
AI-Powered Revenue Leakage Prevention: The CFO's Implementation Guide for 2026
How health systems are using AI to stop losing 3-5% of net revenue annually to billing errors, denials, and underpayments
Your health system is operating on a 2-3% margin. Somewhere in your revenue cycle, you are quietly losing another 3-5% of net revenue every year. That gap is not theoretical. It compounds across every service line, every payer contract, and every quarter you delay intervention.
The HFMA published research in January 2026 confirming what revenue cycle leaders have known for years: AI has moved past the pilot phase and is now producing measurable, documented results in charge capture, denial prevention, and underpayment recovery. The question is no longer whether AI belongs in your revenue cycle strategy. The question is whether your implementation plan is specific enough to generate ROI within the next 12 to 24 months.
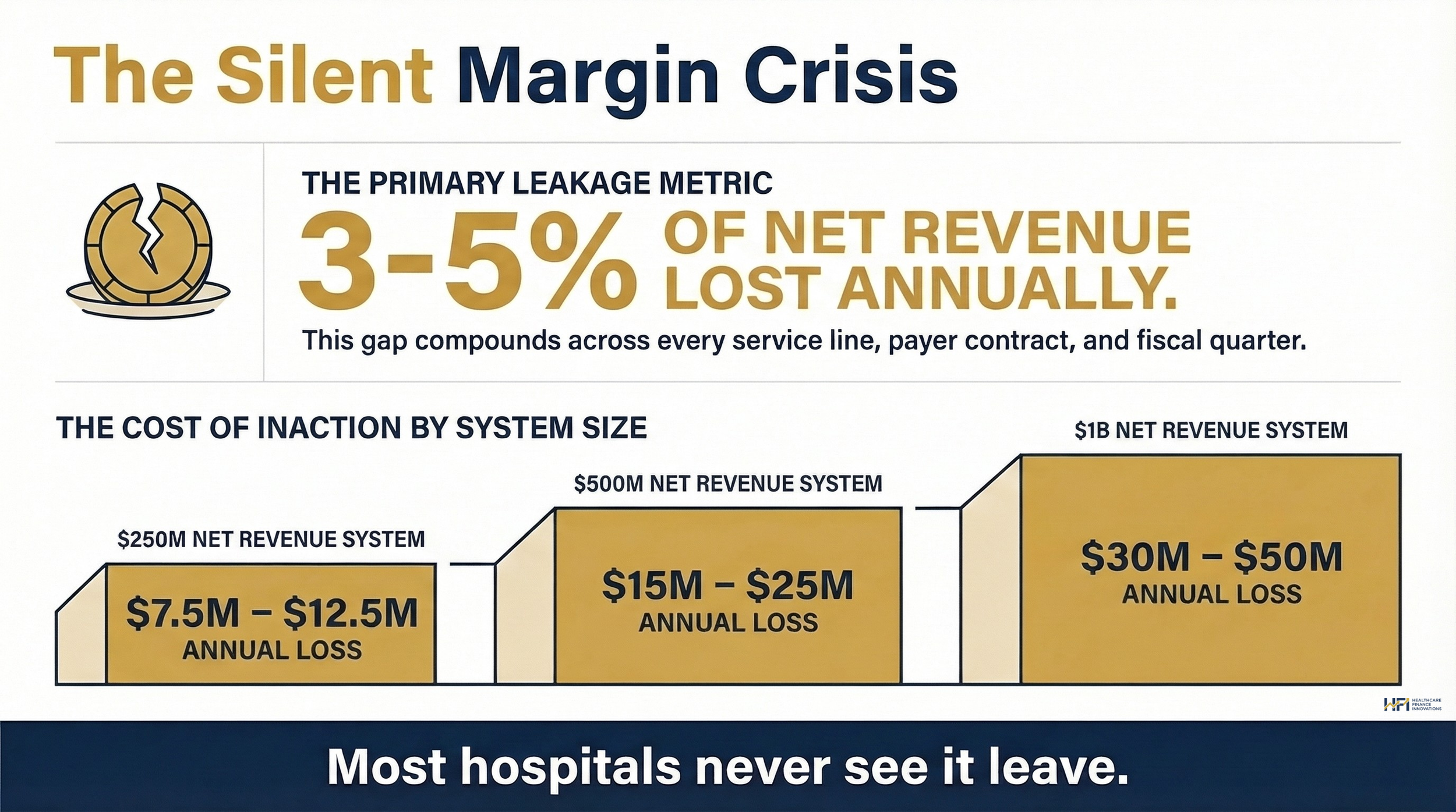
A horizontal scale showing what this means at three system sizes: $250M system = $7.5-12.5M lost / $500M system = $15-25M lost / $1B system = $30-50M lost
What Revenue Leakage Actually Costs You
Before evaluating any AI solution, you need a baseline. Revenue leakage is the unintentional loss of income through inefficiencies, missed billing opportunities, and underpayments. Nationally, hospitals lose approximately 3-5% of net revenue annually to these causes. For a $500M health system, that is $15-25M walking out the door each year without a single patient complaint or audit trigger.
The losses are distributed across three revenue cycle phases, and the breakdown matters for prioritization.
Front-end failures drive the highest volume of denials. Registration errors, eligibility gaps, and prior authorization failures account for roughly 46% of all denied claims. These are preventable. Most are caught too late, after the claim is already submitted and staff time has already been spent.
Mid-cycle deficiencies are the hardest to see. Incomplete clinical documentation, inaccurate coding, and missed charges sit in physician notes and operative reports that no human team can audit at scale. A single missed charge on a complex surgical case can represent thousands of dollars. Multiply that across a high-volume orthopedic or cardiovascular service line and the exposure becomes material.
Back-end shortcomings generate the most frustrating losses. Approximately 15% of claims are denied on first submission. Nearly two-thirds of those are never resubmitted. Payer underpayments, hidden in remittance data across thousands of monthly transactions, can erode collections by up to 11%.
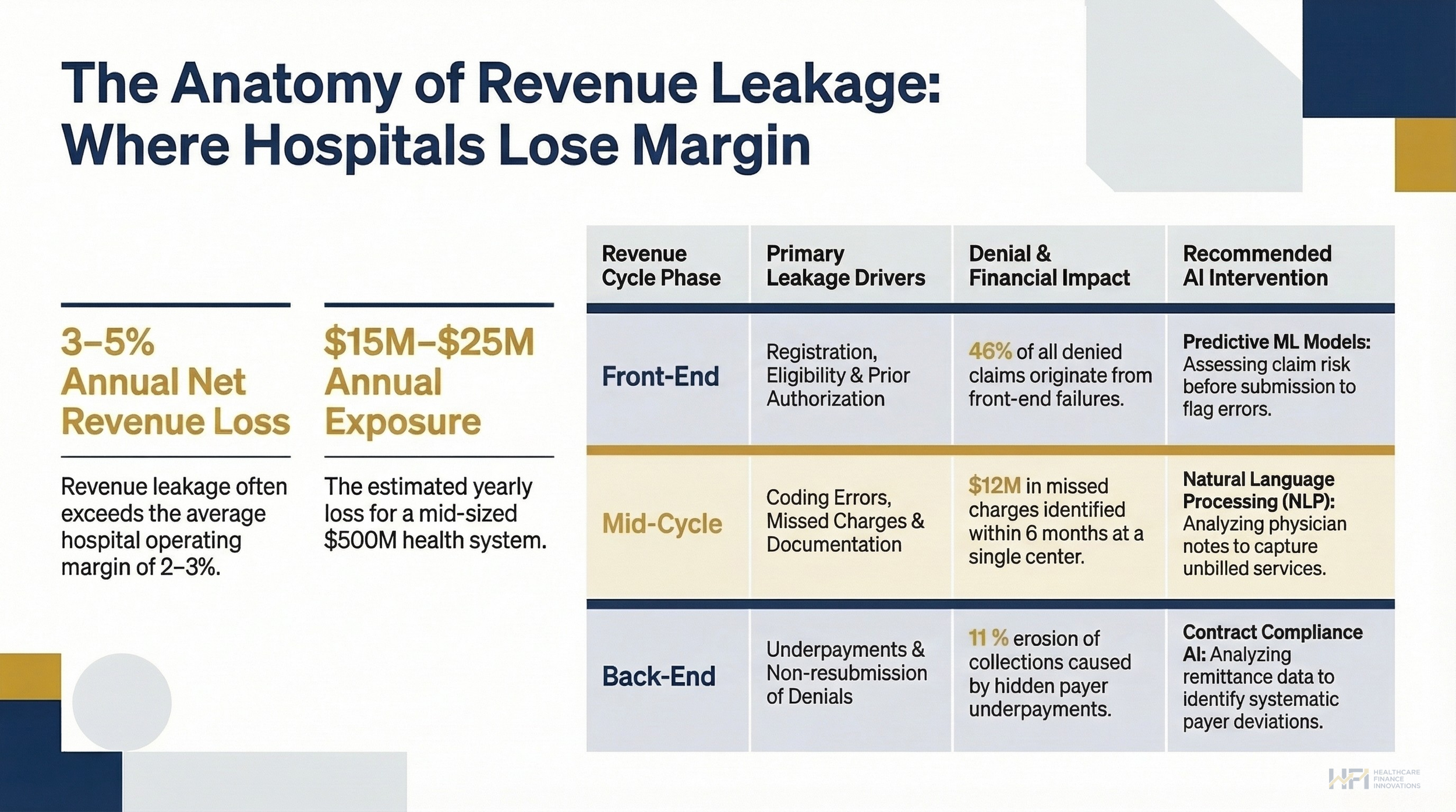
Front-End (Registration, Eligibility, Prior Auth) / Mid-Cycle (Coding Errors, Missed Charges, Documentation) / Back-End (Underpayments, Non-resubmission)
Where AI Creates Measurable Returns
AI is not a single tool. It is a category of capabilities that maps to different revenue cycle failure points. CFOs evaluating vendors need to understand what the technology actually does before evaluating price.
Charge capture via NLP. Natural language processing analyzes physician notes, operative reports, and diagnostic documentation to identify services that were performed but not billed. A large academic medical center in California deployed this approach and identified $12 million in missed charges within six months, primarily in ancillary services like laboratory and imaging. Coding-related denials dropped 22% in the same period.
Denial prediction and prevention. Machine learning models assess claim risk before submission, flagging high-probability denials so billing staff can correct them in advance. A Midwest health system with $3 billion in annual revenue integrated denial prediction with its EHR and reduced denial rates by 18%. First-pass yield improved from 85% to 92%. Total net revenue impact: $40 million in a single year.
Contract compliance and underpayment recovery. AI-enabled tools analyze remittance data at scale, identifying systematic payer deviations from negotiated rates. An integrated delivery network in Texas used this approach to uncover recurring underpayments on orthopedic procedures. Armed with the data, the CFO renegotiated payer contracts and secured an 8% reimbursement increase worth more than $25 million annually.
When I have seen revenue cycle teams at large systems try to do this work manually, the limiting factor is always capacity. Staff can audit a sample. AI can audit everything.
A Use Case Your Vendor Probably Has Not Pitched Yet
Most AI revenue cycle conversations focus on claims, coding, and denials. There is a less-discussed application that has significant upside for service-line-heavy health systems: GPO contract and implant invoice monitoring.
Implant costs in high-volume service lines like orthopedics, spine, and cardiovascular are among the most difficult to manage at scale. Prices shift. Contract terms change. Chargemaster updates lag behind actual purchase prices. The result is either underbilling (you charged less than you paid) or chargemaster misalignment that creates compliance exposure.
AI can be deployed to continuously scrape GPO contracts and vendor invoices, monitoring for price changes and automatically flagging when a chargemaster update is needed. Instead of discovering a six-month pricing discrepancy during an annual audit, you catch it in real time.
For systems where implant-driven service lines represent 15-25% of net revenue, this use case alone can justify a significant portion of an AI vendor contract. It is also the kind of capability that rarely appears in vendor demos because it requires the finance team to ask for it specifically.
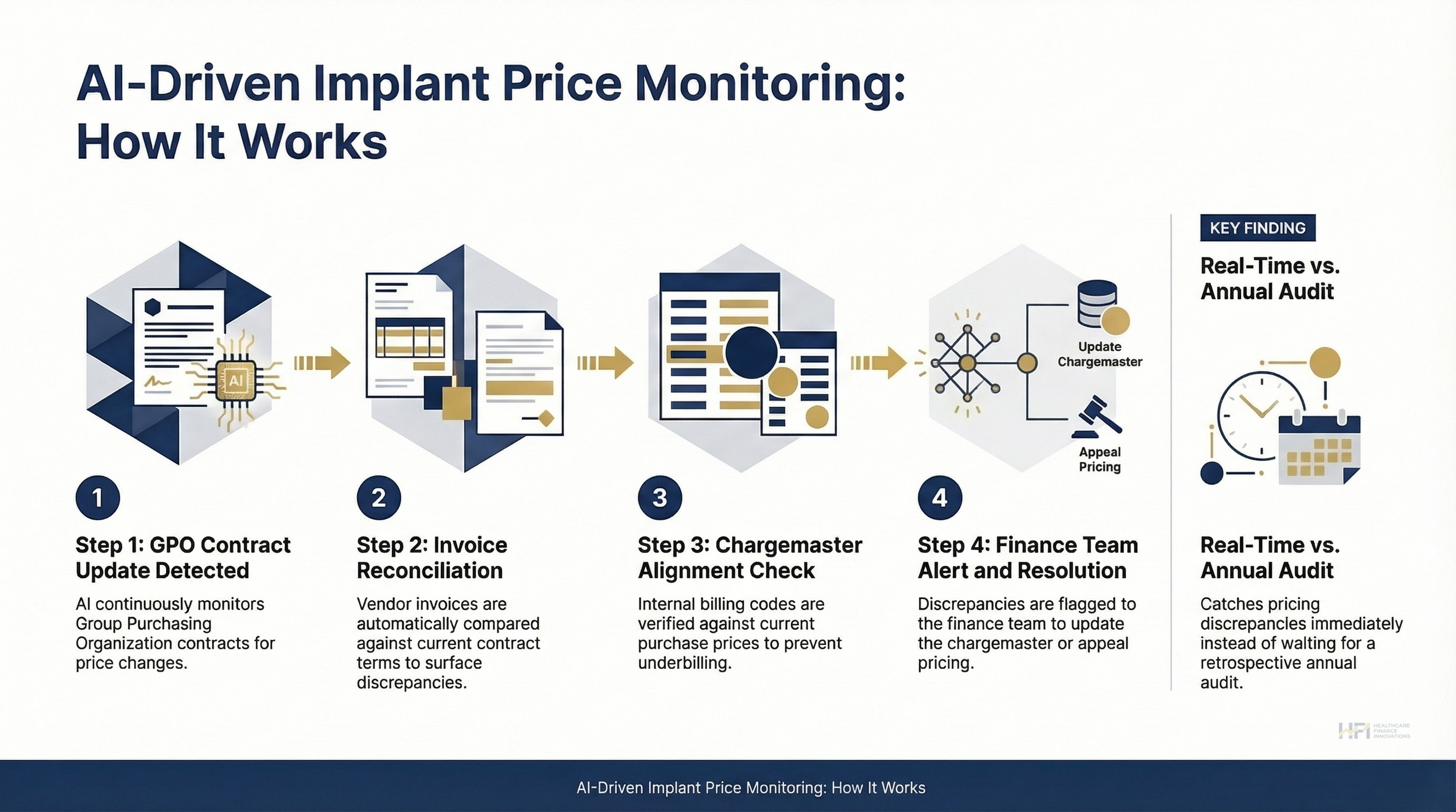
1. GPO Contract Update Detected / 2. Invoice Reconciliation / 3. Chargemaster Alignment Check / 4. Finance Team Alert and Resolution.
If your health system has high-volume orthopedic, spine, or cardiovascular service lines and you are not currently monitoring GPO contracts and invoices against your chargemaster in real time, that gap has a dollar value.
I conduct implant pricing audits and can help your finance team set up an AI-driven monitoring workflow like the one above. If this is a problem you are actively managing, reply to this email or connect with me directly on LinkedIn. I work with a limited number of health systems at a time.
The Regulatory Environment Is Accelerating Adoption
CMS is actively incorporating AI into its own payment oversight infrastructure. The WISeR (Wasteful and Inappropriate Service Reduction) Model uses machine learning to identify clinically unsupported care before payment, signaling that payers on both the government and commercial side are deploying AI to scrutinize your claims with greater precision than ever before.
If your revenue cycle is not using AI to defend your claims, your payers are using it to deny them.
The FY2024 inpatient prospective payment system final rule also introduced social determinants of health as payment rate factors. Accurate documentation of homelessness, food insecurity, and other SDOH codes now directly affects reimbursement. AI tools that improve documentation capture have a direct line to payment rate optimization under this framework.
Governance matters here. Any AI implementation operating on claims data must comply with HIPAA, the False Claims Act, and Stark Law. If an AI model produces overbilling errors, the liability belongs to the health system. Build audit trails, model-validation protocols, and oversight committee structures before go-live, not after.
A Phased Implementation Framework for CFOs
Deploying AI across the revenue cycle requires a deliberate sequence. Systems that try to implement everything simultaneously typically produce neither fast wins nor sustainable infrastructure.
Phase 1 (Months 1-3): Establish your baseline. Run denial analyses, missed-charge audits, and underpayment reviews against the prior 12 months of data. This is not optional. Without a documented baseline, you cannot demonstrate ROI to your board, and you cannot evaluate whether a vendor is actually performing. At Ascension, when I worked across seven hospitals tracking productivity and operational metrics, the systems that maintained rigorous baselines were the ones that could defend their investments when budget cycles tightened.
Phase 2 (Months 3-9): Deploy quick-win applications. Focus on eligibility verification, claim scrubbing, and denial prediction first. These domains have the shortest feedback loop and the clearest ROI metrics. Most systems see measurable improvement within six months.
Phase 3 (Months 9-18): Scale into advanced applications. Once front-end and prediction tools are stable, expand into NLP-based documentation improvement, AI-assisted coding, and contract compliance monitoring. This is also the phase to integrate GPO and implant price monitoring if you have high-volume implant service lines.
Ongoing: Weekly dashboard review. Track first-pass yield, denial rates, discharged-not-final-billed accounts, days in accounts receivable, and patient self-pay collections. If you cannot see the metrics weekly, you are managing revenue cycle performance in the dark.
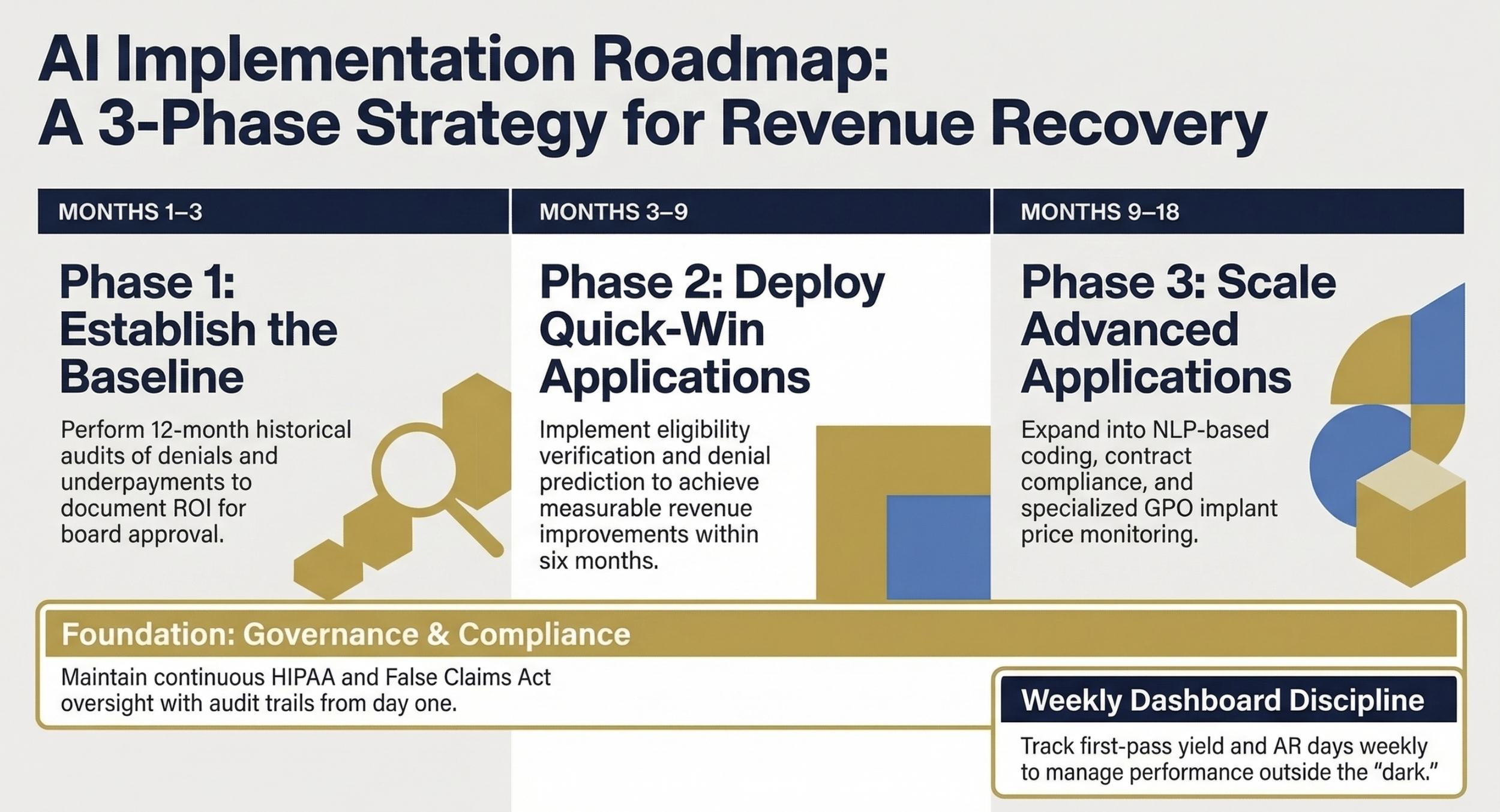
Three-phase timeline graphic showing key milestones
The Workforce Reality CFOs Are Not Talking About Enough
Every AI implementation displaces some manual work. That is the point. But the displacement requires active management, not just announcement.
Billing staff roles shift from manual data entry and claim processing to AI monitoring, exception handling, and financial analysis. This is a real workforce transformation, and it carries real costs: training time, potential attrition among staff who resist the change, and a transitional period where both the old process and the new system are running simultaneously.
The most common failure mode I see in AI revenue cycle deployments is not technical. It is organizational. The technology works. The rollout plan does not account for the human response to it.
Plan for a 6-12 month transition period. Invest in training. Identify your internal champions early. And communicate clearly to staff that the goal is to eliminate the tedious work, not the people doing it.
If You Are Not Using AI in Payer Negotiations, You Are Leaving Money on the Table
One of the most underutilized applications of AI-generated data is contract renegotiation. The Texas IDN example above is instructive: the CFO did not just recover underpayments. They used AI-generated evidence of systematic payer noncompliance to restructure a contract worth $25 million annually.
This is a capabilities shift. Your payers have data scientists. If you are sitting across the table from a payer contract team with a spreadsheet and they have a machine learning model that has analyzed every claim you have submitted in the last three years, you are at a structural disadvantage.
AI-generated contract compliance reports, denial pattern analyses, and underpayment trend data give your finance and managed care teams the evidence base to negotiate from a position of documented fact rather than industry benchmarks.
If your revenue cycle strategic plan for 2026 does not include a specific, phased AI implementation roadmap with baseline metrics and defined ROI thresholds, that is the gap to close before Q2.
Revenue Cycle Management in 2026: Stop Optimizing and Start Diagnosing Your Real Problems offers a diagnostic framework for identifying where your system's specific leakage is concentrated before you select a vendor. Start there.
What is your current first-pass yield rate, and do you know which denial categories are driving the gap? Hit reply and tell me. I read every response.
The evidence is no longer speculative. AI is producing documented financial returns for systems that deploy it with discipline. The $12M in missed charges, the $40M net revenue recovery, the $25M contract renegotiation outcome — these are not projections. They are reported results from systems operating under the same margin pressure yours is.
The implementation window matters. Systems that establish baselines now and begin phased deployment in Q2 will have 12+ months of performance data before the next budget cycle. Systems that wait will be evaluating vendors with no comparative leverage and no internal proof of concept.
You can also revisit the AI Medical Scribes: The ROI Case Healthcare Finance Leaders Need Before Budget Season for a parallel look at how AI ROI frameworks apply across different operational domains, and Why Your Revenue Cycle ROI Calculations Are Probably Wrong for the methodology behind measuring returns that will hold up to board scrutiny.
The strategic imperative is clear. Build the baseline, select the right deployment sequence, and govern the implementation from day one.
P.S. I am curious: Has your health system deployed any AI revenue cycle tools yet? If yes, what was the first use case you tackled, and did the ROI materialize on the timeline you projected? If no, what is the primary barrier holding you back? Hit reply. I want to understand where finance leaders actually are on this.