
Healthcare Analytics 2026: The CFO's Guide to Solving Old Problems with New Tools
From virtual nursing to Bulk FHIR, the analytics solutions reshaping margins and outcomes are more accessible than you think.
Your analytics stack is probably three to five years behind what the market can actually deliver today. That gap is costing you margin, staff hours, and patient outcomes you cannot get back.
The healthcare organizations seeing the biggest operational wins right now are not the ones with the largest IT budgets. They are the ones with leaders willing to ask whether the way they have always done something is still the best way to do it.
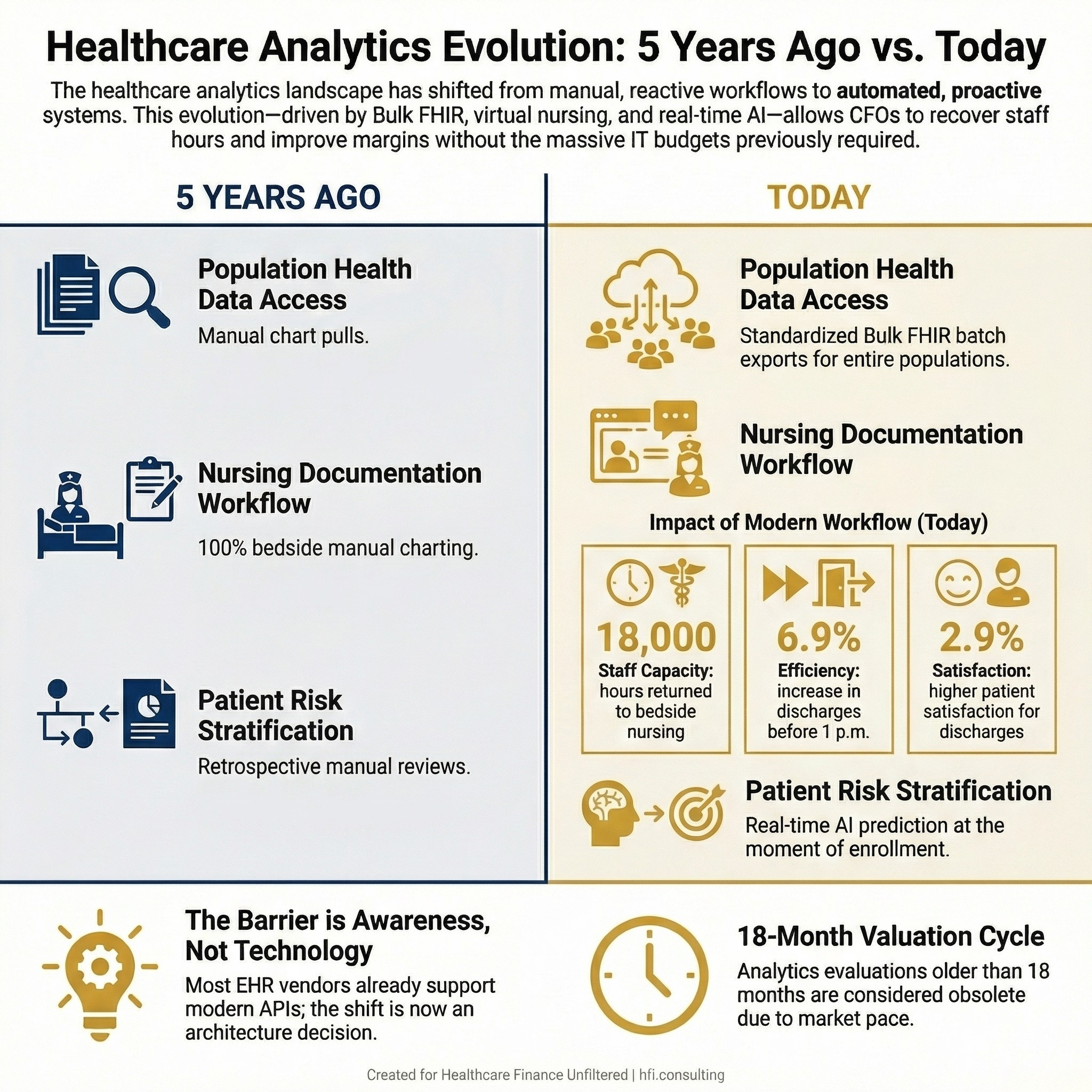
Infographic comparing healthcare analytics capabilities from 2021 to 2026, showing advances in Bulk FHIR, virtual nursing, and AI-powered risk stratification.
The Problem Nobody Wants to Say Out Loud
Healthcare CFOs are operating in one of the most data-rich environments in any industry. They also have some of the least accessible, least actionable data of any sector their size.
The conventional response has been to hire a consulting firm, buy a new platform, and build toward a five-year roadmap that costs eight figures before it produces a single insight. That approach is not wrong. It is just increasingly unnecessary for many of the problems finance leaders are actually trying to solve.
The real issue is that our mental model of what analytics costs, what it requires technically, and what is realistically achievable has not kept pace with the market. Solutions that needed an enterprise data science team three years ago now come as configurable modules. Tools that required months of implementation can be operational in weeks. And the use cases that generate the fastest ROI are not the glamorous AI projects your vendor is pitching. They are workflow problems you have already identified and set aside because you assumed the solution was out of reach.
What "Thinking Outside the Box" Actually Means for a CFO
The phrase gets overused, but in a healthcare finance context it has a specific and practical meaning: it means evaluating a problem without assuming the solution has to look like the last solution you bought.
Three categories of analytics problems deserve a second look right now.
Data access problems. Many health systems are still pulling population-level data through manual chart reviews or fragmented extracts from multiple systems. Bulk FHIR APIs, which matured significantly under the 21st Century Cures Act, now allow organizations to extract standardized datasets across entire patient populations through a single batch-style approach. At HIMSS26, leaders from MultiCare Health System and Providence described using Bulk FHIR to feed analytics platforms and support risk modeling at scale. The technology is not new. Most of your EHR vendor already supports it. The barrier is not availability; it is awareness.
Workflow time problems. When Sentara Health implemented a virtual nursing platform across its system, the goal was not just technology adoption. It was care team redesign. The result in year one was 18,000 hours returned to bedside nursing staff through more than 59,000 virtual nursing sessions. Discharges before 1 p.m. increased by 6.9%, and patient satisfaction scores for virtual discharge interactions came in 2.9% higher than for in-person discharge. These are finance metrics. Hours recovered and LOS improvement translate directly to throughput and labor cost per adjusted discharge.
Prediction problems. The pharmaceutical patient services space offers a case study worth importing into provider and payer analytics strategy. Patient services teams have moved from waiting to see which patients abandon their prescriptions to using AI models that estimate abandonment risk at the moment of enrollment. The same logic applies to readmission prediction, prior authorization delays, and denial pattern identification. The shift from reactive to proactive is not a technology problem. It is an architecture decision.
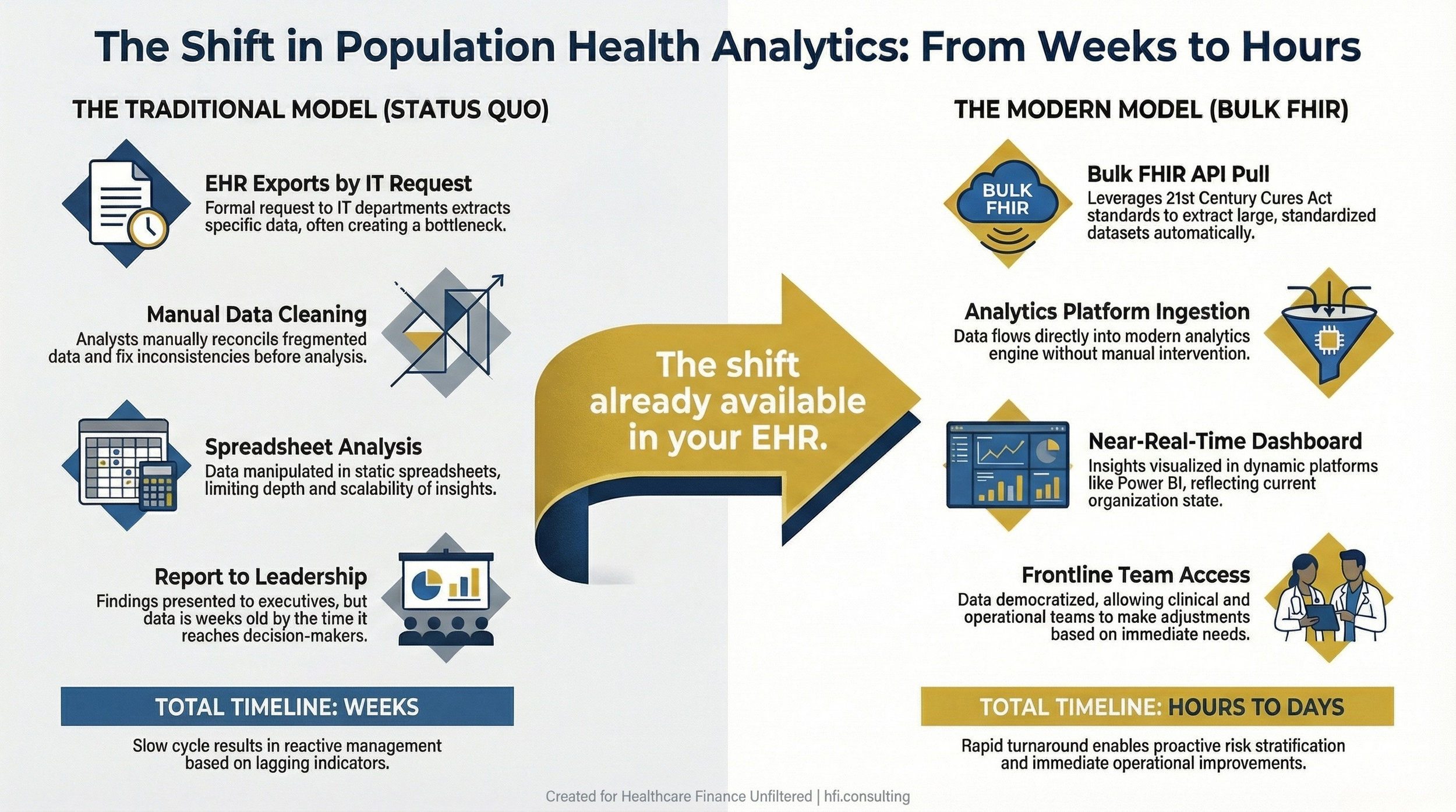
Process flow diagram comparing traditional EHR data extraction timelines with Bulk FHIR API-based population health analytics workflows.
The Staff-Building Argument That Keeps Getting Skipped
There is a pattern in healthcare that deserves to be named directly. When a new analytics problem surfaces, the default response is to scope an RFP, evaluate vendors, and bring in an outside firm to build and manage the solution. That decision is sometimes correct. It is also sometimes a way of avoiding a harder internal conversation about capability development.
When East London NHS Foundation Trust embarked on a decade-long analytics transformation, one of the two foundational decisions its leadership made was to build technical skill within the team. The other was to design data access around what frontline teams needed, not what the board wanted to see. The result was a cloud-based data warehouse, near-real-time dashboards in Power BI structured at the team level, and HIMSS AMAM Stage 6 achievement in December 2025, becoming the first organization in the EMEA region to do so under updated requirements.
That transformation was not driven by a consulting engagement. It was driven by internal capability development over time.
In my work at Ascension across seven hospitals, I watched the difference between teams that understood the data they were working with and teams that were entirely dependent on IT or outside analysts to pull and interpret it. The teams with internal analytics fluency moved faster, caught errors faster, and built better business cases. The teams that outsourced all interpretation often got accurate data and wrong conclusions, because the people doing the interpreting did not know the operational context.
This is not an argument against vendor partnerships. It is an argument for investing in your own people alongside any technology purchase. If your finance team cannot read and interrogate a Power BI dashboard, you do not have an analytics strategy. You have a reporting subscription.
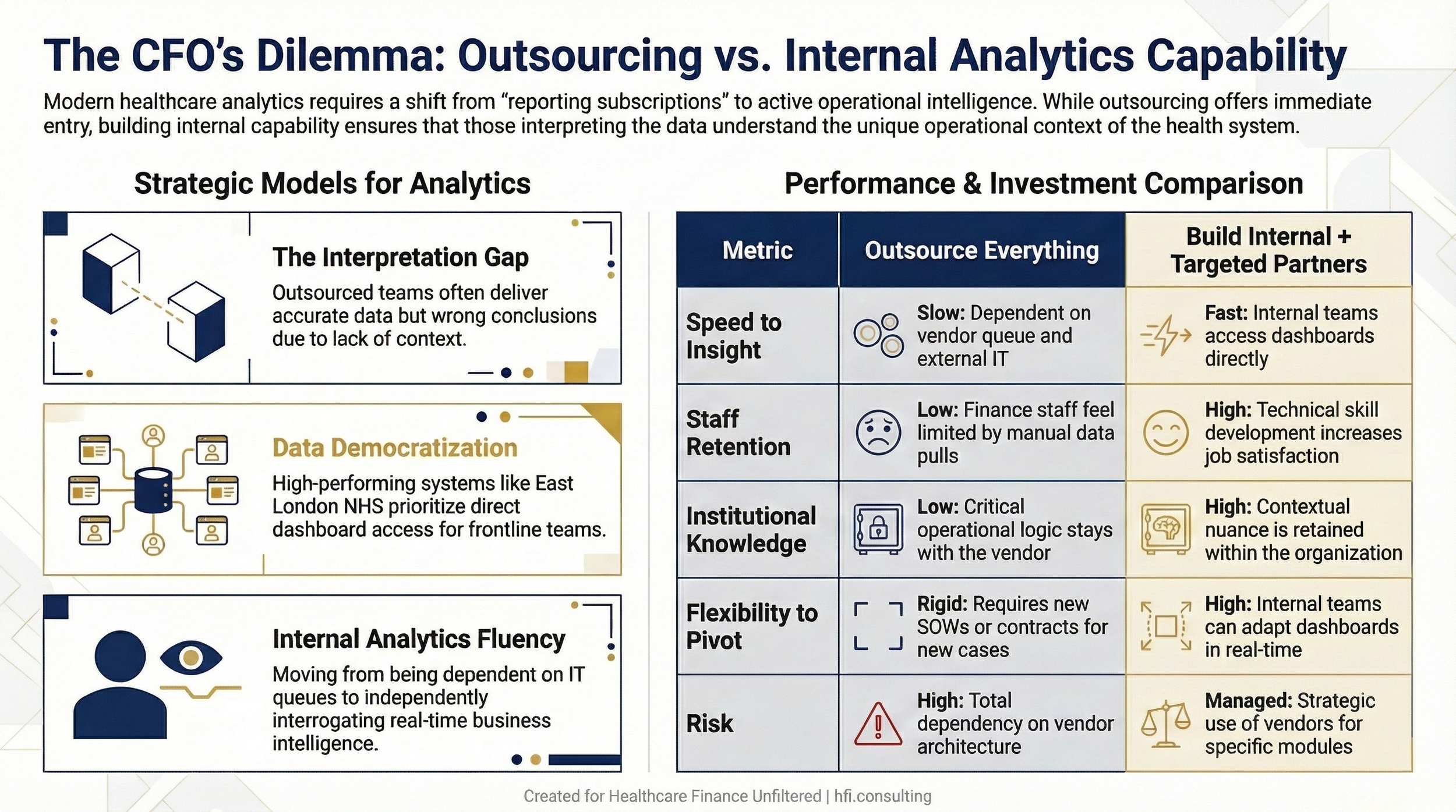
Comparison table contrasting fully outsourced analytics models with hybrid approaches that combine internal team development and targeted vendor partnerships
Practical Entry Points That Do Not Require a Full Platform Overhaul
The organizations referenced in this article are not all large academic medical centers with unlimited capital. The Sentara virtual nursing model started with 11 positions and transitioned to virtual delivery without a single layoff. The analytic approach at East London NHS began with a decision about design principles, not a technology purchase. Bulk FHIR adoption at MultiCare and Providence is happening alongside, not instead of, existing EHR infrastructure.
The practical entry point for most CFOs is identifying one problem that is costing measurable money or hours, then asking whether a solution that would have seemed impractical three years ago might actually be available and affordable today.
Some concrete starting points by problem type:
If your problem is labor cost per discharge or LOS, look at what virtual care delivery options exist within your current EHR and telehealth vendor relationships before scoping a new procurement. Sentara built its virtual nursing program on existing infrastructure and focused primarily on care team redesign and shared governance.
If your problem is population-level risk stratification for value-based contracts, pull a conversation with your EHR vendor about Bulk FHIR readiness. Ask specifically whether the API can export your attributed population in a single batch and what restrictions exist on record volume. The bottlenecks are usually EHR-side infrastructure limits, not regulatory barriers.
If your problem is prior authorization denial rates or payer-side claims pattern analysis, the predictive models being used in pharmaceutical patient services, which flag patients at risk of prescription abandonment before they drop out, use the same underlying logic as denial prediction models. The data inputs are different. The architecture is not.
If your problem is finance team productivity and report turnaround, the East London NHS approach of democratizing data access, putting near-real-time dashboards directly in the hands of frontline teams rather than routing all requests through IT, cuts report cycle time significantly while building analytical capability across the organization.
None of these requires a greenfield technology build. All of them require a CFO willing to sponsor a conversation that does not start with "what can we afford" but instead starts with "what is this problem actually costing us, and what has changed in the market since the last time we looked at it."
I covered the ROI case for AI in revenue cycle in more detail here: AI-Powered Revenue Leakage Prevention: The CFO's Implementation Guide for 2026. The framing on building the internal business case before engaging vendors applies directly to analytics investments as well.
The Compliance and Privacy Framing That Slows Good Decisions
One of the most common reasons analytics projects stall is a compliance concern that turns out to be resolvable. HIPAA does not prohibit modern analytics. It establishes standards for how data is accessed, stored, and used.
Organizations using AI for patient services are running models against anonymized, aggregated patient data stored inside organizational firewalls. Patients are assigned random identifiers at enrollment. Outreach is pre-authorized. The system can track patient movement across vendors and care settings without compromising protected health information.
If your compliance team has said "we cannot do that because of HIPAA," and no one has gone back with a specific technical architecture for review, that conversation is worth reopening. The answer may still be no. But in many cases, the answer is yes with guardrails, and the guardrails are already built into the platforms your vendors are offering.
For CFOs thinking about how technology investment decisions intersect with IT contract risk, the issues I covered in the Epic interoperability context apply here too. Machine Learning in the OR: The Real Cost of Doing Nothing and AI Medical Scribes: The ROI Case Healthcare Finance Leaders Need Before Budget Season both address how to frame the cost of inaction when evaluating analytics and AI investments. Retrieve these URLs from your Substack dashboard for internal linking.
"The question is not whether your organization can afford to invest in better analytics. At 2-3% operating margins, the question is whether you can afford not to. Every month you are running on lagging indicators is a month of margin erosion you will not get back."
-- CFO perspective, multi-hospital health system
Building the Internal Business Case
Before you take an analytics proposal to your board or your CFO peers, the business case needs to answer three questions in this order.
What is the current cost of the problem? This means hours, denials, LOS days, staff turnover attributable to administrative burden, or whatever metric is most relevant to the use case. Sentara calculated hours returned to bedside nursing. East London NHS tracked whether care was improving over time, not just what the current snapshot showed. You need a denominator before you can calculate a return.
What has changed in the market since we last looked at this? If your last analytics vendor evaluation was more than 18 months ago, it is out of date. The pace of capability development in healthcare AI and analytics has been faster than most procurement cycles can track. Do a current-state market scan before you write a scope of work.
What internal capability do we need to develop alongside any technology purchase? If the answer is "our team will use whatever the vendor provides," that is not a capability plan. Identify specific roles, training resources, and milestones for building internal analytics fluency.
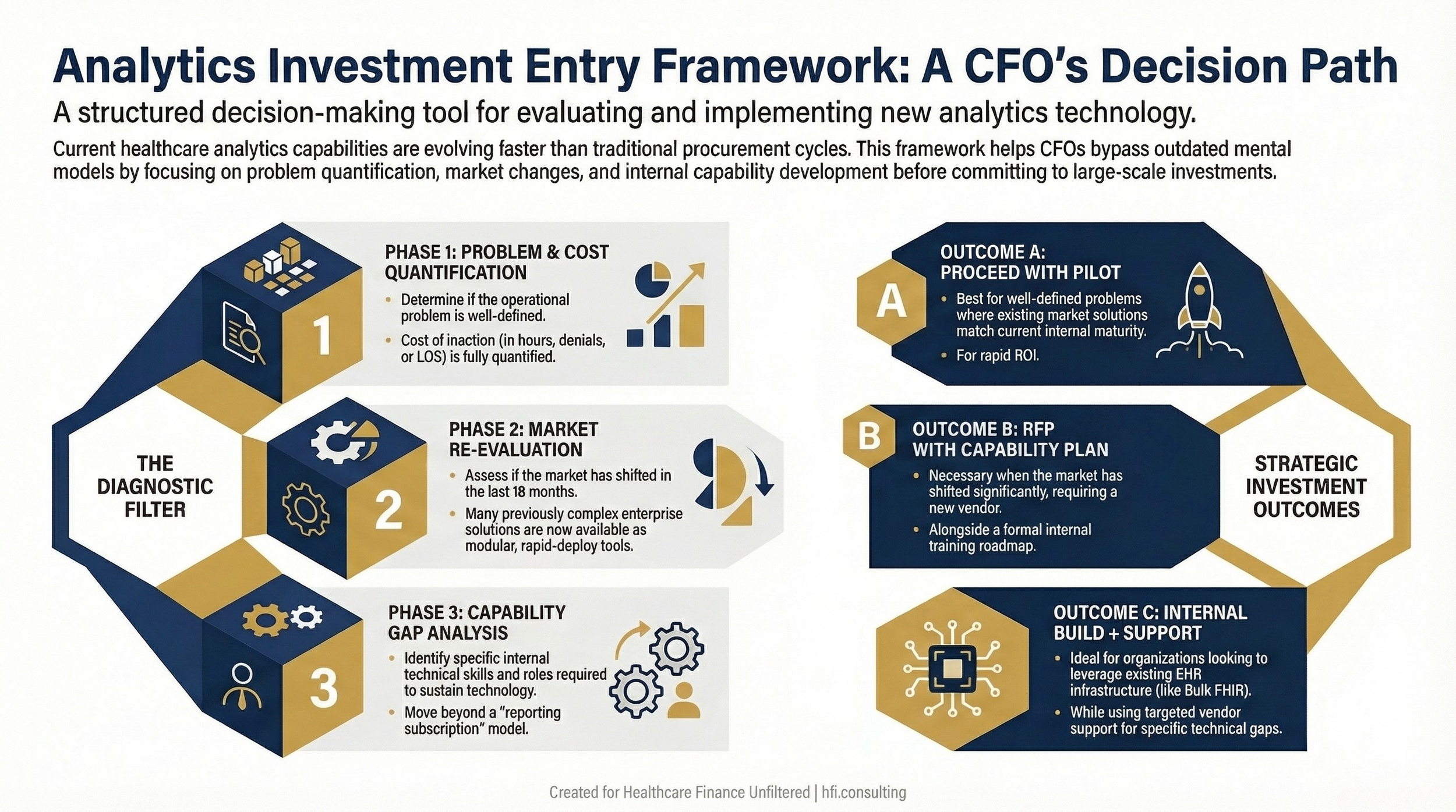
Decision tree framework for healthcare CFOs evaluating analytics and AI investment decisions, covering problem definition, market assessment, and internal capability planning.
What to Do This Week
The goal of this article is not to convince you that AI will solve your budget problems. It will not, at least not without the organizational work required to use it well.
The goal is to challenge one assumption: that the analytics problem you have been sitting on is still as expensive or technically complex to address as it was the last time you looked at it.
Pick one. Identify the cost. Ask whether the market has moved.
That is the conversation worth having right now.
If you are working through an analytics vendor evaluation or trying to build the internal business case for a population health or revenue cycle analytics investment, I am happy to think through the framework with you. Hit reply and tell me what problem you are trying to solve. I read every response.
The Harder Truth About Analytics Maturity
Healthcare organizations have been told for fifteen years that they are on the cusp of becoming truly data-driven. Most are not there yet, and most know it.
But the gap between "not there yet" and "making meaningful progress with available tools" has narrowed considerably. The organizations in this article, a UK NHS trust, a large U.S. health system, pharmaceutical patient services teams, and the interoperability leaders presenting at HIMSS26, are not outliers with unique resources. They are organizations that decided to ask a different set of questions about problems they had been managing the same way for years.
The technology has moved. The question is whether your organization's willingness to evaluate it has kept pace.
Healthcare Finance Unfiltered publishes practical analysis for CFOs and finance leaders navigating the operational and strategic decisions that do not make the trade press. If this framing is useful, subscribe for weekly coverage at hfi.consulting
P.S. What is the analytics problem in your organization that keeps getting pushed to next year's roadmap? I am genuinely curious whether it is a budget issue, a compliance concern, a vendor limitation, or something else entirely. Hit reply and tell me. Responses to this question have been some of the most useful conversations I have had with readers this year.