
Kaiser Permanente's $9.3B Profit Problem: What the Nonprofit Model Crisis Means for Healthcare CFOs
$73B in reserves. A nursing strike over staffing. Two federal settlements. The integrated payer-provider model has a governance problem every CFO should study.
The headline is $9.3 billion. But the story isn't really about profit.
Kaiser Permanente posted $9.3 billion in net income for 2025, drawing immediate scrutiny from labor unions, policy researchers, and community advocates. Critics are questioning whether the nation's largest private nonprofit has quietly become something else entirely. The scrutiny is warranted. But for healthcare finance leaders, the more urgent question isn't whether Kaiser is a good nonprofit. It's what the structural vulnerabilities exposed by this story mean for your organization's governance, your workforce strategy, and your risk posture heading into 2027.
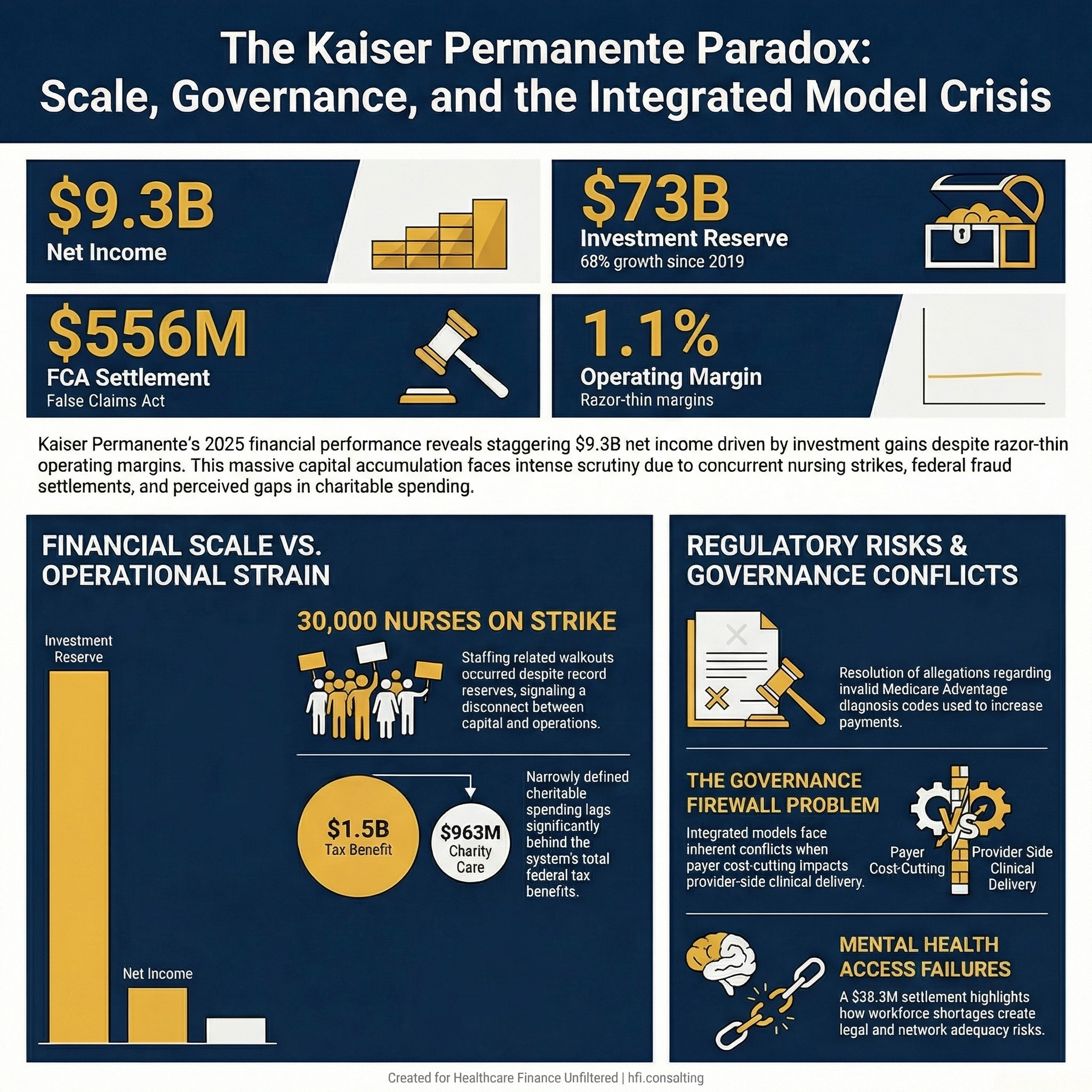
Kaiser Permanente 2025 financial snapshot showing $9.3B net income, $73B reserve, $556M FCA settlement, 1.1% operating margin
The Numbers That Don't Add Up
Start with the operating results. Kaiser reported $1.4 billion in operating income on $127.7 billion in revenue, a 1.1% operating margin. That is a thin margin by most measures, actually consistent with the industry-wide pressure most health system CFOs are navigating right now.
The $9.3 billion net income figure came primarily from investments. That distinction matters for how you read the story, but it does not resolve the tension.
Kaiser's reserve of cash and investments reached $73 billion in 2025. That is 68% higher than in 2019. Meanwhile, 30,000 nurses and healthcare professionals walked out for four weeks in California and Hawaii, citing patient safety and staffing levels as the core issues, not wages.
Sit with that for a moment. A $73 billion investment portfolio. A four-week nursing strike over whether there were enough staff to safely care for patients.
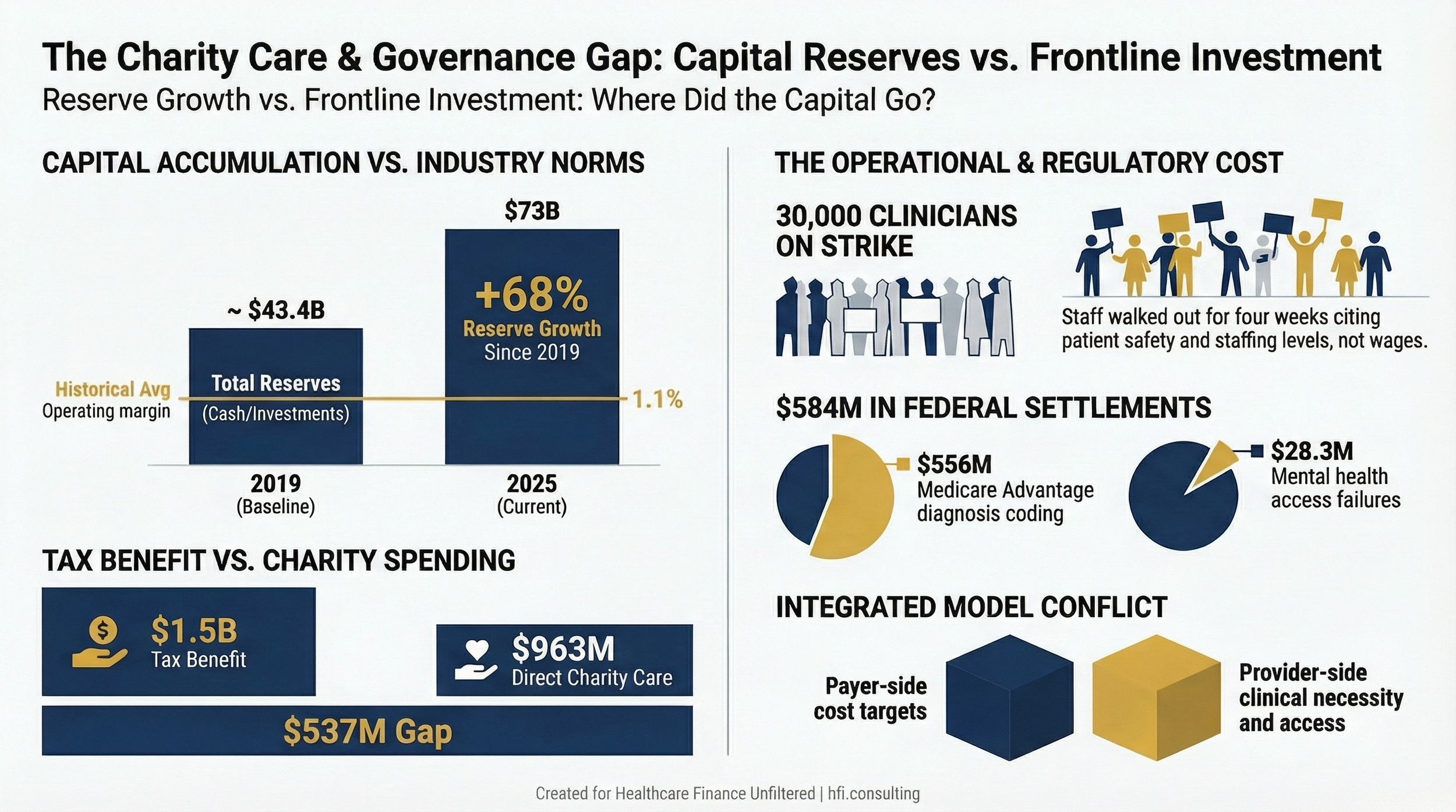
Bar chart comparing Kaiser Permanente investment reserve growth from 2019 to 2025 against nonprofit health system industry median days cash on hand
The Charity Care Gap
The Lown Institute's 2024 analysis found that Kaiser had the largest disparity between tax benefits and charitable spending among the largest nonprofit systems in the country. Kaiser received approximately $1.5 billion in tax and other benefits through its nonprofit status. It provided $963 million in patient financial assistance and community health program contributions.
Kaiser disputes that calculation. The system told the Los Angeles Times its combined charitable efforts totaled $5.3 billion when including affordable housing, food access, community health, and disaster recovery investments. The American Hospital Association has also pushed back on Lown's methodology, arguing it oversimplifies the policy, payment, and demographic complexity hospitals actually operate within.
Both arguments have merit. The AHA is right that charitable mission accounting is genuinely complicated. And Kaiser's expanded definition of community investment is not unreasonable.
But the Lown analysis points to a structural reality that finance leaders cannot ignore: when your tax benefit exceeds your narrowly defined charity care spending by more than half a billion dollars, the math is a public relations problem regardless of accounting methodology.
California Is Not the Rest of the Country
Here is the context the national coverage largely misses. Kaiser operates predominantly in California and along the West Coast. These are among the highest-taxed, most heavily regulated labor markets in the country.
California has a $20 minimum wage for healthcare workers. The state's nursing ratio requirements are among the strictest nationally. And the broader California workforce exodus is real. As employees and employers continue relocating to lower-tax environments, Kaiser faces a talent retention challenge that compounds with every year it operates in this market.
A $73 billion reserve is not inherently indefensible. Large integrated systems have legitimate reasons to hold significant reserves: catastrophic risk, long-term capital planning, bond rating requirements, and pension obligations all factor in. California's unpredictable regulatory environment adds additional justification for a robust rainy-day fund.
But there is a meaningful difference between maintaining strategic reserves and allowing frontline staffing levels to deteriorate while those reserves grow 68% in six years. The nurses who walked out were not asking for a share of the investment portfolio. They were asking for enough colleagues to safely deliver care.
From my time managing financial operations across seven hospitals at Ascension, one of the most persistent governance challenges was maintaining discipline around the gap between what the balance sheet could absorb and what the operational model actually needed. The temptation to optimize the investment story at the expense of frontline resource allocation is not unique to Kaiser. But Kaiser's scale makes the consequences unusually visible.
The False Claims Act Problem Is Bigger Than One Settlement
In January 2026, Kaiser agreed to pay $556 million to resolve allegations it submitted invalid diagnosis codes for Medicare Advantage enrollees to obtain higher federal payments. The system said it settled to avoid prolonged litigation.
In February, it agreed to pay $28.3 million to resolve allegations its health plan failed to provide timely and appropriate access to mental health and substance use disorder services.
The MA diagnosis code settlement sits within a pattern of industry-wide scrutiny that healthcare finance leaders have been tracking for several years. If you have not read our analysis of the Aetna False Claims Act settlement, the risk adjustment documentation environment is not getting more forgiving. CMS and DOJ are both actively pursuing MA overpayment cases, and integrated systems with both payer and provider operations face compounded exposure.
The mental health access settlement is a different category of problem. At Florida Blue Medicare, the core challenge in meeting network adequacy requirements for behavioral health was not network design. It was the workforce. Geographic coverage requirements simply could not be met in many markets because qualified behavioral health providers did not exist in sufficient supply. Kaiser cited the same dynamic in its response to the mental health settlement, pointing to a 10-week strike by 2,000 mental health clinicians in 2023 and ongoing clinician shortages.
That explanation is operationally accurate. It is also an indictment of the system's long-term workforce investment strategy. If your organization cannot meet federal network adequacy requirements because you do not have enough credentialed behavioral health providers, that is a capital allocation decision, not a force majeure event.
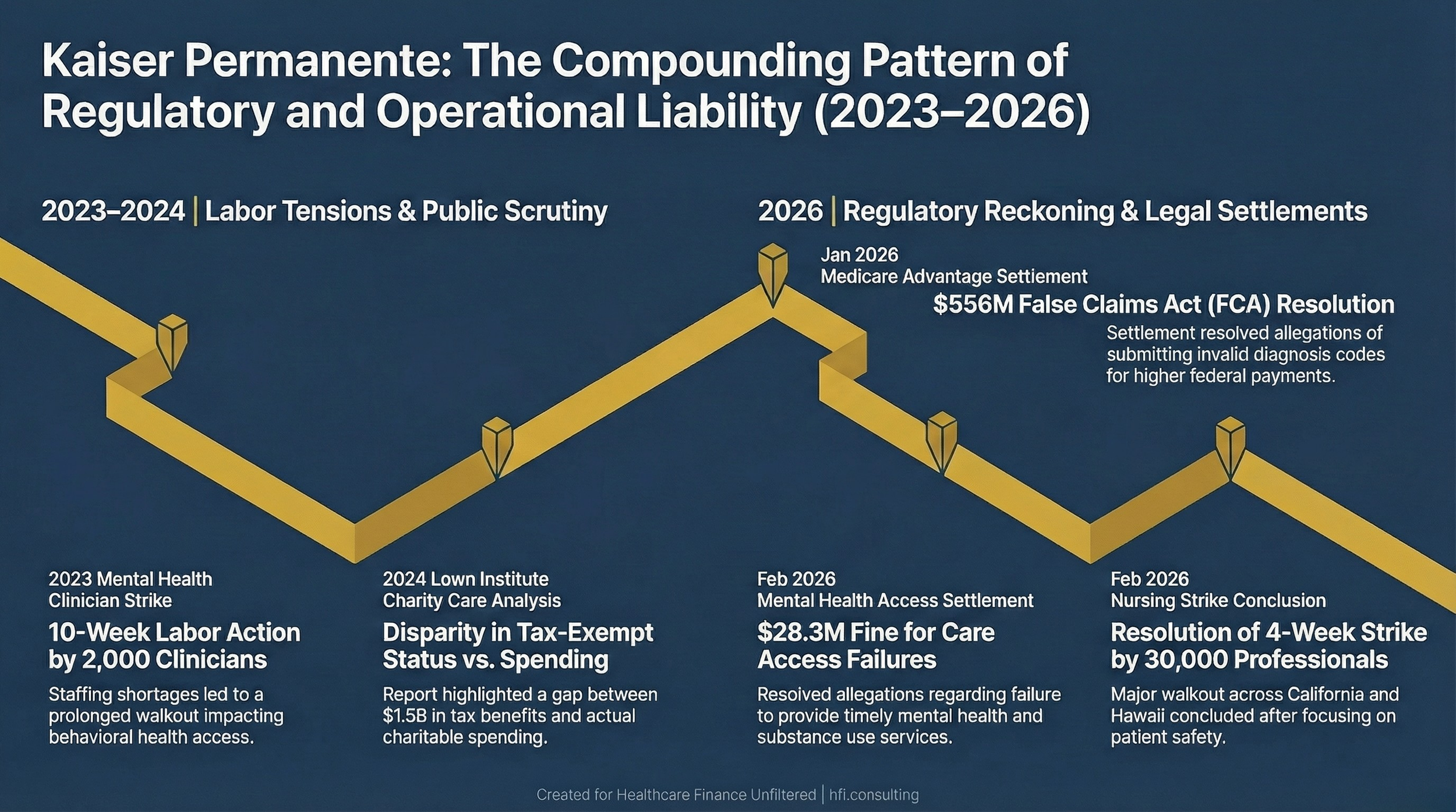
Timeline of Kaiser Permanente regulatory and legal events from 2023 through early 2026 including labor actions and federal settlements
The Integrated Model's Structural Problem
This is the issue that deserves more attention than the profit headlines are generating.
Kaiser is not just a health system that also happens to have an insurance arm. It is a fully integrated payer-provider model where the same organization makes underwriting decisions, sets formulary policies, manages utilization review, and employs the clinicians delivering care. At scale, that integration creates efficiencies. It also creates conflicts that are structurally difficult to resolve.
Here is a concrete example of where the conflict becomes operational. When the payer side determines that a specific drug is not on the PBM formulary, the provider-side clinician must work within that constraint regardless of clinical preference. The patient's physician and the patient's insurer answer to the same financial leadership. That is not a hypothetical tension. It is a daily operational reality for Kaiser clinicians and, by extension, Kaiser patients.
The Prior Authorization Final Rule and related CMS guidance have attempted to create structural guardrails around exactly this dynamic. But regulation cannot fully substitute for governance.
A meaningful governance firewall in an integrated model requires specific structural commitments. Medical necessity and formulary decisions must be made by clinically independent bodies that operate under governance structures separate from the CFO's direct line of accountability. Utilization management protocols must be benchmarked against external clinical standards, not just internal cost targets. And there must be an independent mechanism for identifying and escalating cases where payer-side decisions are producing measurable patient safety or access outcomes.
Without that structure, the integrated model's efficiency arguments gradually hollow out. You end up with a system that is optimized for financial performance on the payer side while the provider side absorbs the quality and workforce consequences.
What CFOs at Other Organizations Should Do Right Now
The Kaiser story is not just a cautionary tale about scale. It is a checklist.
If you lead finance at a nonprofit health system, pull your last three years of Schedule H filings and calculate your own tax benefit to charity care ratio. Not because the Lown methodology is the only valid measure, but because the scrutiny that landed on Kaiser will reach other organizations as Congress and state legislatures sharpen their focus on nonprofit accountability.
If your organization operates any Medicare Advantage business, risk adjustment documentation practices are a material financial risk. The $556 million Kaiser settlement is not an outlier. It is a signal about the enforcement direction.
If you are working through your own risk adjustment compliance posture, or if you want a framework for evaluating your charitable spending documentation, reply to this email and let's talk through what that looks like for your organization.
If you participate in any integrated payer-provider arrangement, even a partial one such as an ACO or a risk-bearing contract, map the decision points where payer-side cost pressure could produce provider-side access or quality outcomes. Identify those pressure points before a regulator or a plaintiff's attorney does it for you.
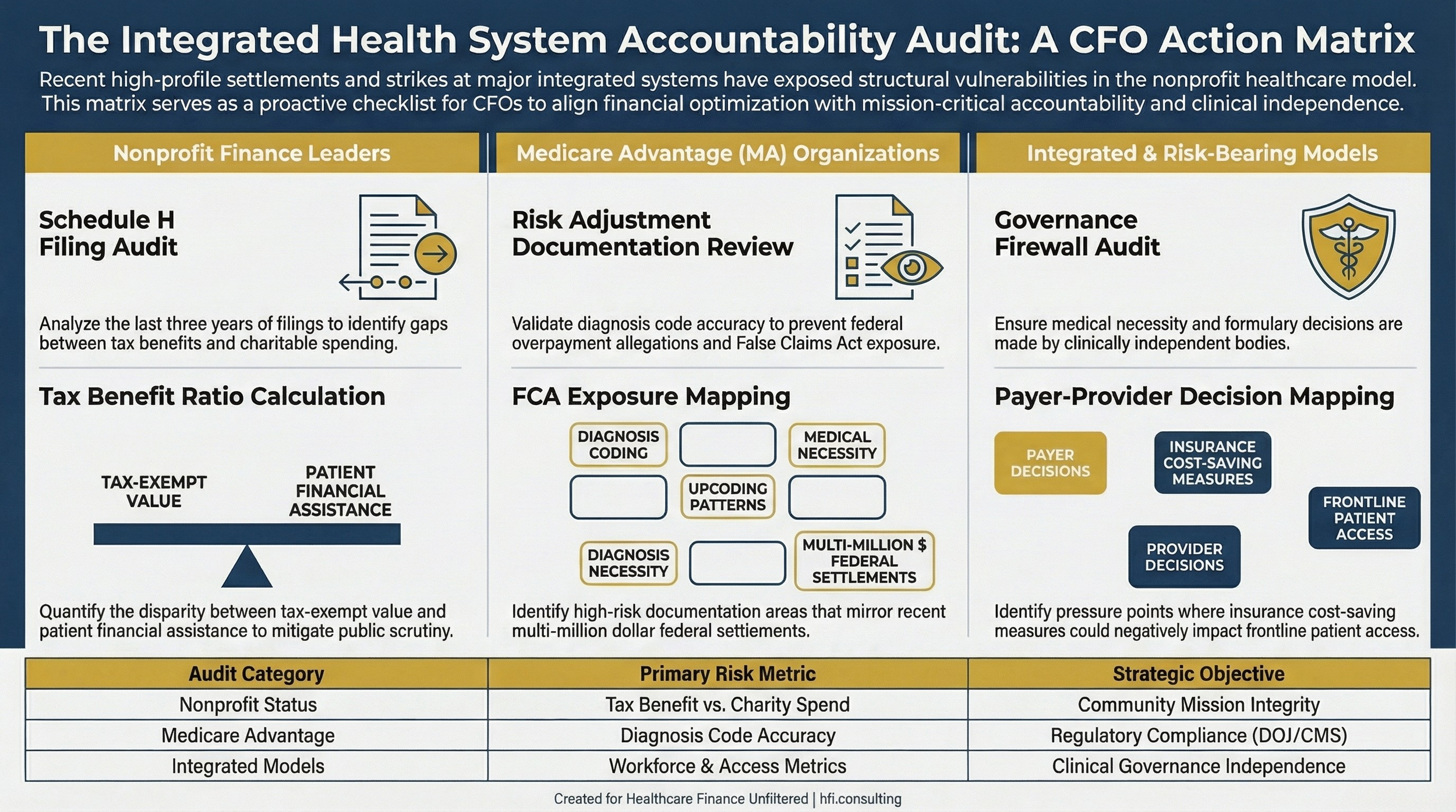
Three-column CFO action matrix covering accountability checks for nonprofit systems, Medicare Advantage participants, and integrated payer-provider organizations
The Governance Firewall Is Not Optional
The argument for breaking up fully integrated payer-provider models is gaining momentum in Washington. Mark Cuban's recent support for the Break Up Big Medicine Act signals that this conversation is moving from the policy fringe toward legitimate legislative consideration.
Most healthcare finance leaders are not running Kaiser-scale integrated models. But the governance principle applies at every level of integration. Wherever payer-side incentives and provider-side care delivery share a financial decision-maker, there needs to be a documented, auditable mechanism for ensuring clinical accountability is not subordinate to cost optimization.
The inconsistency is the vulnerability. At Ascension, governance structures around community mission varied significantly across markets. Some hospitals had formal board-level accountability mechanisms. Others relied on regional leadership culture. The markets with stronger formal structures navigated margin pressure more sustainably over time because the mission commitments were structural, not discretionary.
Kaiser's situation illustrates what happens at scale when integration is optimized for financial performance without sufficient structural separation between the payer and provider accountability chains. Thirty thousand nurses and two federal settlements later, that structure is being examined by people with subpoena power.
You do not want to get to that stage of the review process before you understand your own governance architecture.
If you found this analysis useful, consider sharing it with a colleague navigating similar decisions. A paid subscription to Healthcare Finance Unfiltered gives you access to the full archive and frameworks like this every week.
P.S. Here is a question worth sitting with: At your organization, who has the authority to override a payer-side formulary or utilization management decision when clinical staff identifies a patient safety concern? Is that person's accountability structure independent of the CFO? Hit reply and tell me what that governance looks like where you work.