
Healthcare Process Automation: CFO Guide to FHIR, AI Workflows, and Operational Intelligence Beyond Revenue Cycle
Most health systems automate billing first and everything else never. Here is the framework for changing that.
A new Peterson Health Technology Institute (PHTI) report landed in April with a finding that should be uncomfortable for any finance leader who has been selling automation as a cost-reduction story. AI may actually be increasing healthcare costs by accelerating transaction volume without addressing underlying structural inefficiencies.
More prior authorization submissions. More billing activity. More back-and-forth between providers and payers. The technology works exactly as designed, and the result is more administrative spend, not less.
That is not an argument against automation. It is an argument for doing it correctly.
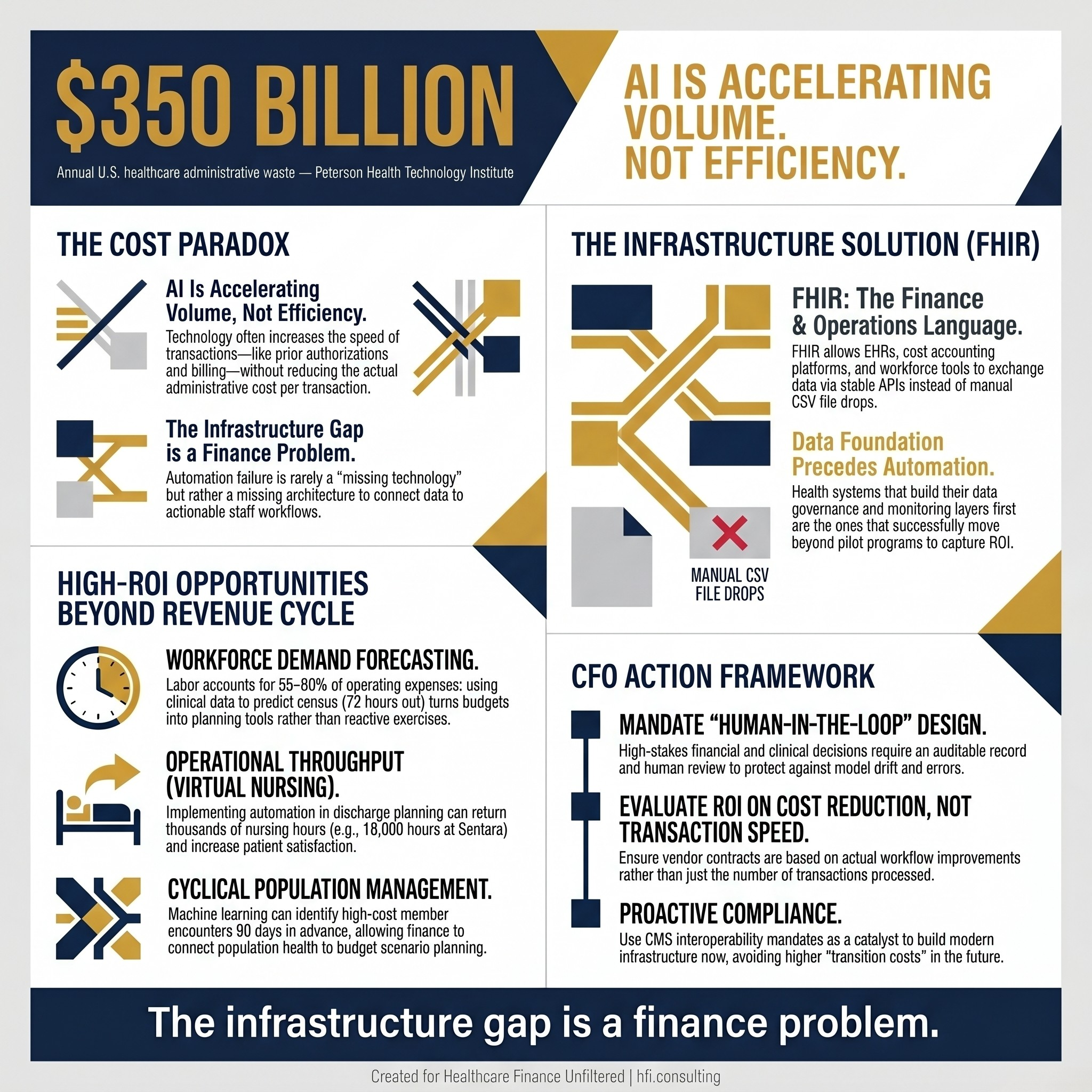
Stat card showing $350 billion annual healthcare administrative waste and the warning that AI is accelerating volume without improving efficiency.
The Problem Is Not the Tool. It Is the Operating Model Around It.
Healthcare organizations have concentrated most of their automation investment in revenue cycle: claims submission, denial management, prior authorization follow-up. That makes sense as a starting point. Billing is where money moves, and the ROI narrative is easier to construct.
But the $350 billion administrative waste problem identified by PHTI extends far beyond billing. Workforce scheduling inefficiencies, duplicative EHR data entry, population health outreach that runs on spreadsheets, and supply chain processes that still depend on fax and phone are all administrative waste. They simply do not show up in the same line item.
Finance leaders who have worked on both the payer and provider sides know that the dysfunction is symmetric. At Florida Blue Medicare, I managed programs where the gap between what population data said should happen and what actually triggered in operational workflows was significant. The problem was rarely a missing technology. It was a missing architecture for connecting what the technology knew to what staff could act on.
What FHIR Actually Unlocks for Finance Leaders
The shift toward FHIR-compliant systems is not a clinical informatics story. It is a finance and operations story, and most CFOs have not fully internalized that yet.
FHIR, the HL7-standard data language now baked into most modern EHR, payer, and health IT platforms, allows applications to exchange data the way modern software is supposed to exchange data: through stable APIs rather than CSV file drops or proprietary feeds. When your clinical documentation system, your cost accounting platform, and your workforce management tool all speak the same data language, the automation layer becomes dramatically more reliable.
The practical implication: the automation you have been trying to build on top of fragmented, manually reconciled data can finally work the way the vendor promised. That is not a technology upgrade. That is a finance and operational infrastructure decision.
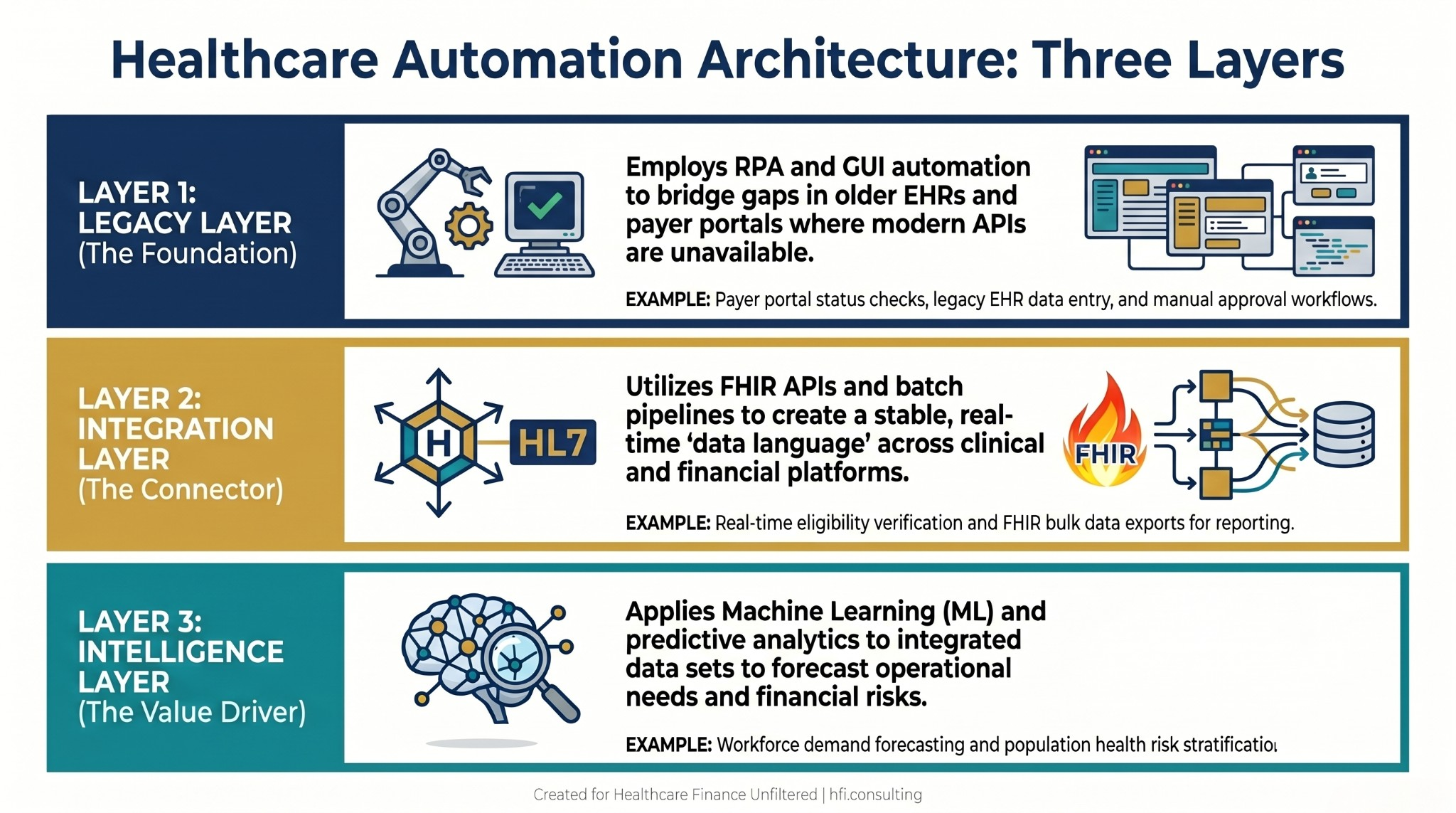
Three-layer healthcare automation architecture diagram showing RPA for legacy systems, FHIR API integration layer, and AI-powered intelligence layer with examples of each.
Three Automation Use Cases Finance Leaders Are Still Underusing
Revenue cycle is the obvious starting point, and if you have not addressed AI-driven denial prevention and documentation integrity, that work belongs on this year's roadmap. But the organizations producing the most measurable operational improvement are applying automation logic across three functions that finance typically influences but rarely owns technically.
Workforce Demand Forecasting
Labor is 55 to 60 percent of most health system operating expense. Most workforce management systems produce reports about what happened. Predictive analytics, when connected to FHIR-based clinical data feeds, can tell you what is likely to happen: inpatient census by unit for the next 72 hours, seasonal surge patterns for specific diagnoses, post-holiday ED volume spikes that have been predictable for five consecutive years but still get managed reactively.
At Ascension, managing financial operations across seven hospitals, the budget variance conversation was almost always a volume conversation. When volume forecasting uses real clinical pattern data instead of prior-year actuals plus an inflation adjustment, the budget becomes a planning tool rather than a compliance exercise.
Cyclical Condition Population Management
Payer organizations and health systems that take on value-based risk have a particular financial exposure here. Conditions like CHF, COPD, and diabetes follow seasonal patterns. They also follow social patterns. Members who lose insurance coverage in Q1 tend to show up at higher acuity in Q3.
Machine learning models trained on multi-year claims and clinical data can identify which members are most likely to generate high-cost encounters in the next 90 days. That is not a clinical decision. It is a financial planning input. The CFO who can connect population health predictions to budget scenario planning has a materially different conversation with the board than the one who is reacting to cost per member per month after the quarter closes.
Operational Throughput and Capacity Planning
OR scheduling, bed management, and discharge planning all have predictable patterns that existing staff still manage largely through experience and judgment. That judgment is valuable. The automation opportunity is not to replace it but to give it better inputs faster.
Sentara, for example, reported returning 18,000 nursing hours in year one of virtual nursing deployment, with 6.9 percent more pre-1pm discharges and patient satisfaction scores 2.9 percent higher for virtual discharge than in-person. Those are finance metrics. They show up in labor cost, length of stay, and bed utilization before they show up anywhere labeled "technology ROI."
Why the Infrastructure Has to Come First
Here is where most automation programs fail, and it is worth being direct about the mechanism.
Health systems that have successfully moved beyond pilot programs share a common characteristic: they built their data foundation before they bought the automation layer. Reliable data architecture, governance, monitoring, and workflow integration are not IT prerequisites. They are finance prerequisites.
A recent Healthcare IT News analysis co-authored by researchers from Jefferson Health put it plainly: the shortfall in healthcare AI adoption is not in the tools themselves. It is that most organizations lack the infrastructure those tools require to operate safely and at scale.
If your team cannot trust the data coming into a model, you cannot trust what the model tells you to do. If your governance structure takes six months to approve a low-risk automation application, you cannot move fast enough to capture the ROI that justified the investment. And if your monitoring process is retrospective rather than real-time, you will not catch the model drift until it has already affected your operations.
Finance leaders are positioned to sponsor this work in a way that IT alone is not. Capital allocation, vendor contract structure, and governance design are finance decisions. If you have covered the broader IT governance landscape, the framework we covered in IT Governance Is Now a Finance Problem for Health System CFOs applies directly here.
If you are evaluating automation vendors or planning a process automation initiative and want an independent framework for structuring the business case and governance model, that is work we do at hfi.consulting. The contact form takes about two minutes.
The Auditability Requirement Is Not Optional in Healthcare
Regulated environments require that any automation layer be fully auditable before it can be trusted with clinical or financial outcomes. This is not a compliance checkbox. It is the mechanism that protects your organization when a model makes a wrong recommendation.
Every automated action in a financial or clinical workflow needs a traceable record: what data triggered the decision, what rule or model was applied, what output was produced, and whether a human reviewed it before execution. Organizations building on modern platforms like Appian or UiPath are incorporating this audit architecture as a core requirement rather than an afterthought.
Human-in-the-loop design is the practical expression of that requirement. For high-stakes financial decisions, the automation performs the heavy lifting and pauses for a human to review and approve before the final write executes. That is not inefficiency. That is appropriate governance. The productivity gain is real even with that pause built in, because the human is reviewing a completed analysis rather than doing the analysis from scratch.
The cost case for payer organizations specifically: Global Excel Management, which processes claims across more than 90 countries, built automated data intake through FHIR-compatible portals and reported that faster claim adjudication translated directly to revenue. When you can address a member's concern faster, that is more revenue. The technology is paying for the project in many implementations.
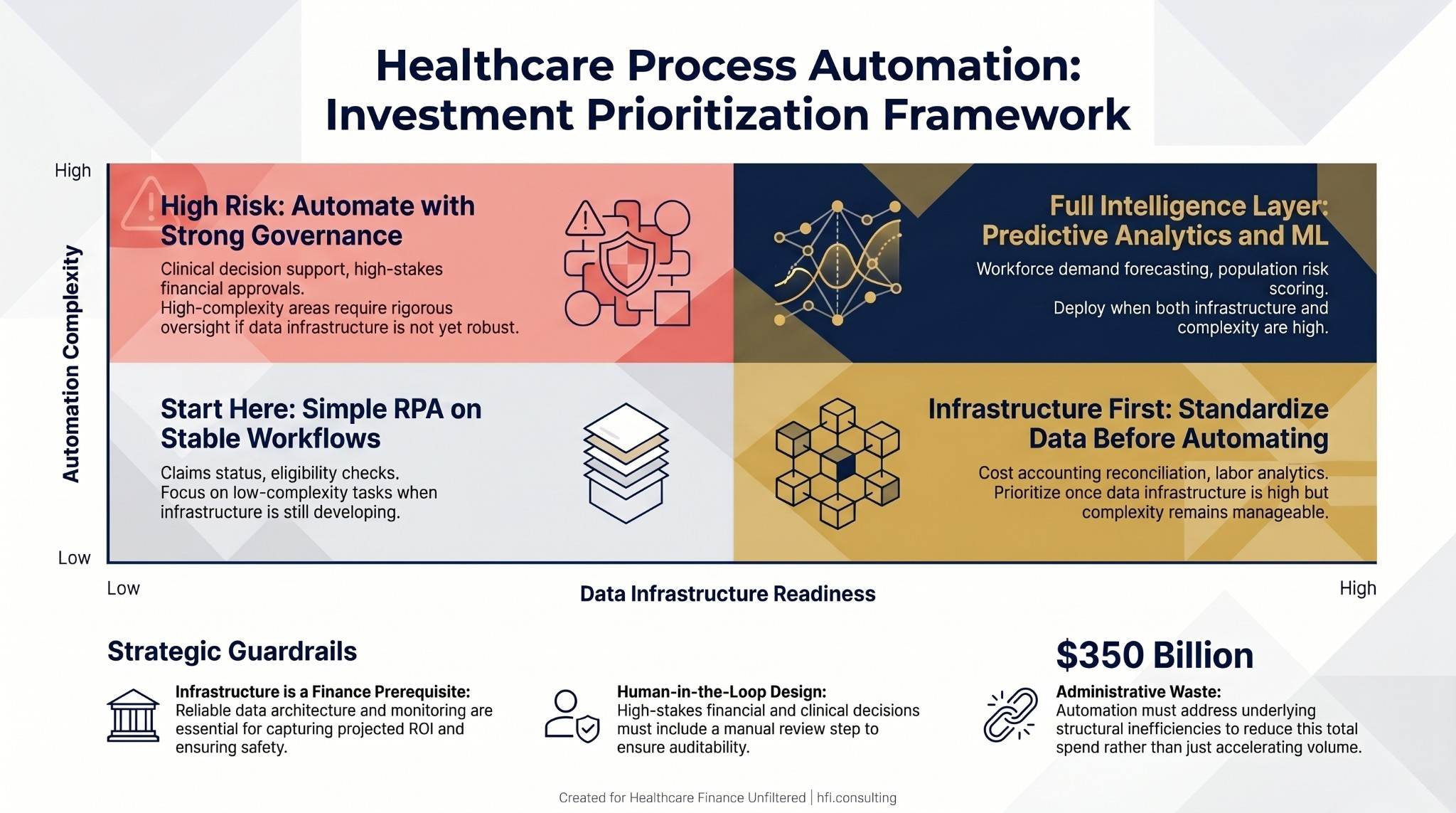
Decision matrix for healthcare automation investment prioritization based on data infrastructure readiness and workflow complexity, with four quadrant recommendations.
A CFO Action Framework for Process Automation
The finance leader's role in automation is not to manage the technical architecture. It is to ask the right questions of the right vendors and build the governance conditions that allow automation to work.
Before approving any new process automation investment, consider four questions:
Does this process require clinical judgment, or does it follow clear decision rules? Rule-based processes are safe automation candidates. Processes that require interpreting ambiguous clinical context need human-in-the-loop design from the start.
What happens when the source data changes upstream? Every automated pipeline has a failure mode. The question is whether you have monitoring in place to catch it before it affects your financials. We have covered what happens when it does not inThe AI Automation Trap.
Is your vendor's ROI case based on transaction speed or actual cost reduction? Transaction volume acceleration without workflow redesign is how AI increases administrative costs. The PHTI finding is a cautionary example of what happens when that distinction is not made in the contract and the governance model.
Does your governance structure have a clear path for approving and monitoring this specific tool? If the answer is "we will figure that out after implementation," the ROI timeline will slip. TheDigital Health Investment Justification framework we published earlier this year covers the hidden cost categories that most vendors leave out of the pro forma.
What This Signals for Budgeting and Strategic Planning
The healthcare organizations building automation infrastructure now are not doing it because the technology is finally ready. They are doing it because the regulatory environment is forcing administrative modernization whether they are ready or not.
CMS interoperability mandates, the claims attachments final rule, and prior authorization electronic requirements are all pulling administrative data onto modern infrastructure. Organizations that build proactively will pay less on every future mandate because the foundation is already in place. Those that wait will pay transition costs on top of compliance costs simultaneously.
For finance leaders who want to connect analytics capability to operational decision-making, the analytical infrastructure question has not changed. The tools available to answer it have. If your reporting stack is not telling you what is going to happen, only what already did, that gap has a financial cost that compounds every quarter it goes unaddressed.
The question is not whether to automate beyond revenue cycle. It is whether to build the infrastructure that makes that automation reliable before you buy the next layer of capability on top of an unstable foundation.
Ready to build the business case for a process automation initiative or governance framework at your organization? Connect at hfi.consulting. We work with health system and payer finance teams on the strategic and financial architecture before the vendor selection conversation starts.
P.S. How is your organization thinking about the balance between automated decision-making and human oversight right now? Are your governance structures keeping pace with what your vendors are actually deploying, or is that a gap you are actively working to close? Hit reply and let me know.