
Health System Cost Control in 2026: What Still Works, What Needs Updating, and What CFOs Should Do Now
The Advisory Board's 20-tactic framework is still useful, but three of its core recommendations need a serious update for today's margin reality.
Hospital operating margins averaged 2.3% in 2024, according to Kaufman Hall. That is not a typo, and it is not a trend that reverses itself without deliberate action at the finance leadership level. If you are walking into your next board meeting without a structured cost discipline framework, you are already behind.
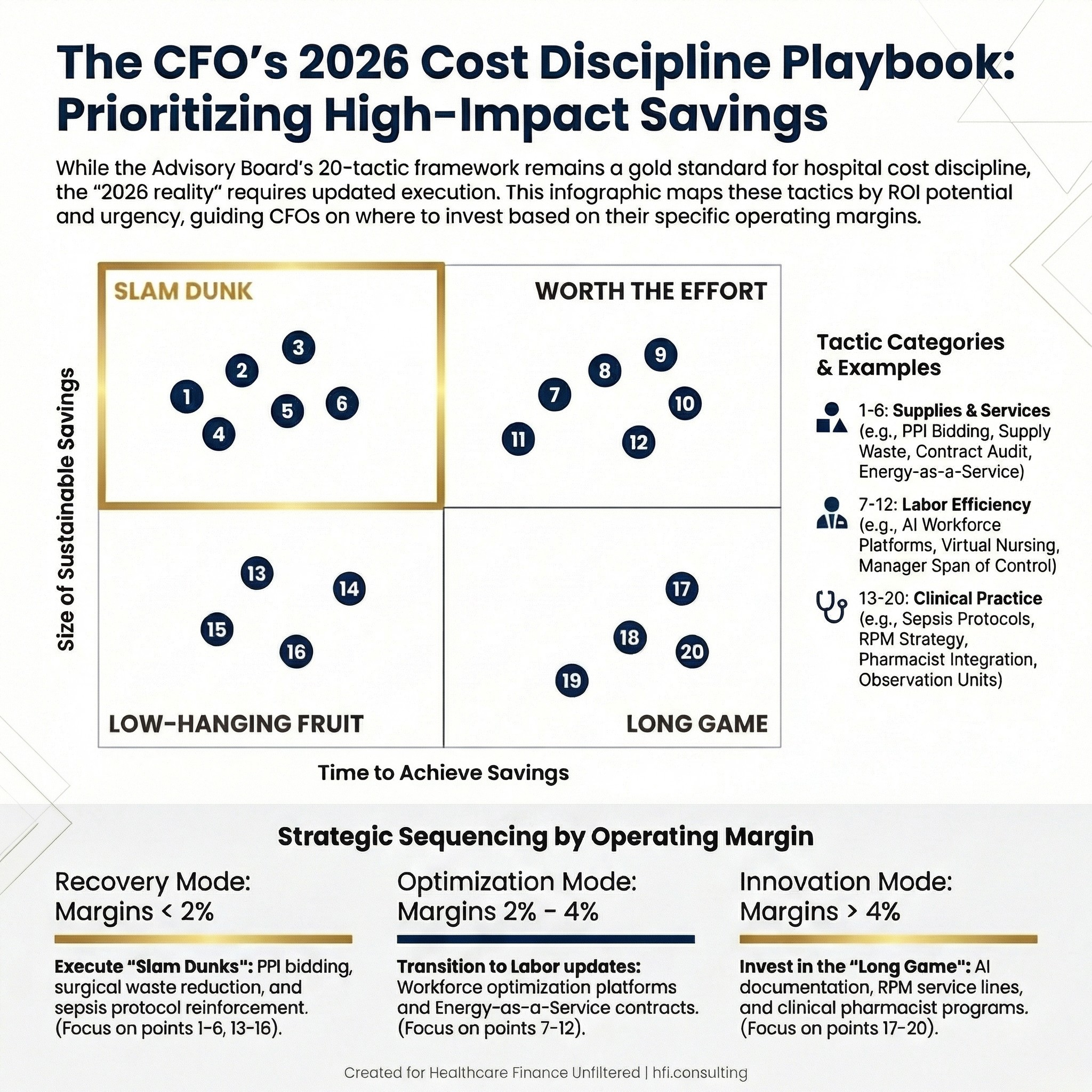
A 2x2 quadrant matrix showing 20 health system cost-saving tactics mapped by time to achieve savings and size of sustainable savings, with slam dunk tactics highlighted in the upper left quadrant
Why This Framework Still Matters (And Where It Falls Short)
The Advisory Board published a landmark list of 20 cost-saving tactics for health systems that quickly became a reference document for CFOs and finance teams across the country. The logic was sound: stop reacting to every cash crunch with cuts and build systematic, sustainable cost discipline instead.
That framework holds up. What does not hold up is applying every recommendation exactly as written in 2026.
Three years of healthcare inflation, post-pandemic labor normalization, AI tool proliferation, and CMS reimbursement restructuring have changed the implementation calculus for several of these tactics. Some are now more urgent than they were when first published. A few need significant updating before you hand them to your VP of Supply Chain or your Chief Nursing Officer.
This article walks through all 20, flags which ones are ready to implement today, and digs into the honest pros, cons, and implementation complexity for the ones that matter most to your bottom line right now.
The Framework at a Glance
The Advisory Board organized the 20 tactics across three categories: Supplies and Services, Labor Efficiency, and Clinical Practice. They also mapped each tactic on a matrix showing time to achieve savings versus size of sustainable savings, with four quadrants: Slam Dunk, Worth the Effort, Low-Hanging Fruit, and Long Game.
That quadrant logic is still the right starting mental model. Where you are in your margin recovery cycle determines which quadrant you should be prioritizing. A health system at 1% operating margin needs slam dunks. A system at 4% with stable liquidity can invest in long-game tactics.
Here is a quick summary before we go deeper:
Supplies and Services (Tactics 1-6): Largely still valid. Direct contracting and PPI bidding strategies remain among the highest-ROI moves a CFO can make with relatively low implementation friction. Energy savings has evolved significantly and now includes financing structures that were not available in 2023.
Labor Efficiency (Tactics 7-12): This is the category that needs the most updating. The workforce landscape in 2026 is materially different from 2023, and two of the six labor tactics require a complete reframe before they are useful guidance.
Clinical Practice (Tactics 13-20): Mostly still sound. Sepsis protocols, blood utilization, and pharmacist integration remain high-value, evidence-backed interventions. Remote patient monitoring has evolved dramatically and requires a 2026 lens to implement correctly.
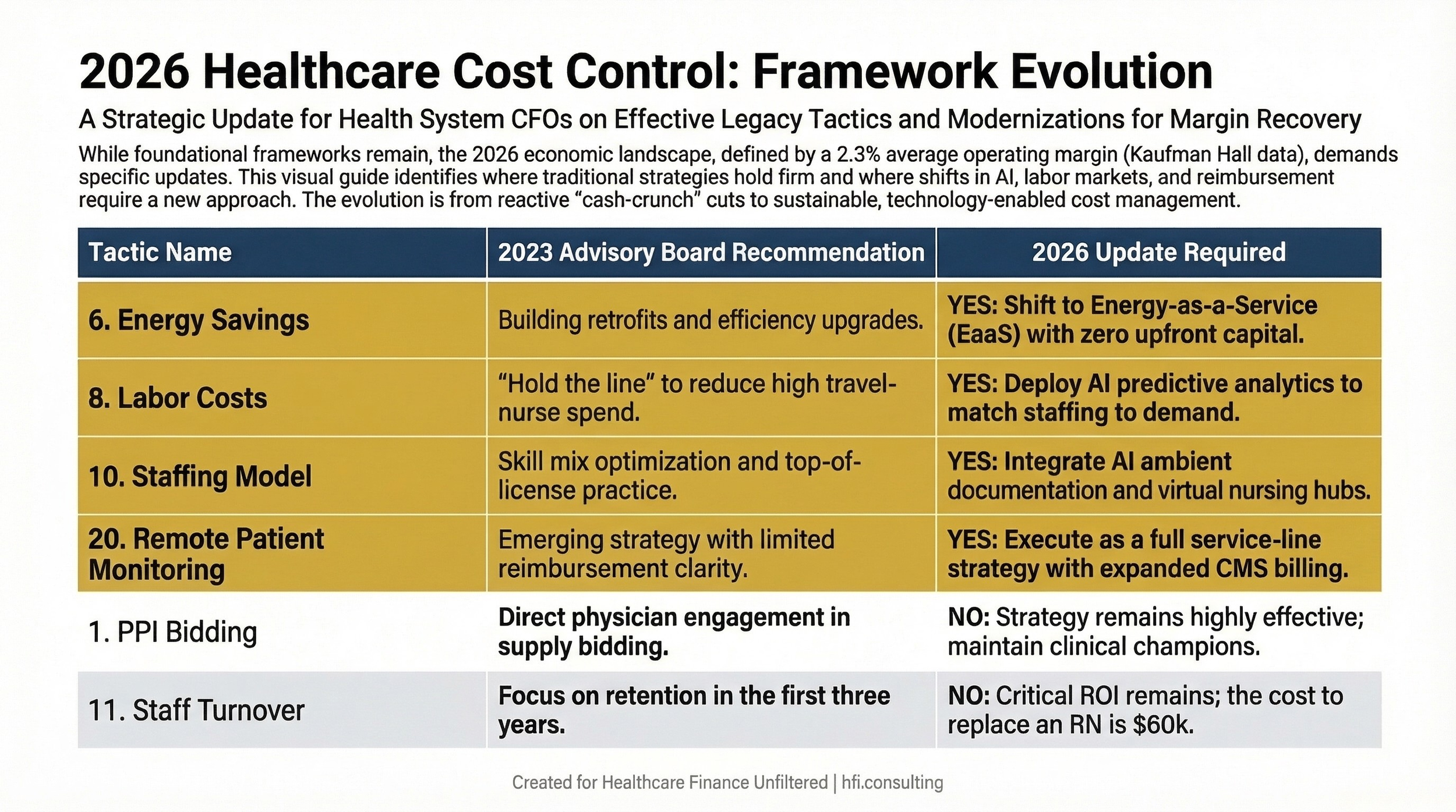
A three-column comparison table showing 20 health system cost control tactics, the original 2023 Advisory Board guidance, and whether a 2026 update is required for each
Supplies and Services: Still Solid, One Major Update
Tactic 1: PPI Bidding Strategy
Still highly relevant. Physician preference items, particularly implants in orthopedics and spine, represent one of the largest controllable cost variables on a hospital's supply expense line. Engaging physicians in the bidding process through clinical champions who share unblinded cost and quality data remains one of the best documented cost-reduction plays in healthcare finance.
The honest implementation challenge: Physician culture resistance is real. In my work tracking supply chain costs across seven hospitals at Ascension, the systems that made the most progress on PPI costs were the ones where finance leaders built direct relationships with department chairs, not just OR directors. You need a physician champion who is willing to sit across the table from their colleagues and make the case on the data. That person is harder to find than the strategy itself.
Verdict: Slam dunk, but only if you have the physician relationship infrastructure to support it.
Tactic 2: Surgical Supply Waste Prevention
Still relevant. Color-coding procedure preference cards and monitoring discarded supply data are straightforward operational wins. The implementation friction is low, and the savings accumulate quickly in high-volume surgical programs.
Tactic 3: Minimize PPI Contract Savings Leakage
Still relevant. This is the unsexy enforcement side of tactic 1. Having a contract is not enough. Limiting vendor rep access in the OR and holding physicians accountable to contracted products requires ongoing attention. This is a process management problem as much as a cost problem.
Tactic 4: Revisit Unfavorable Contract Terms
Still relevant, and more urgent. Supply chain inflation from 2021 through 2023 locked many systems into contracts that no longer reflect market reality. If you signed multi-year agreements during that period without renegotiation triggers, now is the time to audit those terms. Most contracts have provisions for early renegotiation that finance teams do not exercise.
Tactic 5: Direct Contracting for Clinical Preference Items
Still relevant. GPOs serve a purpose for commodity supply categories, but they are structurally disincentivized to find the lowest price on preference items. For any service line where volume is high enough to support a direct relationship, direct contracting consistently outperforms GPO pricing.
Tactic 6: Energy Savings
Updated recommendation needed. The original guidance focused on building optimization and retrofits achieving 10% to 26% in energy cost reduction. That math still holds, but the financing vehicle has changed.
In 2026, energy-as-a-service (EaaS) contracts allow health systems to execute major energy infrastructure upgrades with no upfront capital requirement. The vendor funds installation and is repaid through a share of the energy savings. For capital-constrained systems, this changes the calculus entirely. Onsite solar generation and battery storage paired with demand response programs have also matured to the point where they belong in your capital planning conversation alongside traditional efficiency upgrades.
Updated advice: Do not just model retrofit costs. Model EaaS contracts against your current energy spend and evaluate solar-plus-storage feasibility based on your facility footprint and state utility incentives.
Labor Efficiency: The Category That Needs the Most Work
Tactic 7: Employee Health Cost Accountability
Mostly still valid, with new complexity. Wellness incentive programs for self-insured employers remain effective for cost containment, but two issues have emerged since 2023. First, GLP-1 coverage decisions are now a material cost driver that most wellness program frameworks did not anticipate. Second, mental health parity enforcement has tightened, and plan designs that create barriers to behavioral health access now carry regulatory exposure.
Practical advice: Review your wellness incentive structure with your benefits counsel before assuming it is reducing costs without creating liability.
Tactic 8: Hold the Line on Labor Costs
This advice needs a complete reframe for 2026. The original guidance was written during the peak of pandemic-era workforce shortages, when health systems were paying travel nurse rates of two to three times normal in a desperate attempt to maintain census. The framing at the time was essentially: stop the bleeding.
The labor market has shifted. Travel nurse rates have normalized significantly. Permanent nursing vacancy rates have improved at most health systems. The imperative now is not to hold the line on costs but to rightsize labor spend using tools and strategies that were not available in 2023.
Updated recommendation: Invest in AI-driven workforce management platforms that use predictive analytics to match staffing to patient demand in real time. Platforms in this category have demonstrated 5% to 12% reductions in premium pay through better schedule optimization and float pool management. Pair this with a structured international nurse pipeline if your market supports it, not as a crisis measure but as a deliberate long-term workforce strategy.
The CFO's role in this updated tactic is different from what the original framing implied. You are not just holding a cost line. You are building a data infrastructure that lets you stop making staffing decisions based on manager intuition and start making them based on predictive models.
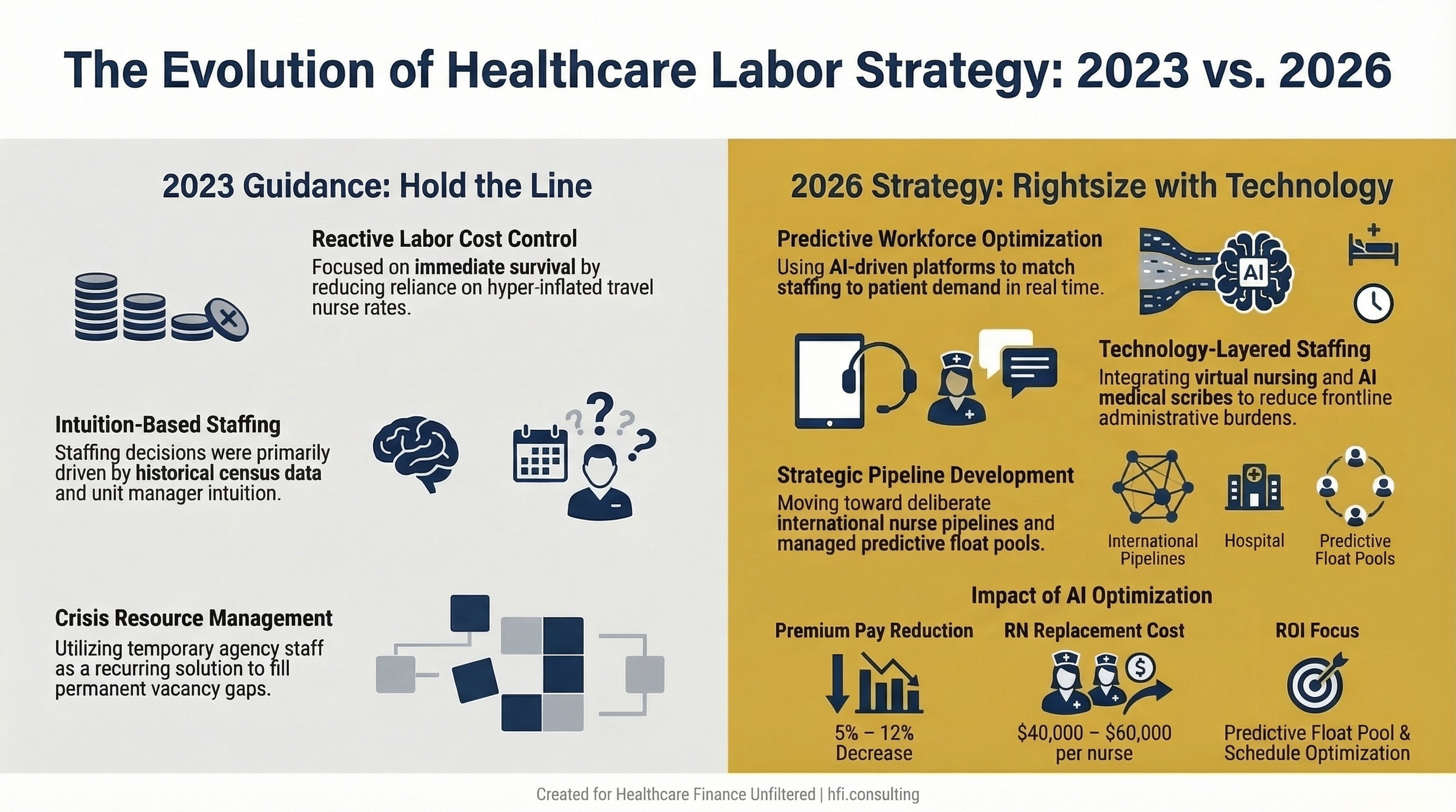
A side-by-side comparison showing the outdated 2023 "hold the line" labor cost strategy on the left versus the 2026 AI-driven workforce optimization approach on the right
Tactic 9: Revisit Manager Span of Control
Still relevant. Healthcare management structures remain heavily weighted toward small spans of control at the top of the organization. Most health systems have room to reduce management layers without affecting frontline care quality, particularly in administrative and support functions.
Tactic 10: Build a Value-Driven Staffing Model
Significantly evolved. Top-of-license practice and skill mix optimization remain valid goals. What has changed is the tool set available to support them.
In 2026, AI medical scribes and ambient documentation tools are mainstream in the organizations that have adopted them, and they demonstrably reduce the administrative burden on physicians and advanced practice providers. Virtual nursing programs, where RNs at a central hub manage documentation and non-direct-care tasks for multiple rooms simultaneously, have shown promising results in early adopters.
Updated recommendation: Your staffing model conversation now has to include a technology layer. The question is not just which roles do which tasks. It is also which tasks can be supported or replaced by AI-assisted tools, freeing clinical staff to work at the top of their training.
Tactic 11: Stop Junior Staff Turnover in the First Three Years
Still highly relevant and arguably more important now. The cost to replace a bedside RN has been estimated at $40,000 to $60,000 when you factor in agency coverage, training, and productivity ramp. That number has not gone down. Early-career retention programs including structured preceptorship, internal mobility pathways, and manager coaching remain among the best ROI investments a CFO can support.
Tactic 12: Tie Compensation to Enterprise Performance
Still valid. Incentive compensation aligned to operational cost targets and margin performance creates accountability at the department and service line level. The caution is in design: poorly structured incentive compensation that rewards volume without accounting for total cost of care can undermine the broader cost discipline you are building.
Clinical Practice: Mostly Sound, One Major Update
Tactics 13-16: Sepsis Protocols, Blood Utilization, ED Pharmacist, Discharge Ownership
All four of these remain valid, evidence-backed interventions with clear ROI. Sepsis remains a top driver of avoidable cost and mortality. Blood utilization protocols are frequently outdated and worth a dedicated audit. An ED-based pharmacist is one of the most consistently documented cost-per-dollar investments in clinical operations. Discharge process ownership directly reduces avoidable readmissions, which carry both cost and quality implications.
None of these need updating. If you have not implemented them, they should be on your near-term priority list.
Tactics 17-18: Multimodal Pain and Pharmacist Integration
Both still valid. Pharmacist integration into cross-continuum care has one of the most compelling ROI profiles in clinical operations, with documented returns of $12 for every dollar invested in one trauma center model. Multimodal pain management reduces opioid dependence risk while lowering per-patient medication costs.
Tactic 19: Observation Units for Low-Cost Short-Stay Patients
Still relevant, with one important caveat. The reimbursement gap between observation and inpatient status remains a financial reality. Dedicated observation units do reduce cost per episode compared to treating observation patients in fully staffed inpatient units.
The caveat: CMS continued to refine its two-midnight rule enforcement through 2024 and 2025. Your finance and clinical documentation teams need to be aligned on the compliance requirements for observation versus inpatient classification before you scale this strategy. Miscategorization carries both revenue risk and audit exposure.
Tactic 20: Remote Patient Monitoring
Major update required. When this was written in 2023, remote patient monitoring was an emerging strategy with limited CMS reimbursement clarity. The landscape in 2026 is materially different.
CMS significantly expanded RPM billing codes and reimbursement in its 2024 and 2025 Physician Fee Schedule updates. Wearable technology including continuous glucose monitors, cardiac event monitors, and pulse oximetry devices now integrate directly with EHR platforms in ways that make clinical workflow adoption realistic rather than aspirational. AI-driven alert systems reduce alarm fatigue by triaging patient data before it reaches a clinician.
Updated recommendation: RPM is no longer a pilot program question. It is a service line strategy question. The decision framework for your organization should include: which high-risk populations generate the most avoidable admissions, which conditions have reimbursable RPM codes, and what your care coordination capacity looks like to act on incoming patient data. The organizations that have operationalized RPM effectively treat it as a revenue cycle and care management conversation simultaneously, not just a technology implementation.
Where to Start: A CFO Prioritization Framework
Not every health system can pursue all 20 tactics simultaneously. Here is a practical sequencing framework based on margin position:
If your operating margin is below 2%: Focus on slam-dunk tactics first. PPI bidding, surgical supply waste, direct contracting for preference items, blood utilization, and sepsis protocol reinforcement. These generate savings within one to two fiscal quarters and require relatively low capital investment.
If your operating margin is 2% to 4%: Layer in the labor tactics with updated framing. Workforce optimization platforms, early-career retention investment, and span of control review. Begin evaluating EaaS energy contracts and remote patient monitoring business cases.
If your operating margin is above 4%: You have capacity to pursue the long-game investments. Value-driven staffing model redesign incorporating AI tools, full RPM service line strategy, and integrated pharmacist programs.
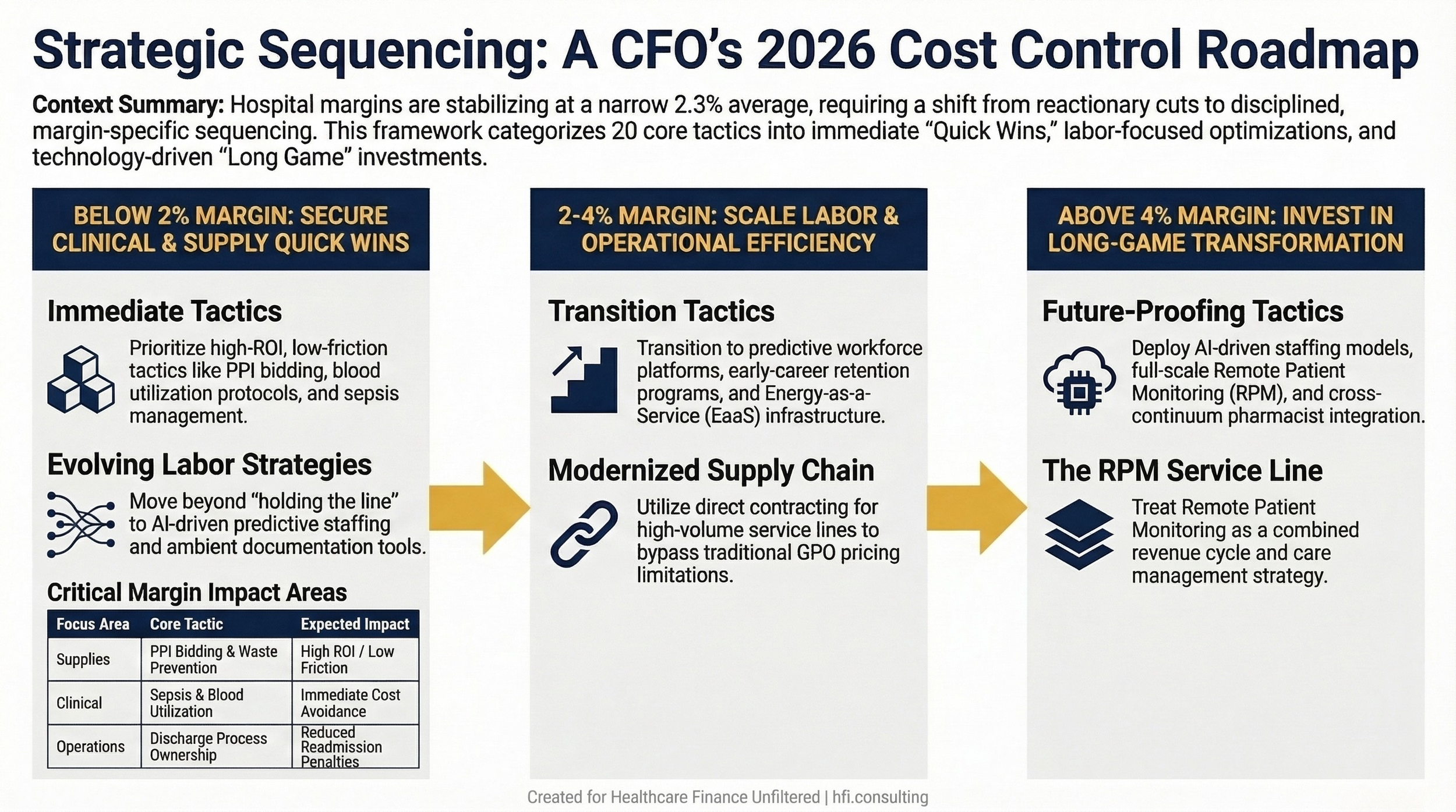
A three-column decision flowchart showing which of the 20 cost control tactics to prioritize based on whether operating margin is below 2%, between 2% and 4%, or above 4%
If you are walking into next quarter's budget cycle without a structured cost discipline framework, this list is your starting point.
The Advisory Board taxonomy is still the right organizing structure. The execution details for 2026 require updating. Use this article as your conversation starter with your leadership team, your supply chain officers, and your clinical operations partners.
What is your current biggest cost containment priority? Hit reply and tell me. I read every response and will feature common themes in an upcoming issue.
The Bottom Line on Cost Discipline
Reactionary cost-cutting does not produce sustainable margin improvement. A CFO who is cutting headcount in a crisis and rebuilding it six months later is not managing costs. They are managing optics.
The health systems that are widening their operating margins in 2026 are not doing anything revolutionary. They are executing the fundamentals listed above with discipline, sequencing, and leadership buy-in. They have physician champions in supply chain conversations. They have technology partners in their staffing models. They have finance and clinical documentation teams working from the same playbook on observation status.
The framework exists. The question is whether your organization is executing it.
For a deeper look at how revenue cycle gaps interact with cost containment strategy, see AI-Powered Revenue Leakage Prevention: The CFO's Implementation Guide for 2026 and CMS Medicaid Fraud Crackdown 2026: What Hospital Finance Leaders Must Do Now.
Ready to build a cost discipline framework tailored to your organization's margin position and service line mix? Connect with me at hfi.consulting or reply directly to this email.
P.S. Which of the 20 tactics on this list has generated the most resistance in your organization, not operationally but from physician or leadership culture? I am working on a follow-up piece specifically on change management for cost initiatives and would love to hear what you have run into.