
The AI Automation Trap: Why Healthcare Finance Leaders Are Quietly Walking Back Their Biggest Bets
Over 70% of health systems use AI in operations. Most are not getting the ROI they were promised. Here is why the operating model is the problem.
Healthcare organizations are spending real money on AI and getting disappointing results. Industry data suggests the majority of healthcare AI automation projects fail to deliver projected ROI, and many are abandoned or significantly scaled back within 18 months of launch.
That number should stop every CFO reading this. Not because AI is a bad investment. Because the operating model surrounding the AI is almost always the problem, and finance leaders are the ones left holding the margin gap.
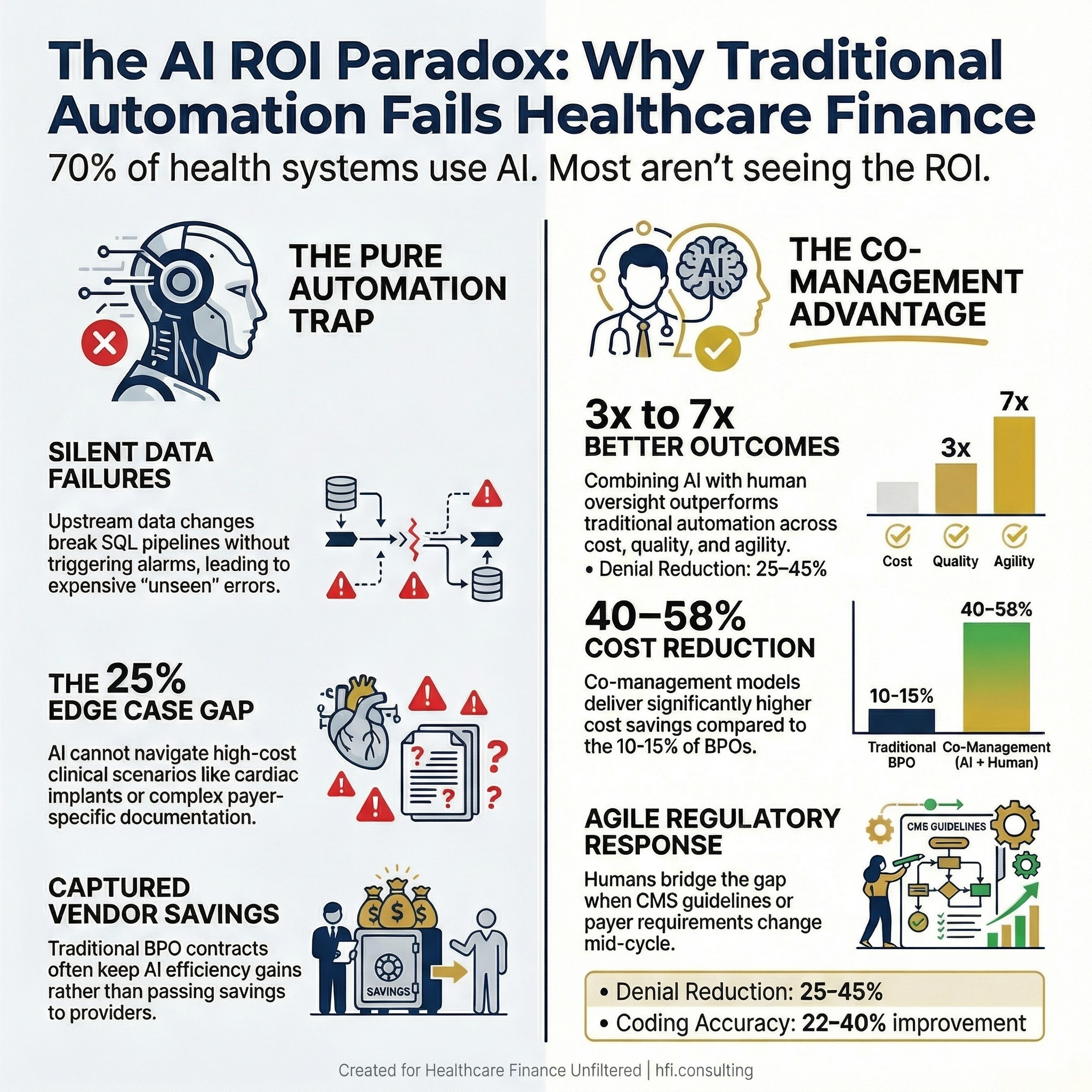
Infographic showing 70% of health systems use AI but most fail to achieve projected ROI, comparing pure AI vs. AI plus human co-management outcomes
The Silent Failure No One Talks About
Most AI failure stories in healthcare never make it to a conference presentation. They get absorbed into a budget variance, blamed on "implementation challenges," or quietly fixed by someone on the team who figured out what broke.
At Florida Blue Medicare, we use automated pipelines and algorithms that read claims and other points of member data daily. When source data changes upstream, those automations stop working. A missing table here, a new field in a dataset throwing off the SQL there, and suddenly the daily processing halts with no alarm.
The problem is that nothing looks wrong on the surface. The job appears to have run. The member data just does not look quite right.
It was not until I built a dedicated monitoring page into our dashboard that we could see, every single day, whether each job had actually completed successfully. Before that layer existed, we were operating on the assumption that if no one was complaining, the automation was working. That assumption is expensive.
This is a failure mode that vendor pitches and implementation timelines do not account for. The AI works exactly as designed, until the data environment changes. And in healthcare, data environments change constantly.
Why Vendors Oversell and What It Costs You
The Florida Blue situation was a maintenance failure. The second category of AI breakdown is more corrosive because it happens at the point of sale.
When I worked at McKesson, in what is now Change Healthcare, I was a Business Advisor during Performance Analytics implementations. The product worked as designed. That was not the issue.
The issue was that every health system had homegrown metrics they had built over years. Custom productivity calculations, service line margin definitions, cost-per-encounter formulas specific to their payer mix and documentation standards. When a new system went live, those metrics could not be replicated out of the box. The back-end configuration required to match a health system's existing calculations was consistently scoped out of the project.
I could sit across from a CFO or a VP of Finance and see exactly what they needed. The calculation was not complicated. But getting the system to produce it on their timeline, within the contracted scope, was a different conversation entirely.
That gap between what sales demonstrates and what implementation delivers is where trust erodes. It is also where the real cost lands, because the finance team now has two systems: the new AI-enabled platform they bought and the spreadsheets they never stopped running.
The Edge Case Problem Healthcare AI Cannot Solve Alone
The failure modes above are operational. The third category is structural, and it matters more.
AI systems trained on common claim types and documentation patterns cannot handle the long tail of clinical scenarios: rare diagnoses, complex comorbidities, non-standard payer rules, and unusual coverage situations. When these edge cases represent 15 to 25% of volume, which is typical in medical coding, prior authorization, and denial management, pure automation creates dangerous gaps.
At Ascension, across the seven hospitals where I worked on financial operations, the clearest example was high-cost cardiac implant reimbursement. Procedures like TAVR (transcatheter aortic valve replacement) and the Watchman device carry significant implant costs. Payers contract for those reimbursements, but getting paid within contract prices is not automatic.
We would ultimately get paid. But it could take months of investigation. Pulling the operative report. Matching implant invoice dates to the claim. Cross-referencing payer-specific billing requirements for these device categories. Escalating to the right contact at the payer when the initial payment came in short.
An AI does not know where to look for that documentation. It does not know which payer contacts to escalate to. It does not know how to read an operative report alongside a remittance advice and identify the gap. That investigation is human work, and the dollar amounts at stake make that distinction matter.
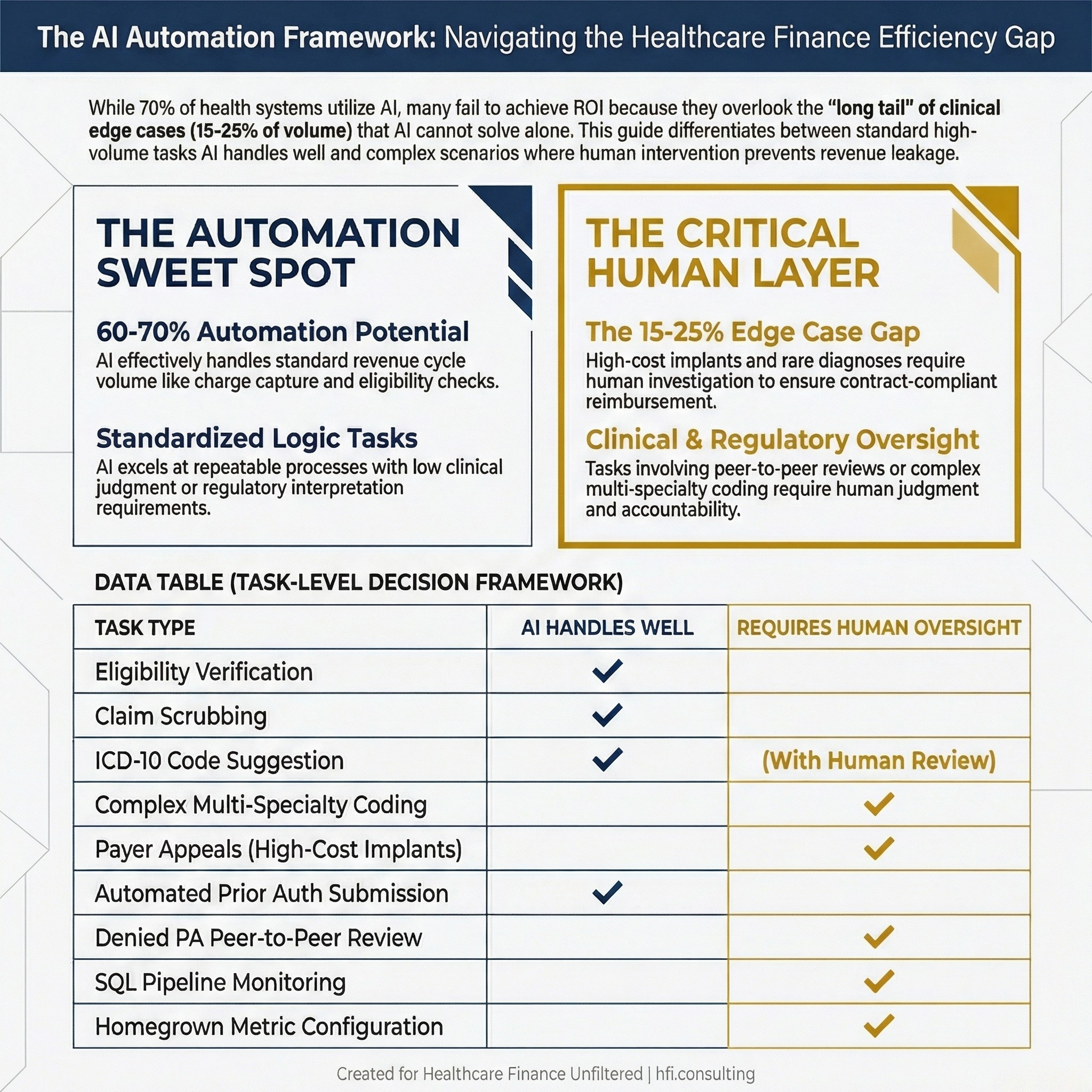
Table comparing which healthcare revenue cycle tasks AI handles well versus which require human oversight, covering coding, prior auth, payer appeals, and data monitoring
The Misaligned Incentive Nobody Puts in the Contract
Traditional Business Process Outsourcing economics are built on headcount. Vendors profit by maximizing the number of full-time equivalents deployed to client accounts. This creates a fundamental misalignment: AI automation reduces headcount, which reduces vendor revenue.
The practical consequence is that when your BPO vendor implements AI, they have no structural incentive to pass the efficiency gains back to you. The savings stay on their side of the ledger.
Consider a scenario where a health system engages a BPO to manage 80 FTEs performing medical coding, denial management, and prior authorization. The BPO implements AI that enables 25 specialists to handle the workload previously requiring 80, a 69% efficiency gain. Under traditional BPO pricing, the client continues paying the same monthly rate. The BPO's actual labor cost drops substantially. The client sees zero cost reduction despite significant automation.
For a healthcare organization running on 2 to 3% margins, that is not a vendor relationship. That is a revenue capture mechanism pointed at your operating budget.
The structural alternative is a co-management model, where organizations maintain direct control over workflows and technology selection, and pricing is tied to actual FTEs deployed. When AI reduces headcount requirements, costs drop proportionally. The efficiency gain stays with the organization.
This distinction does not show up in vendor presentations. It shows up in contract terms, and in the variance analysis 18 months after go-live.
If you want a framework for evaluating AI vendor ROI before signing, the analysis I published on revenue leakage prevention covers the CFO-level calculation framework: AI-Powered Revenue Leakage Prevention: The CFO's Implementation Guide for 2026
What the Performance Data Actually Shows
The case study data on AI plus human co-management versus traditional BPO is not close.
Organizations implementing co-management approaches achieve 40 to 60% cost reductions in targeted functions while simultaneously improving quality metrics and maintaining full HIPAA compliance. Co-management implementations deliver 3 to 7 times better outcomes across cost, quality, compliance, and operational agility dimensions.
The specific metrics matter for finance leaders building a business case:
Cost reduction: 40 to 58% under co-management versus 10 to 15% under traditional BPO. Coding accuracy improvement: 22 to 40% versus 3 to 8%. Denial rate reduction: 25 to 45% versus 5 to 10%. Workflow iteration cycles: 15 to 20 per year versus 2 to 3. HIPAA compliance incidents: 50 to 70% fewer under co-management.
The operational agility difference is particularly relevant given how frequently CMS updates coding guidelines, payers adjust prior authorization requirements, and documentation standards shift. Healthcare organizations report 4 to 8 week delays for even minor workflow modifications under traditional BPO contracts, a timeline that is unacceptable when payer policies change mid-cycle or coding updates take effect.
If your organization is evaluating an AI implementation or renegotiating a BPO contract in the next 12 months, I want to hear about the specific friction points you are navigating. Hit reply and tell me what is actually breaking down, or where the vendor promise is not matching operational reality. I read every response.
A Framework for Deciding What to Automate and What to Protect
The right question for a CFO is not "how much can we automate" but "where does automation create risk we are not pricing in."
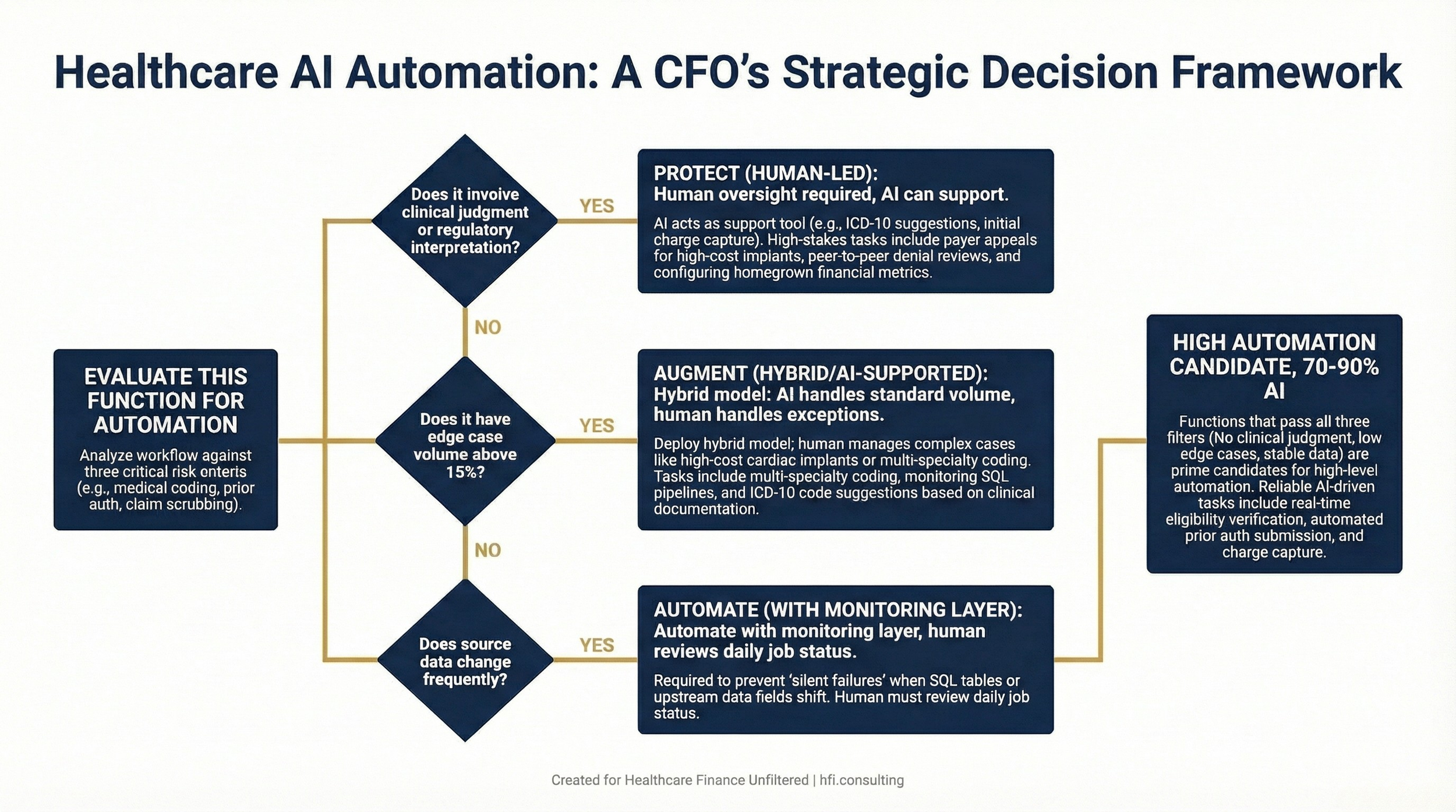
Decision flowchart for healthcare CFOs evaluating which revenue cycle functions to automate, augment with AI, or keep under human oversight, based on clinical judgment requirements, edge case volume, and data stability
The functions where full automation consistently underperforms in healthcare finance:
Payer appeals requiring clinical documentation review. High-cost implant and device reimbursement disputes. Prior authorization denials that require peer-to-peer escalation. Any coding scenario where a single case involves multiple specialties, unusual comorbidities, or a payer with non-standard rules. Monitoring automated pipelines for silent failures.
The functions where AI delivers clear, measurable efficiency gains without requiring human replacement:
Automated charge capture, initial code suggestion from clinical documentation, real-time eligibility checks, claim scrubbing against payer-specific edits, and predictive denial analytics handle 60 to 70% of standard revenue cycle volume effectively.
The practical implication: build your AI strategy around the 60 to 70% that automation handles reliably, and invest the human capital you free up into the 15 to 25% of complex cases that drive disproportionate revenue recovery.
The HIPAA Dimension CFOs Cannot Afford to Ignore
Every AI tool deployed in a healthcare workflow creates a new data handling pathway. That is not theoretical; it is a compliance exposure that needs to be mapped before deployment, not after.
AI tools in healthcare workflows require full visibility into which tools process protected health information, how data flows between systems, and what safeguards are in place. Clear audit trails showing which decisions were made by AI versus humans are essential for CMS audits, payer audits, and False Claims Act inquiries.
Under the False Claims Act, incorrect billing is a liability regardless of whether a human or an algorithm made the coding decision. That accountability does not transfer to your vendor. It stays with your organization.
This is why the transparency dimension of any AI vendor relationship is not a nice-to-have. It is a financial risk management question.
What This Means for Your Planning Horizon
Healthcare AI is not going away, and it should not. The efficiency gains in the functions where it actually works, claim scrubbing, eligibility verification, coding suggestion for standard encounters, prior auth routing for straightforward cases, are real and material.
The CFOs who will capture those gains are the ones who go into vendor negotiations with a clear-eyed assessment of what automation can and cannot do, who retain contractual control over workflows and technology selection, and who build monitoring into the model rather than assuming silent automation means working automation.
The CFOs who will get burned are the ones who buy the full automation story, let vendors capture the efficiency savings, and find themselves 18 months in with the same headcount costs and a new system their team is working around.
The hidden truth in healthcare AI is not that the technology fails. It is that the operating model around it fails, and the contracts are written so that failure stays on your balance sheet.
Healthcare Finance Unfiltered covers the operational and financial realities that do not make it into vendor white papers. If you are not already a paid subscriber, the frameworks and analyses that go deeper than this are behind the paywall. Subscribe at rachelbarksdale.substack.com or connect with me at hfi.consulting
P.S. I want to know specifically: has your organization experienced a silent automation failure, a vendor promise that did not survive implementation, or a complex case where you had to pull a human back in? Hit reply. No vendor pitches, just finance leaders talking to finance leaders.