
CMS Interoperability and Prior Authorization Rule 2027: Who Pays, Who Falls Behind, and What CFOs Must Do Now
The Jan. 1, 2027 API deadline is exposing budget gaps and vendor risks on both sides of the payer-provider divide.
The clock on CMS's Advancing Interoperability and Improving Prior Authorization Final Rule is no longer theoretical. With a Jan. 1, 2027 compliance deadline for four separate API mandates, a new WEDI survey released at HIMSS26 makes one thing clear: a significant share of payers and providers are not ready, and the financial exposure is growing.
For finance leaders on both sides of this equation, this is not an IT problem. It is a capital planning problem, a vendor risk problem, and a workflow disruption problem that will reshape operational budgets well before the deadline arrives.
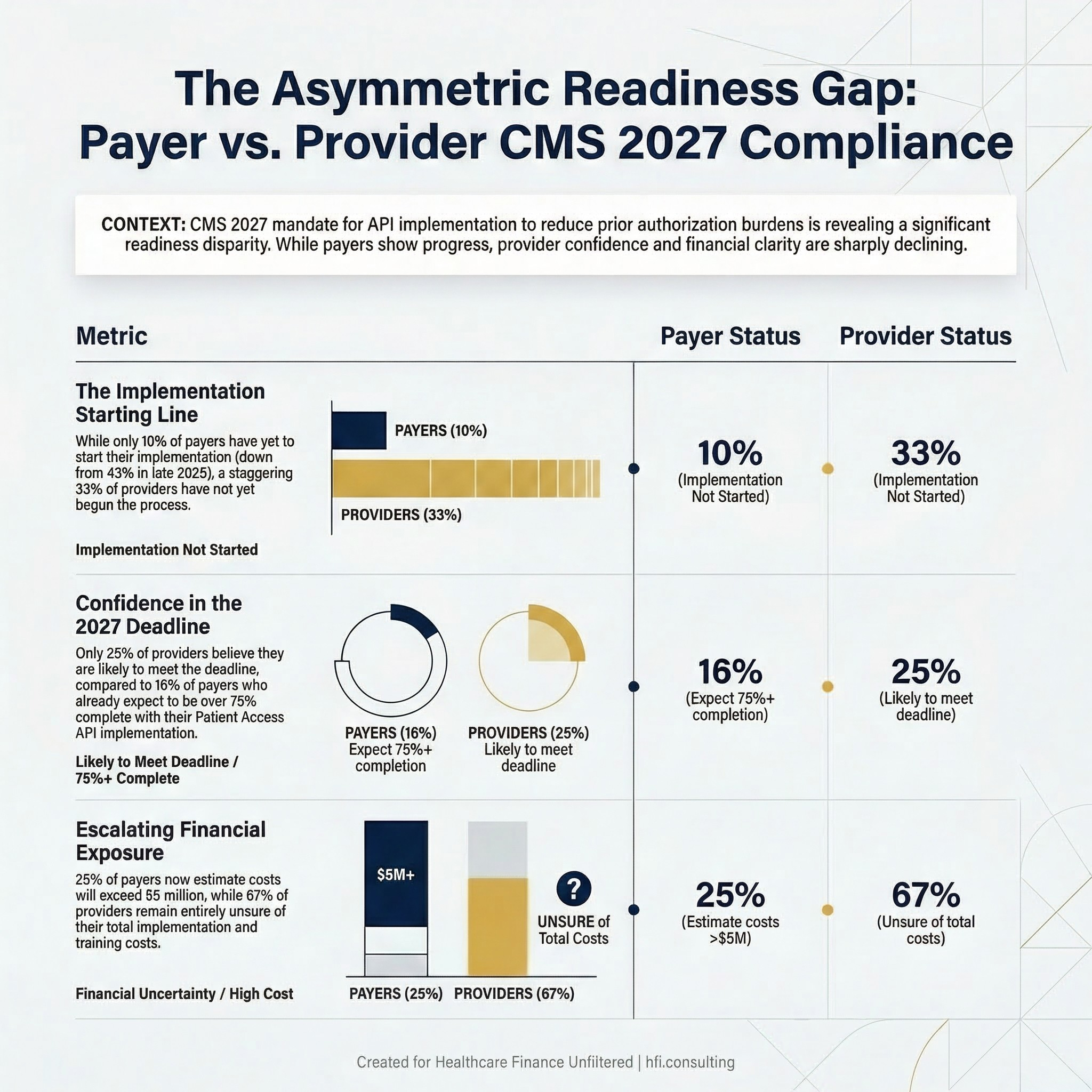
Side-by-side status comparison table Content: Payer vs. Provider readiness metrics from the WEDI Feb 2026 survey
What the Rule Actually Requires
The CMS rule mandates implementation of four API types: Patient Access, Provider Access, Payer-to-Payer, and Prior Authorization. These APIs are designed to standardize how clinical and administrative data moves between organizations, and they apply to Medicare Advantage, Medicaid managed care, CHIP, and qualified health plan issuers on the federal exchanges.
Each API serves a distinct function. Patient Access APIs give members direct access to their claims and clinical data. Provider Access APIs allow treating clinicians to retrieve patient data from payers. Payer-to-Payer APIs enable data continuity when members switch health plans. The Prior Authorization API is where the operational stakes are highest: it requires payers to respond to prior auth requests electronically within defined timeframes and to communicate decisions through machine-readable standards rather than fax or portal workarounds.
The intent is to reduce the $265 billion annual administrative cost burden that prior authorization creates across the system. The implementation reality is considerably messier.
The Readiness Gap Is Wide and Widening on the Provider Side
The WEDI survey results, which pulled responses from 83 to 86 organizations across payers, providers, clearinghouses, and vendors, paint a picture of uneven progress.
On the payer side, there is measurable movement. The share of payers that had not yet begun implementation dropped from 43% in October 2025 to 10% as of February 2026. That is real progress. But only 16% of payers expect to be 75% or more complete with Patient Access API implementation by the Jan. 1 deadline. The majority remain in early or mid-stage work.
The provider picture is more concerning. As of February 2026, 33% of providers had not started implementation of the Prior Authorization API, and 67% were unsure of their own progress. No provider respondents in this survey round had registered any measurable implementation progress. Only 25% of providers say they are somewhat or very likely to meet the Jan. 1, 2027 deadline. For context, that figure was 47% in October 2025 and 69% at the beginning of 2025. Confidence is declining, not building.
Sixty-six percent of providers now say it is extremely important that their contracted payers support the Prior Authorization API. That number has increased from 56% in the prior survey round. Providers are beginning to recognize that their own compliance depends partly on whether their payer partners deliver.
Who Is Footing the Bill
This is where finance leaders need to be paying close attention. Implementation costs are moving upward, and the final number remains unclear for most organizations.
On the payer side, 28% of survey respondents estimate costs between $1 million and $5 million for API implementation, down from 42% in October. More telling is the upward shift at the high end: 25% of payers now estimate implementation will exceed $5 million, up from 15% in October 2025. Costs are escalating as organizations move from planning into actual build and testing phases.
For providers, 67% of respondents say they remain unsure of the total cost, including employee training. That uncertainty is itself a financial risk. You cannot build an accurate budget around an unknown, and the organizations that have not yet started implementation are the furthest from understanding their true cost exposure.
The three top challenges payers identified are: third-party vendors struggling to connect with different systems, the complexity of digitizing prior authorization policies, and insufficient funding. Providers identified insufficient internal expertise, difficulties coordinating testing with vendors and health plans, and the complexity of navigating overlapping network standards including TEFCA, QHIN, and existing HIE connections.
In my work supporting financial operations across multi-hospital systems at Ascension, the pattern is familiar. When a regulatory mandate intersects with a fragmented vendor landscape, organizations with weaker vendor contract governance end up absorbing costs they did not anticipate and delays they did not plan for. The organizations that come through these transitions with the least disruption are the ones that started the vendor conversation early and built contingency into their timelines.
The Vendor Landscape: Who Has Leverage, Who Has Risk
The API compliance ecosystem currently involves EHR vendors, clearinghouses, third-party interoperability platforms, and payer technology vendors. Compliance does not sit cleanly in any one vendor's domain, which creates a coordination challenge that becomes a financial risk.
EHR systems are at the center of the provider-side implementation. Epic has been building FHIR capabilities for years, and its Patient Access and Provider Access API infrastructure is relatively mature for organizations on its platform. But even Epic has limitations. At HIMSS26, Providence Health noted that some EHR systems still limit how patient populations can be managed dynamically, and that bulk data exports remain constrained by underlying infrastructure.
This matters for the Prior Authorization API specifically. The PA API requires real-time or near-real-time data exchange. If the EHR cannot support the volume or frequency of those requests, the compliance gap shifts from a payer problem to a joint infrastructure problem. Finance leaders need to have explicit conversations with their EHR account teams now about what is included in current contracts versus what requires additional licensing or professional services.
On the payer side, clearinghouses and third-party API platforms are a significant piece of the puzzle. Organizations using delegated third parties to manage API connections are experiencing some of the highest friction, because each vendor has its own integration timeline and testing requirements. The WEDI survey identified this as the top payer implementation challenge.
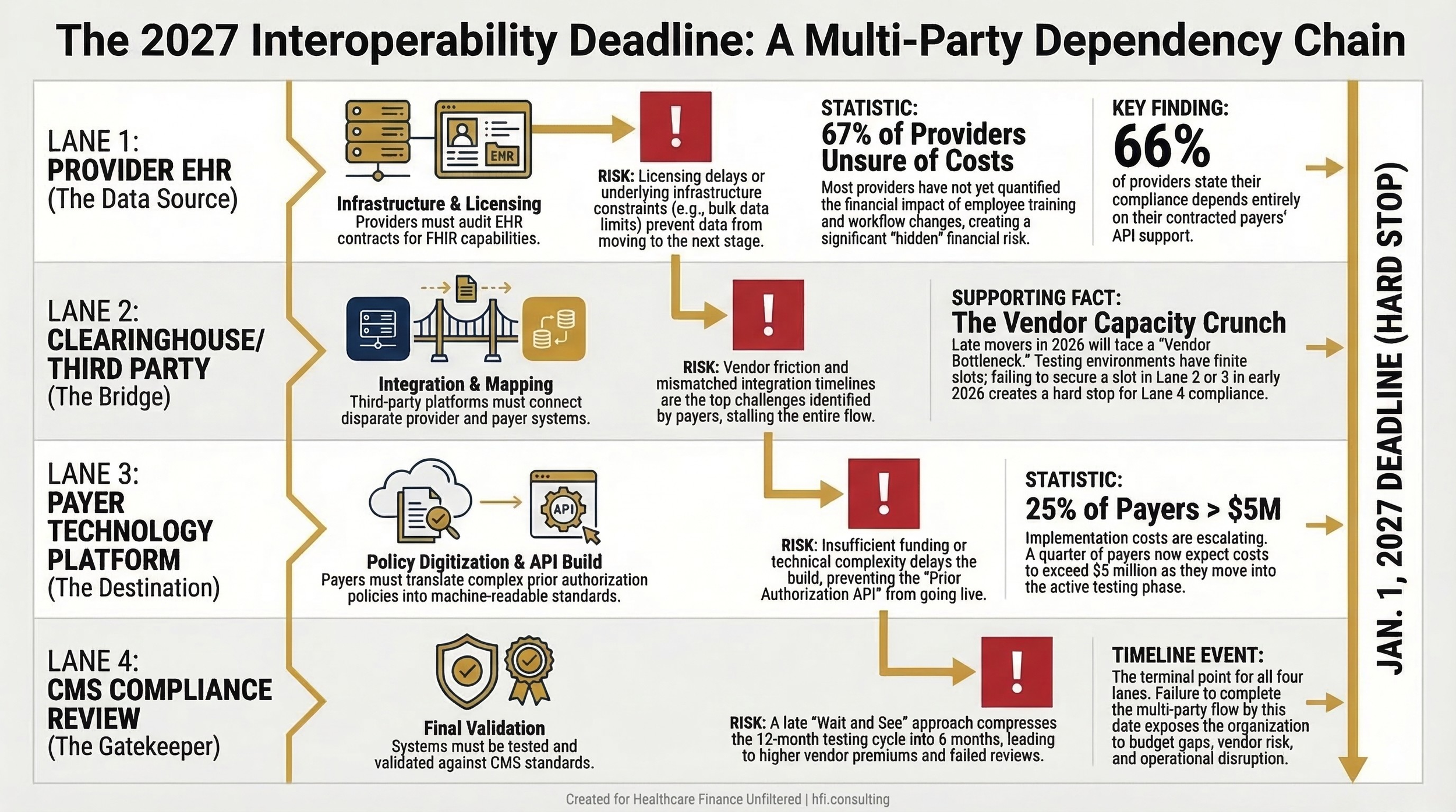
Process flow diagram Content: Four-lane swim lane diagram showing API implementation dependencies.
What "Wait and See" Actually Costs
Some organizations are taking a wait-and-see posture, hoping for a deadline extension or regulatory softening under the current administration. This is not an unreasonable read of the political environment, but it carries real financial risk.
Deadline extensions under CMS have historically been partial, not comprehensive. An extension for one API type does not necessarily apply to others. Organizations that pause implementation to wait for regulatory clarity often find themselves compressing a 12-month build-and-test cycle into six months, which increases vendor costs, requires more expensive contract modifications, and generates the kind of operational disruption that affects claim adjudication timelines and authorization turnaround metrics.
From the payer side at Florida Blue Medicare, one of the clearest patterns in regulatory compliance is that late movers pay a premium. Vendors prioritize implementation capacity for early clients. Testing environments have finite slots. When you are competing for vendor attention in Q3 of a Q4 deadline year, you are not getting the best pricing or the best service.
The organizations currently expressing the most uncertainty about their progress are likely to face the highest cost pressure over the next nine months.
Bulk FHIR: The Longer-Term Financial Opportunity
While most of the immediate compliance conversation centers on Prior Authorization APIs, finance and technology leaders should be aware of a parallel development that carries significant upside for analytics and population health strategy.
Bulk FHIR, a capability introduced under the 21st Century Cures Act, allows organizations to extract standardized clinical data across entire patient populations rather than one patient at a time. Unlike the real-time APIs at the center of the interoperability rule, Bulk FHIR operates as a batch-style export that can feed analytics platforms, risk models, and data pipelines.
For payers operating Medicare Advantage programs and value-based contracts, this is directly relevant to risk adjustment accuracy and population health management. For providers in shared savings arrangements, it creates the infrastructure to analyze utilization patterns and close care gaps at scale.
Leaders at HIMSS26, including clinicians from MultiCare Health System and Providence Health, described Bulk FHIR as foundational infrastructure for AI applications in healthcare. The bottleneck, as several noted, is still EHR infrastructure. Getting large patient population datasets out of EHR systems reliably at scale remains technically constrained. But organizations that invest in solving that bottleneck now are building capabilities that will support analytics and AI strategy for years beyond the 2027 compliance deadline.
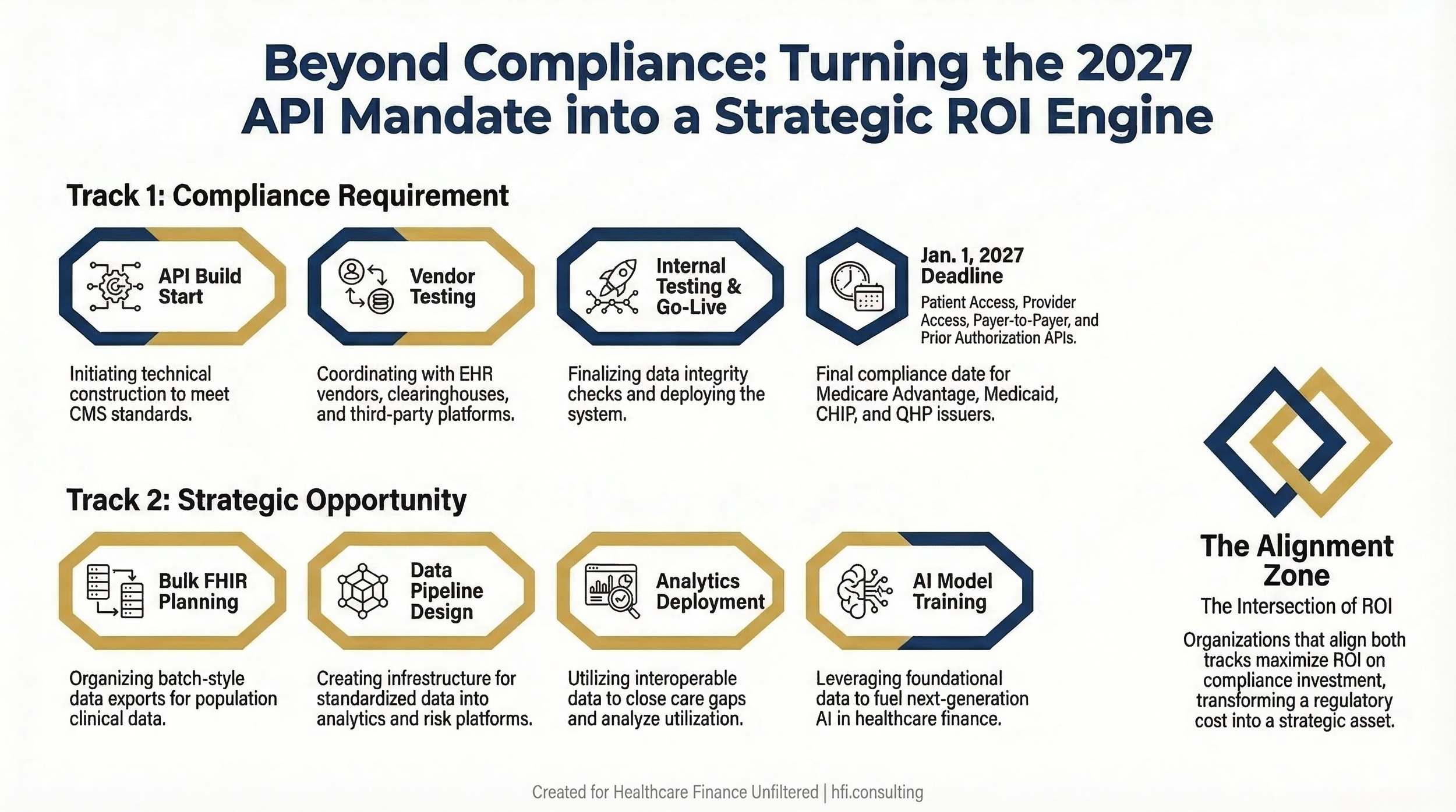
Timeline graphic with dual tracks Content: Two parallel timelines
What Finance Leaders Should Be Doing Right Now
For CFOs and VP Finance on both sides of the payer-provider relationship, the next 90 days are the most critical window before implementation costs escalate further and vendor capacity tightens.
Audit your current vendor contracts. Identify which APIs each vendor is responsible for, what their current implementation timeline is, and what the contract language says about delays or scope changes. If your clearinghouse or EHR vendor is behind, you need to know now, not in October.
Build a dedicated implementation budget line. If you are still carrying API implementation as a general IT budget item, you are likely underestimating the cost and underresourcing the project. Given that 25% of payers now estimate costs above $5 million, organizations that have not budgeted at this level should revisit their assumptions.
Assess your payer or provider counterpart readiness. If you are a provider, you need to know whether your contracted payers are on track. If you are a payer, you need to understand what your provider network is asking for and whether your implementation timeline aligns with their clinical workflow needs. This is a negotiating leverage question as much as a compliance question.
Quantify the prior auth workflow change. The Prior Authorization API will fundamentally alter how authorization requests are submitted, tracked, and adjudicated. For providers, this intersects directly with denial rates and revenue cycle performance. Finance leaders need scenario models for what happens to denial volume and authorization approval timelines if implementation is delayed or incomplete.
Plan for Bulk FHIR as a second phase. If your organization is managing value-based contracts or risk-bearing payment models, Bulk FHIR investment belongs in your 2027 strategic plan, not your IT wish list.
"CFO Perspective: The organizations that treat interoperability compliance as a joint finance-operations priority, not just an IT project, are the ones that will come through 2027 with the least budget damage and the most strategic optionality."
If you are working through API implementation budget modeling or vendor contract risk assessment for the interoperability rule, I would welcome the conversation. Hit reply and let me know where you are in the process. I am hearing from finance leaders on both sides, and the variance in organizational readiness is significant.
For more on managing technology vendor risk in healthcare, , see AI-Powered Revenue Leakage Prevention: The CFO's Implementation Guide for 2026 and CMS Medicaid Fraud Crackdown 2026: What Hospital Finance Leaders Must Do Now.
The Bottom Line
The CMS Interoperability and Prior Authorization Final Rule is not going away, and the Jan. 1, 2027 deadline is closer than most organizations' current implementation timelines suggest. One-third of providers have not started. Implementation costs for payers are already exceeding initial estimates. Vendor capacity will tighten as the deadline approaches.
Finance leaders who treat this as exclusively an IT problem will end up managing an unbudgeted crisis in 2026. The ones who build dedicated budget lines, audit vendor contracts now, and coordinate across payer-provider relationships will be better positioned operationally and financially when the deadline arrives.
Interoperability is not a one-time project. It is the infrastructure for everything that comes next: AI, population health, risk adjustment, and value-based payment sustainability. The organizations that invest smartly now are not just achieving compliance. They are building the data foundation for the next decade of healthcare finance.
P.S. Where does your organization stand on API implementation right now? Are you on track, behind, or still working through vendor contracts? Hit reply and tell me which challenge is hardest to solve from where you sit.