
DOJ Hospital Antitrust Crackdown 2026: What CFOs Must Review in Payer Contracts Now
Two major health systems are facing federal antitrust suits over payer contracts. Here's the clause-level review your managed care team needs to do now.
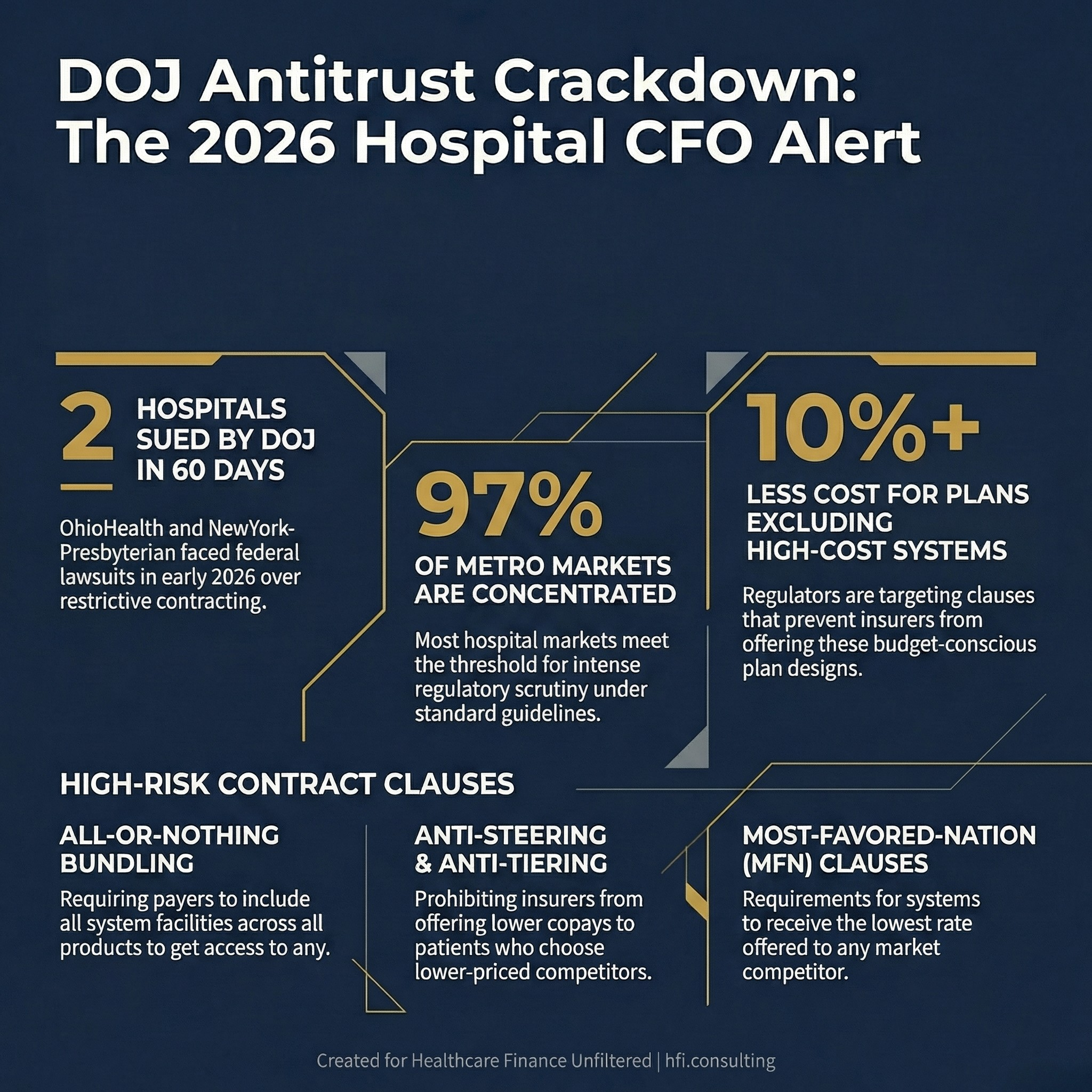
The Department of Justice sued two major hospital systems this quarter over their payer contracts, and a third is under active investigation. If your managed care contracting team hasn't briefed you on what triggered these lawsuits, that is a conversation you need to have before the week is out.
Three statistics showing DOJ's 2026 antitrust enforcement pace against hospital systems
What the DOJ Actually Sued Over
On February 20, 2026, the Justice Department's Antitrust Division filed suit against OhioHealth Corporation, the largest healthcare system in central Ohio. The complaint alleged that OhioHealth used its market dominance to force insurers into contracts that prevented payers from offering innovative, budget-conscious health plans. The core issue: OhioHealth required insurers to include it across all commercial products regardless of price comparisons with competitors.
Then, on March 26, 2026, DOJ filed a civil antitrust lawsuit against NewYork-Presbyterian, one of the most powerful hospital systems in New York City. The complaint described a pattern of leveraging market power to prevent payers from offering lower copays when patients chose lower-priced competitors. DOJ's language was direct: NYP used its position to insulate itself from what the system's own internal documents called "erosion of rates of payment."
A third system, Advocate Health in Charlotte, is under active DOJ investigation according to reporting by the Wall Street Journal.
These are not isolated cases. The FTC launched a new healthcare task force in early 2026, and nearly two dozen states now have some form of anticompetitive contracting restrictions on providers and insurers. The enforcement signal is unmistakable.
The Specific Contract Clauses at Issue
Understanding what triggered these lawsuits requires knowing exactly which contract provisions regulators are targeting. There are three primary clause types that appear in both the OhioHealth and NYP complaints.
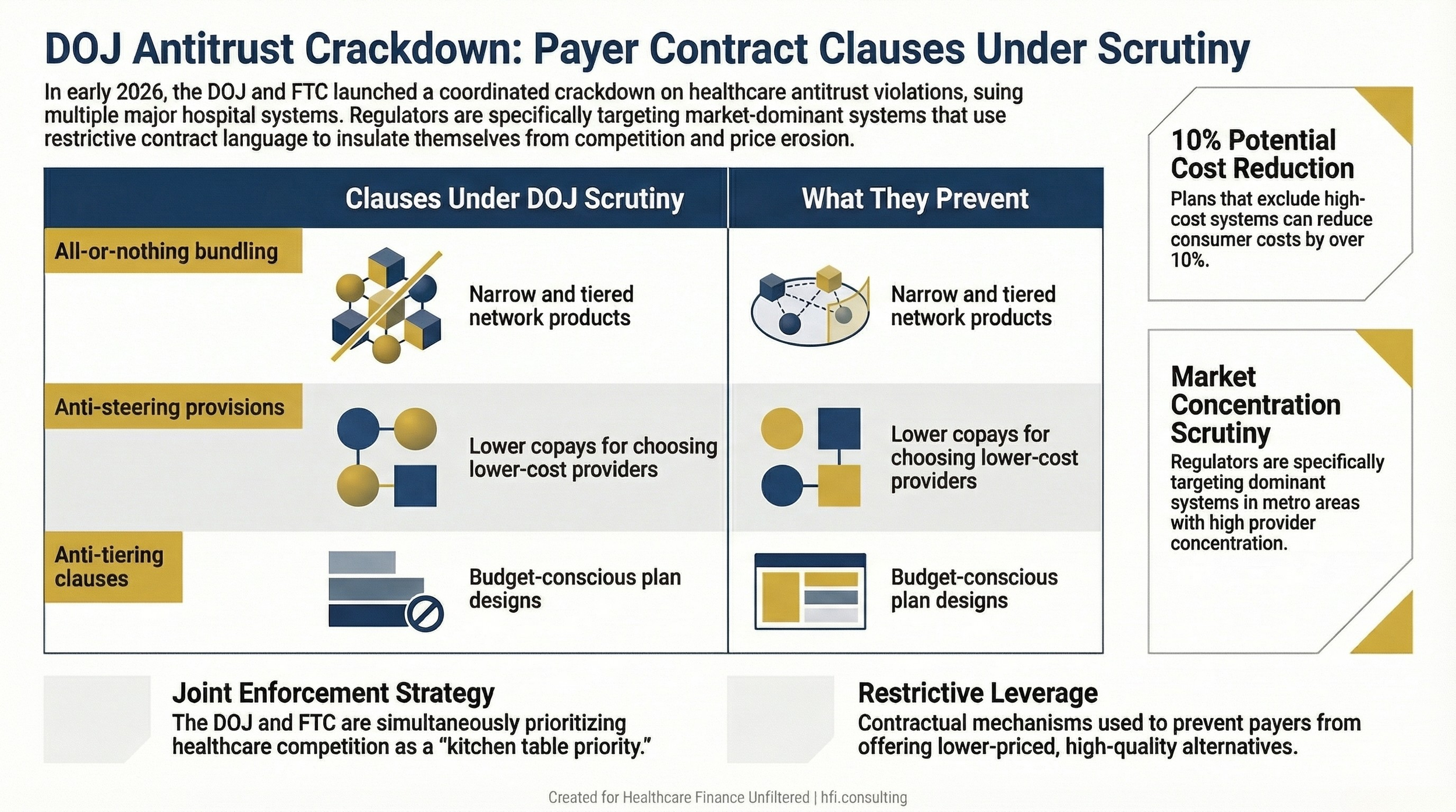
All-or-nothing bundling. OhioHealth required insurers to include the entire OhioHealth system across all commercial network products. This prevented insurers from building narrow or tiered networks that could steer patients toward lower-cost alternatives. Insurers who wanted any OhioHealth facility had to include all of them in all products.
Anti-steering and anti-tiering provisions. NYP required insurers to include its facilities in the most favored network tier and prevented payers from offering lower copays when patients chose competitor hospitals. These clauses specifically blocked the product design that would allow payers to reward patients financially for choosing lower-cost, comparable-quality providers.
Most-favored-nation (MFN) clauses. While not the primary focus of these suits, MFN provisions that require a system to receive the lowest rate offered to any competitor in the market have historically drawn similar scrutiny and are often negotiated alongside anti-tiering language.
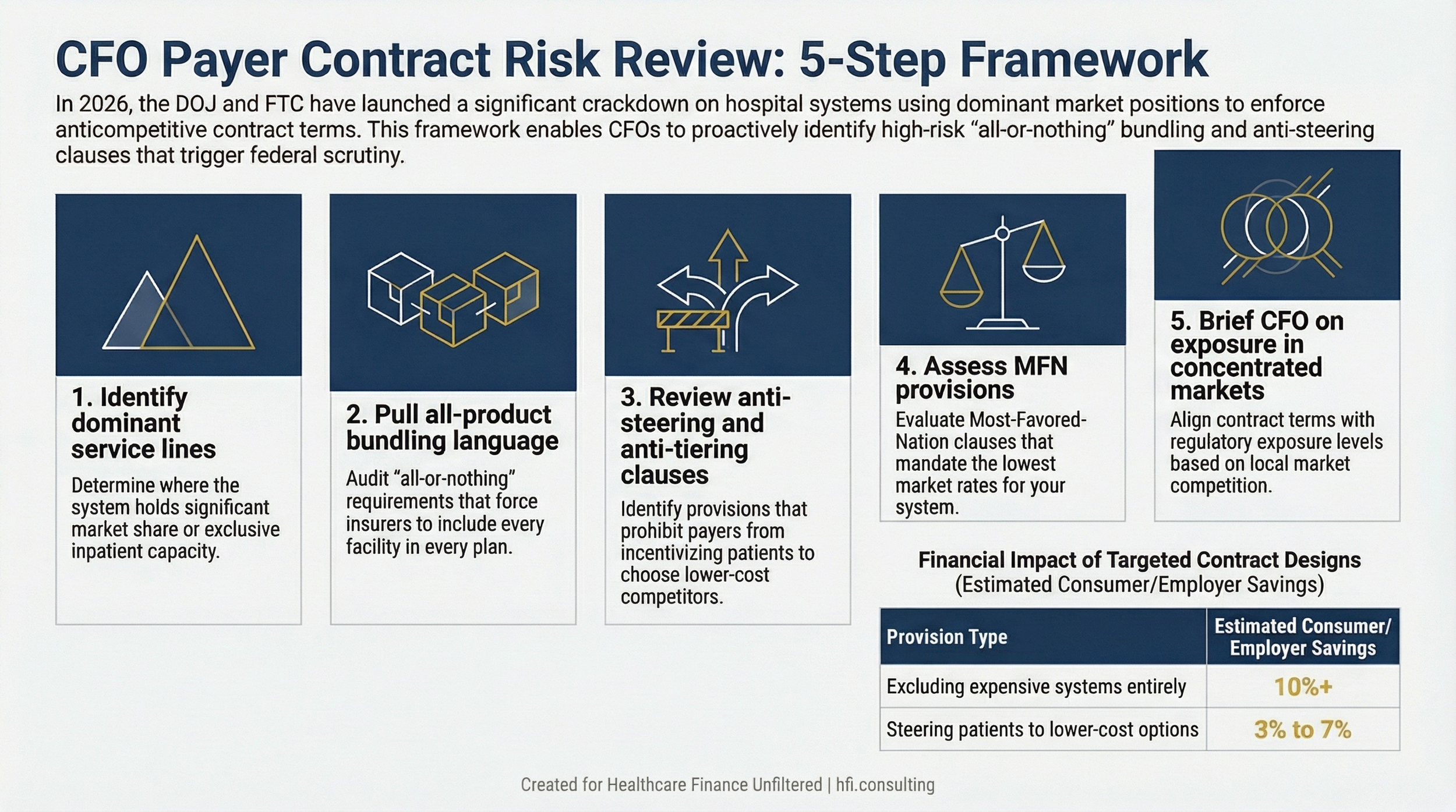
The DOJ's position is that these clauses, when used by systems with dominant market position, prevent the development of the budget-conscious plan designs that exist in other parts of the country. According to the Wall Street Journal's investigation of hospital contracting, plans that exclude expensive systems entirely can cost consumers and employers more than 10% less. Plans that include all providers but steer patients toward lower-cost options can save 3% to 7% or more.
Comparison table showing three anticompetitive contract clause types and what patient choice each one eliminates
Why Market Structure Determines Exposure
The DOJ cases are not about all large hospital systems. They are specifically targeting systems with dominant market position that use contractual mechanisms to prevent competition from working.
Nearly 97% of metro areas have concentrated markets for inpatient hospital care under standard antitrust guidelines, according to reporting from Axios. That concentration gives large systems leverage in payer negotiations. The question regulators are asking is whether that leverage is being used to restrict patient choice rather than compete on quality and value.
This distinction matters for every CFO in a market with fewer than four major systems. The more concentrated the market, the more scrutiny any restrictive contracting terms will attract.
Jacksonville, Florida offers a useful counterpoint. Having worked at Baptist Health, UF Health, and Ascension Florida across my career, I watched a market where genuine competition kept contracting behavior in check. Baptist, Ascension, UF Health, HCA, and Mayo Clinic compete actively across cardiology, neurology, and trauma designation. They compete for Centers of Excellence accreditations and advertise those wins across the city. That competition drove volume and quality metrics up for every system. Prices did not come down, but the competitive dynamics created a check that prevented any single system from dictating terms to payers.
The evidence of that competitive check came in Fall 2025, when Baptist Health left the Florida Blue Medicare Advantage network. The exit created real friction for retirees who had built relationships with Baptist providers. But it also demonstrated that in a genuinely competitive market, a payer has meaningful alternatives. That is precisely what DOJ says OhioHealth and NYP prevented through their contract terms.
The CFO's Contract Audit: What to Review Now
The managed care contracting team handles the clause-level detail of payer agreements. That is the right operational model. But the DOJ suits put specific contract terms into the executive risk category, which means finance leadership needs visibility into provisions that may not have been part of recent CFO-level discussions.
There are four areas worth requesting a briefing on from your managed care team.
All-product or all-facility bundling requirements. Does your system require payers to include all facilities across all network products as a condition of including any facility? If yes, understand the market share rationale and whether it mirrors language in the OhioHealth complaint.
Anti-steering and anti-tiering provisions. Do your payer contracts prohibit insurers from offering lower member cost-sharing for patients who choose lower-priced competitors? These are the specific provisions DOJ cited against NYP.
Most-favored-nation clauses. Do any contracts require payers to give your system the lowest rate offered to any market competitor? In concentrated markets, these attract scrutiny.
Exclusivity and network inclusion requirements. Are there provisions that make it difficult for payers to build or offer plans that do not include your system? The goal of these clauses from a negotiating standpoint is understandable. The regulatory risk in a concentrated market is real.
This is not a legal audit. It is a strategic briefing to ensure that terms negotiated at the managed care level are aligned with the organization's regulatory exposure, particularly if your market is concentrated or your system is the dominant provider in a service line.
Five-step process flow for CFO-level payer contract antitrust risk review
The Payer Perspective: Broad Networks and Missed Leverage
The DOJ suits are framed as consumer protection actions against hospital systems. That framing is accurate as far as it goes, but finance leaders on the payer side of the table have their own complexity to navigate.
Even in competitive markets like Jacksonville, most commercial insurers and Medicare Advantage plans are still locked into broad network designs. Tiered network products that would allow payers to financially incentivize patients toward lower-cost, high-quality providers exist in other parts of the country. They have not been widely developed in markets where hospital systems have successfully negotiated anti-tiering and anti-steering provisions.
The irony is that payers in concentrated markets have largely accepted these contract terms as the cost of network adequacy. When a single system controls a large share of inpatient capacity in a market, building a commercially viable network without them is not a realistic option. That is the structural leverage DOJ is now challenging.
For payer CFOs, the enforcement trend creates a different kind of opportunity. If DOJ succeeds in enjoining these provisions, payers in concentrated markets may gain the product design flexibility to build tiered networks for the first time in years. The financial modeling implications for benefit design, premium competitiveness, and employer contracting are worth starting now rather than waiting for litigation outcomes.
The Axios reporting on the NYP lawsuit quoted Georgetown health policy researcher Katie Keith noting that eliminating anti-steering restrictions would give insurers and employers more flexibility to negotiate in-network rates rather than being "at the will of the hospital system." That flexibility is also a revenue and margin opportunity for plans willing to move first.
What the DOJ's Posture Signals for the Rest of 2026
The Acting Assistant Attorney General's remarks at George Washington Law School on March 23, 2026 made the enforcement posture explicit. The DOJ Antitrust Division filed its first new civil conduct case of this administration, specifically targeting anticompetitive healthcare contracting. The division characterized fighting for lower costs and more choices in healthcare as a "kitchen table priority."
This is not a trend that will slow down before the midterm election cycle, which Axios noted is driving some of the political timing. The FTC's simultaneous health care task force launch reinforces that both major antitrust enforcement bodies are moving on the same set of issues at the same time.
For CFOs at large health systems in concentrated markets, the question is not whether to have the contract audit conversation. The question is whether to have it before or after a subpoena lands.
Jacksonville's competitive market structure is not a guarantee of insulation. High out-of-network cost penalties that effectively trap patients within a system's network can raise the same questions that formal anti-steering clauses raise, even if they operate differently from a contracting standpoint. The principle DOJ is enforcing, patient and payer choice, applies to any mechanism that limits it.
For more on the regulatory environment affecting hospital revenue and compliance, see AI-Powered Revenue Leakage Prevention: The CFO's Implementation Guide for 2026 and the CMS Medicaid Fraud Crackdown 2026 analysis in the article section.
The Bottom Line for Finance Leaders
Two large hospital systems are defending federal antitrust suits over their payer contracts. A third is under investigation. The provisions at issue, all-or-nothing bundling, anti-steering clauses, and anti-tiering requirements, are common in payer agreements negotiated by systems with market leverage.
Most CFOs know the high-level terms they want in payer agreements. The clause-level detail lives with the managed care contracting team. Given where enforcement is heading, that gap between executive awareness and contract detail has become a strategic risk issue, not just an operational one.
The Jacksonville market shows what genuine competition produces. Multiple strong systems competing on service line excellence, quality designations, and patient access. It is not a perfect market. But it is a functional check that prevented the kind of contractual overreach now drawing federal attention.
Review your contracts. Brief your team. Know what you signed.
If your organization wants to work through the managed care contract review framework or model the financial implications of potential network redesign, connect with me at hfi.consulting
P.S. For the CFOs reading this: when did you last get a clause-level briefing from your managed care contracting team? Is antitrust compliance on your current risk register, or does it sit entirely with legal and outside counsel? Hit reply and tell me where this lives in your organization right now.