model. Run the scenarios. Document the spend. And if your community health needs assessment is due in 2026 or 2027, start that process now, because the coverage environment you document this year will shape what regulators and community members expect from your organization for the next three.
Healthcare Finance Unfiltered covers the financial and operational implications of coverage policy for CFOs and health system finance leaders. Subscribe at hfi.consulting to receive the full analysis as it publishes.
P.S. What is the biggest gap in your current community benefit planning process: volume forecasting, SDOH data infrastructure, or Schedule H strategy? Hit reply and let me know. Your answer may shape a future article.