
Digital Health Investment Justification: The Hidden Cost Framework Every Healthcare CFO Needs
ROI is only one dimension. Here is the complete framework for evaluating digital health investments before committing capital.
Hospitals and health systems are not struggling to adopt digital health tools. They are struggling to make them work. That distinction matters enormously when you are sitting across from a vendor with a compelling demo and a multimillion-dollar price tag.
A new Qventus report on AI management by healthcare CIOs puts the challenge plainly: more than 70 percent of health system leaders now rate automated care operations platforms as critical to their 2026 objectives. But four in five of those same leaders cannot measure the ROI on what they have already deployed. If you cannot measure what you have, you are not in a position to justify what comes next.
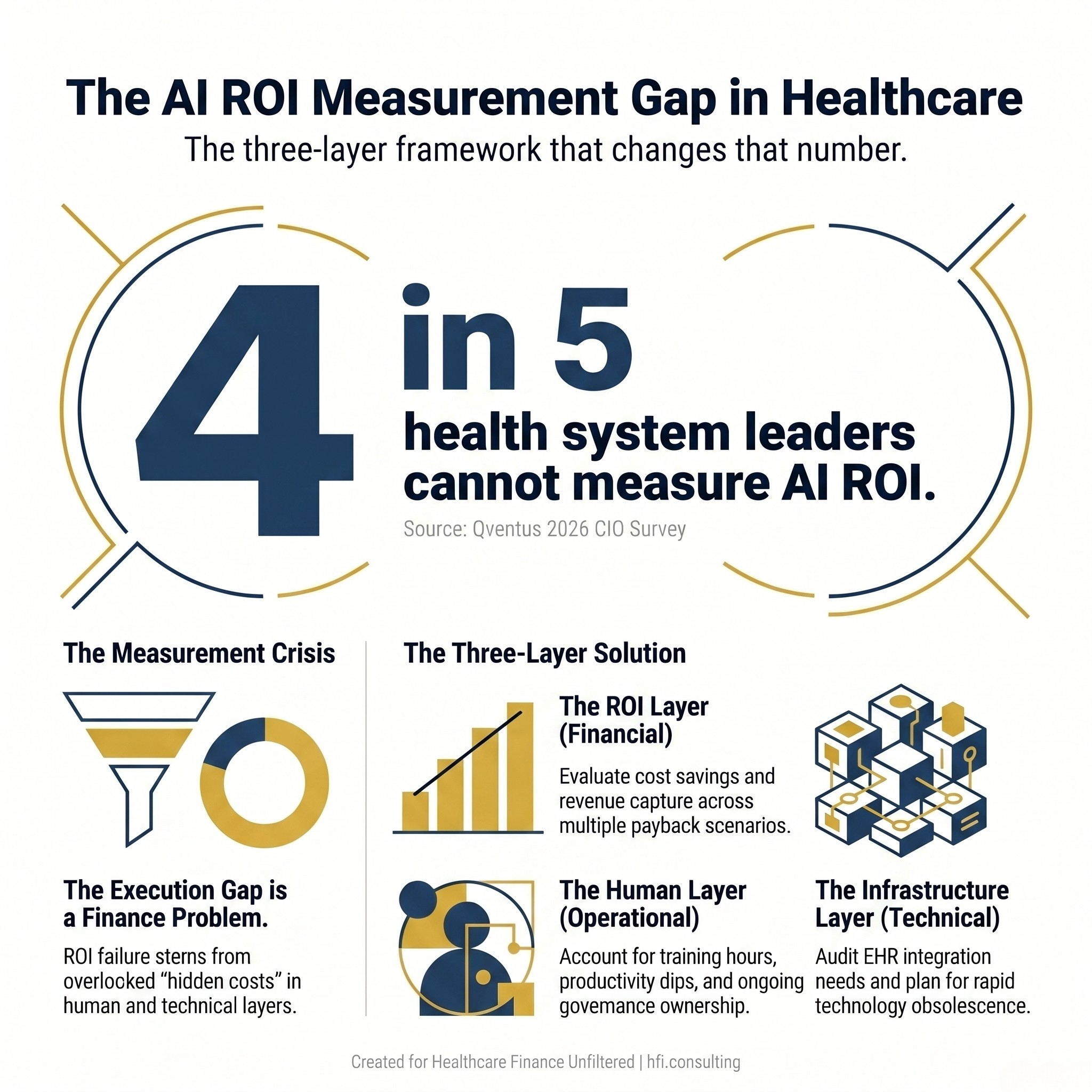
nfographic showing that 80 percent of health system leaders cannot measure ROI on their current AI investments, with a call to a three-layer evaluation framework.
The investment conversation in digital health has become dangerously compressed. Boards want a number. Finance wants a payback period. IT wants a platform decision. And everyone wants it resolved before the budget cycle closes. What gets lost in that compression is the full cost picture. ROI is one dimension. The hidden costs live in two others: the human layer and the hardware layer. Both will determine whether your investment performs or stalls.
Why the ROI Calculation Is Starting from the Wrong Place
The standard digital health business case leads with cost savings and revenue capture. Reduce denials by X percent. Automate prior auth at Y cost per transaction. Cut FTEs by Z. These projections are not wrong, but they are incomplete, and the incompleteness becomes visible only after implementation.
A Guidehouse and HFMA survey of nearly 200 provider executives found that 88 percent cite payer challenges as one of their top revenue cycle stressors. Claim denial rates continue to rise. Prior authorization delays compound the problem. And 20 percent of respondents now face a final denial rate above five percent, nearly double what was reported in the prior year's survey.
Here is the problem with layering AI onto that environment: the technology does not fix the underlying tension. The same survey found that 59 percent of provider executives have not implemented any AI or automation in their revenue cycle operations, even as 75 percent report deploying AI somewhere in the organization. The investment is happening. The revenue cycle is not benefiting. That gap has a cause.
The Human Layer: Where Digital Investments Go to Die
Workflow fit is not a soft concern. It is a financial variable. When AI tools arrive in a clinical or operational environment without adequate change management, staff work around them. Workarounds cost money. They also generate liability.
At Calderdale and Huddersfield NHS Foundation Trust, digital transformation took more than a decade and required structural alignment between clinical, operational, and corporate functions before any single tool could be called a success. Their chief digital and information officer was direct about the lesson: digital maturity cannot exist in isolated pockets of an organization. It must be embedded systemwide or it does not hold.
That is a harder sell in a U.S. health system running on 2-3 percent margins. But the alternative is worse. Implementing an AI-powered prior authorization tool on top of a broken payer-provider relationship does not recover revenue; it accelerates the dysfunction. The Peterson Health Technology Institute made this point explicitly in a recent analysis: when AI is applied to flawed administrative workflows, it does not solve the problems in those workflows. It makes them faster and more entrenched.
The human cost calculation needs to include:
Structured training hours per FTE across all affected departments
Productivity dip during the adoption curve (typically 60 to 120 days in revenue cycle implementations)
Change management resource allocation, including a dedicated internal project lead
Ongoing governance ownership once the vendor leaves the building
That last item is where most budgets are silent. Someone inside your organization needs to own the AI governance function. Without it, four in ten health systems cannot benchmark performance against the targets they set at contract signing.
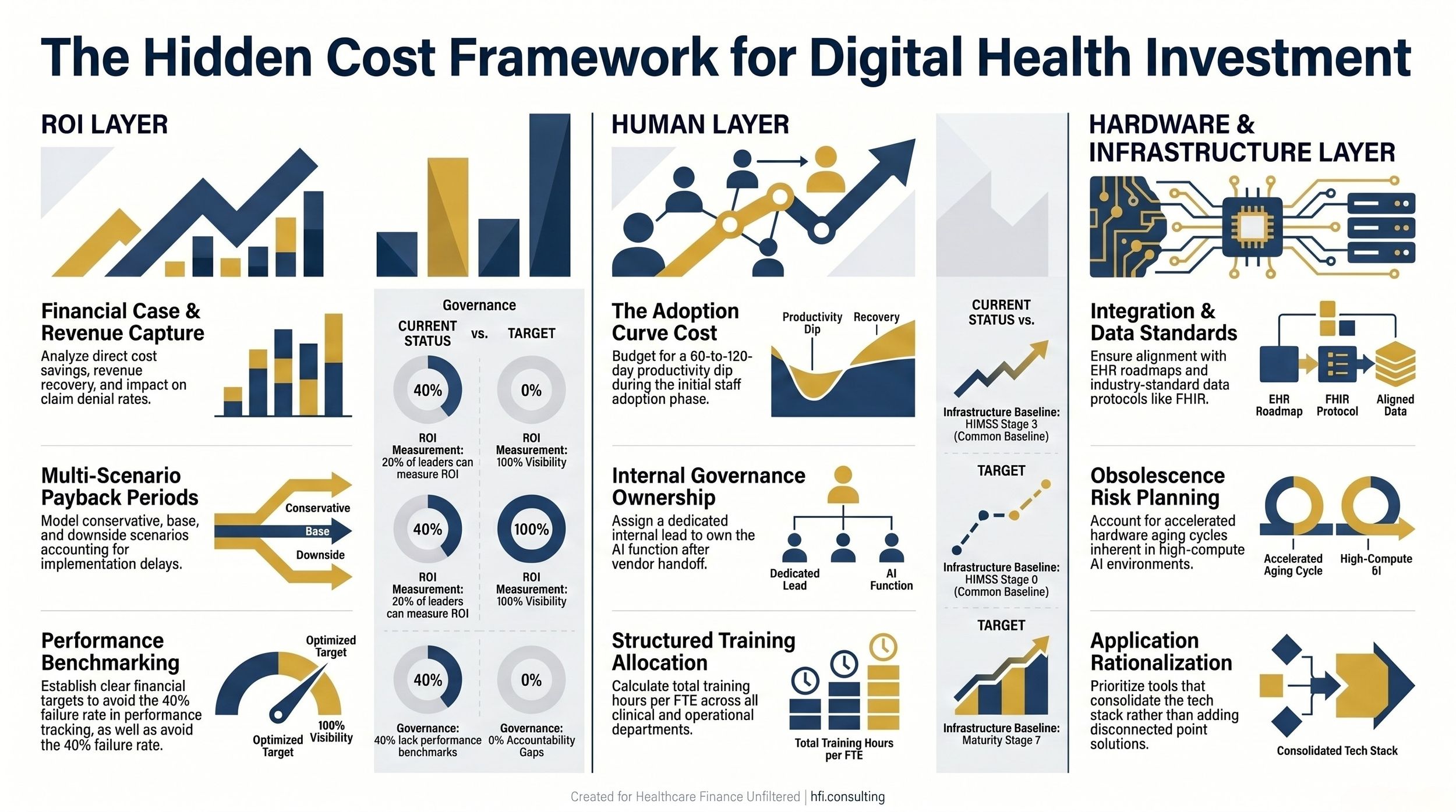
Framework diagram showing three dimensions of digital health investment justification: ROI layer, human layer, and hardware and infrastructure layer, each with key evaluation criteria.
The Hardware and Infrastructure Layer: Planning for Obsolescence Before Day One
Technology specifications age fast under normal conditions. In an AI environment, they age at an accelerated rate that most capital planning models do not account for.
This is the hardware problem in plain terms: the infrastructure required to run an AI application at contract signing may be insufficient to run the next generation of that same application eighteen months later. If your integration is built on a data standard that the vendor is migrating away from, you are looking at a remediation cost that was not in the original pro forma.
When I worked as a business advisor during Performance Analytics implementations at McKesson, the integration layer was always where the surprises lived. Not in the software itself. In the assumptions the implementation team made about what the existing infrastructure could support. Those assumptions were usually optimistic, and the gap between assumption and reality showed up as unbudgeted IT hours and delayed go-live timelines.
Healthcare CIOs are already grappling with this explicitly. Application rationalization is becoming a priority at major health systems, with leaders trying to reduce complexity, eliminate redundant tools, and control costs. The pressure is not to add more point solutions; it is to consolidate. But consolidation only works if the foundational infrastructure can support an integrated environment rather than a stack of disconnected applications.
The infrastructure due diligence checklist before signing:
What version of the EHR integration does this tool require, and what is the vendor's roadmap for subsequent EHR releases?
What data standards does the application use, and are those standards aligned with where the broader market is heading?
Who is responsible for maintaining the integration layer: your IT team, the vendor, or a third-party implementation partner?
What is the refresh cycle for the hardware components that support this application, and is that cycle built into the contract?
The Government of Jersey offers a useful model for this kind of rigor. Before committing to a 32 million pound digital investment, health leaders there conducted a HIMSS maturity assessment that placed their existing infrastructure at Stage 0 out of 7. They then built a risk projection that linked their current digital baseline to patient safety incidents and productivity loss. That projection turned a technical request into a funded program. The discipline was not in the ask; it was in the evidence that supported it.
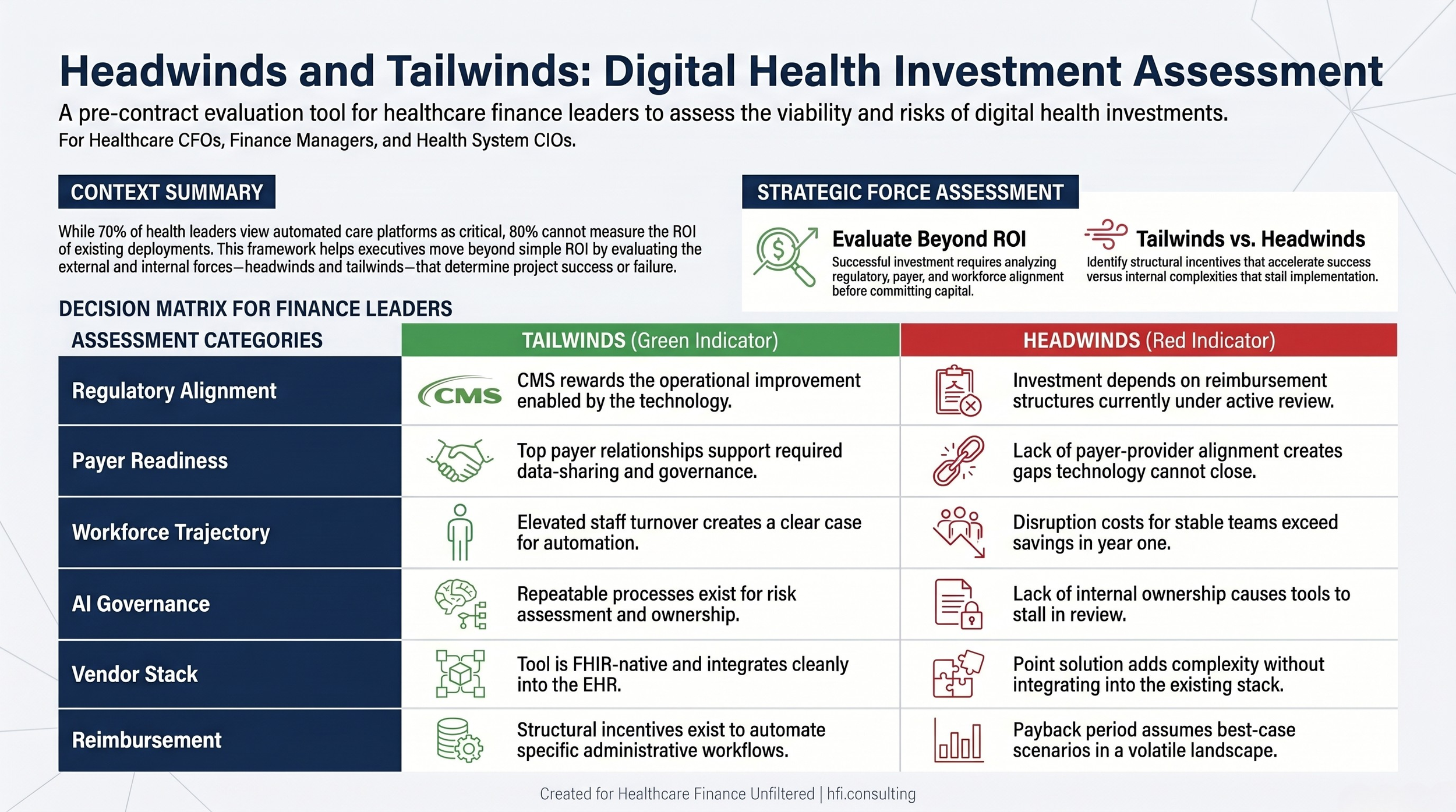
Decision matrix showing headwinds and tailwinds to evaluate before committing to a digital health investment, including regulatory alignment, payer readiness, and AI governance gaps.
Identifying Headwinds and Tailwinds Before the Contract Is Signed
Every digital health investment operates in an environment with forces working for it and against it. CFOs who identify those forces before the contract is signed are in a fundamentally different position than those who discover them post-implementation.
Tailwinds to evaluate:
Regulatory alignment is the most important tailwind to assess. If CMS is moving in a direction that rewards the operational improvement your technology enables, the investment thesis strengthens. Prior authorization reform, for example, is creating structural incentives to automate the approval workflow. A vendor who can demonstrate FHIR-native prior authorization functionality is positioned to capture that regulatory momentum.
Payer readiness is a second tailwind. The Guidehouse and HFMA report was direct: if providers and payers cannot align on governance, technology will not close the gap. Before investing in an AI-powered revenue cycle tool, it is worth understanding whether your top payer relationships can support the data-sharing requirements that tool depends on.
Workforce trajectory matters here too. If your revenue cycle department is experiencing elevated turnover, automation has a clearer ROI case. If your team is stable and experienced, the productivity cost of disruption may exceed the savings from automation in the first 18 months.
Headwinds to evaluate:
AI governance gaps are the most underestimated headwind in the current environment. Technology consultant David Chou, writing in Forbes, described the challenge clearly: health systems lack a repeatable process for approving use cases, assessing risk, assigning ownership, and setting data standards before moving to production. If your organization does not have that process in place, the AI investment will stall in governance review.
Point solution fatigue is a second headwind. Healthcare CIOs are consolidating, not expanding. If the tool you are evaluating adds to an already complex vendor environment without integrating cleanly into the existing stack, expect pushback from IT leadership that will slow the implementation timeline and add cost.
Regulatory volatility is a real constraint in the current environment. If the investment thesis depends on a specific reimbursement structure that is under active review by CMS, the payback period calculation needs a scenario that accounts for that structure changing.
This is where I think a lot of digital health business cases break down. They are built around a point-in-time regulatory environment. Healthcare finance leaders know better than anyone that the environment changes, and that the organization that survives is the one that planned for multiple scenarios, not the one that assumed the best case.
What a Complete Investment Justification Looks Like
The Guidehouse and HFMA report included a statement that healthcare leaders from provider organizations, payers, technology companies, and investment firms all agreed on: reimbursement policy reform is necessary to drive administrative efficiencies at scale. That is a long-horizon structural change. Your budget cycle is not waiting for it.
In the meantime, the investment justification framework that protects your organization covers all three dimensions:
ROI covers the financial case: cost savings, revenue capture, and payback period. It should include a conservative scenario, a base scenario, and a downside scenario that accounts for integration delays and adoption curve productivity loss.
The human layer covers the change management cost: training hours, internal governance ownership, and the productivity dip during implementation. It should include a defined accountability structure for who owns the tool after go-live.
The hardware and infrastructure layer covers the technical case: integration requirements, data standards alignment, vendor roadmap, and obsolescence risk. It should include a refresh assumption that is built into the capital plan, not left to a future budget negotiation.
If you can answer the key questions in each layer before signing, you are in a position to make a defensible investment decision. If you cannot, you are making a bet, and in a margin environment this thin, that is a bet you cannot afford to lose.
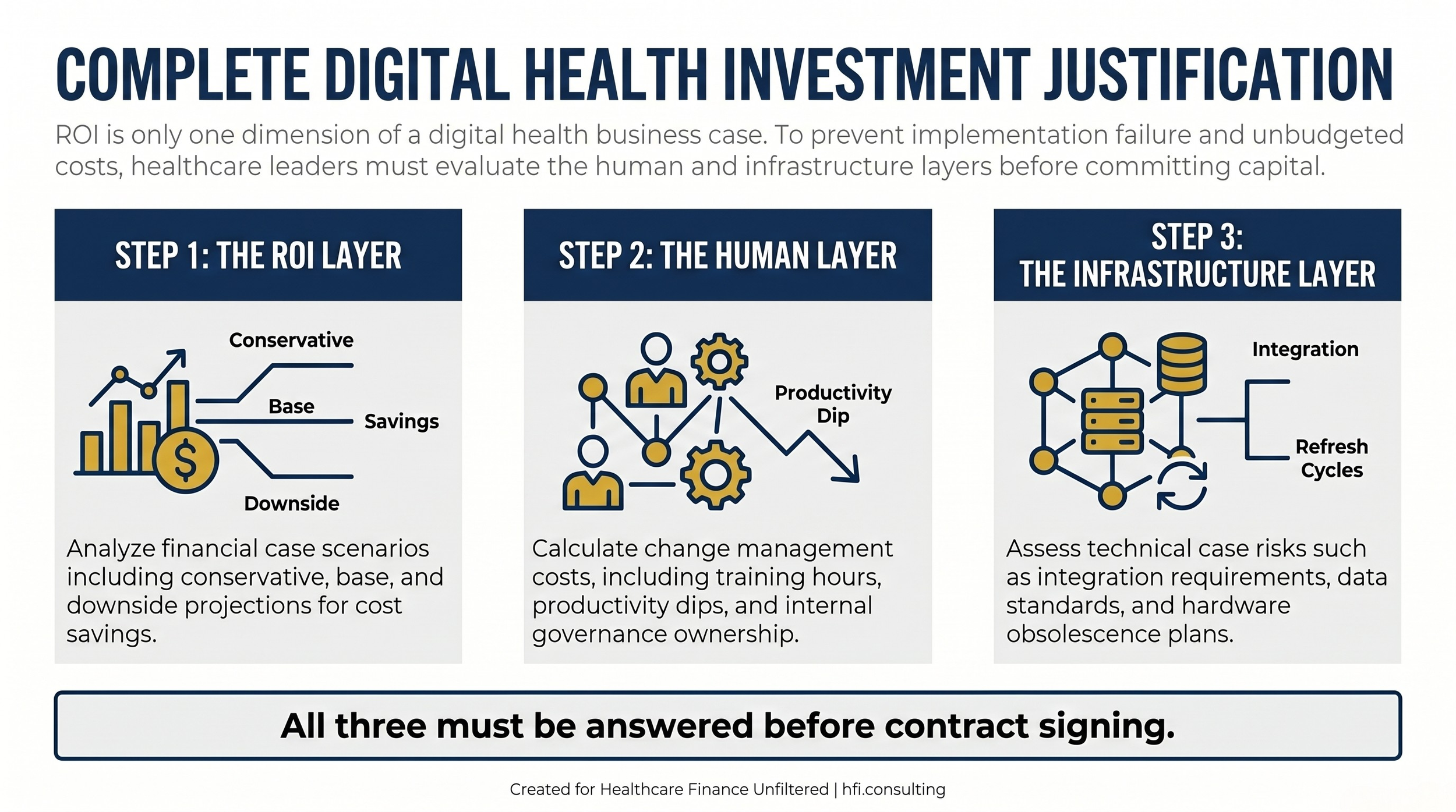
Process flow showing three required layers of a complete digital health investment justification: ROI layer, human layer, and infrastructure layer, with evaluation criteria for each.
If you are working through a digital health investment decision and want a structured framework for the full cost analysis, reply to this post and let me know. I am building out a companion evaluation tool that walks through all three dimensions in a format designed for CFO review.
The Execution Gap Is a Finance Problem
The industry has framed the AI implementation challenge as a technology problem. It is not. It is a governance problem, a workflow problem, and a capital planning problem. Those are all finance problems.
The health systems that will derive real value from digital health investments over the next three to five years are not the ones with the most aggressive AI adoption roadmaps. They are the ones who validated the full cost before they committed, aligned the organizational structure to support execution, and built accountability into the governance model from day one.
That kind of discipline is exactly what healthcare finance leaders are positioned to provide. The question is whether finance is at the table when the investment decision is being made, or whether it arrives after the fact to build a business case for something that has already been chosen.
Get into that conversation earlier. The tools are moving fast. The fundamentals of good investment analysis are not.
If you found this framework useful, forward it to a finance colleague who is in the middle of a digital health evaluation. And subscribe to Healthcare Finance Unfiltered for operational analysis delivered without the vendor spin.
P.S. Where is your organization in the digital health investment cycle right now: still building the business case, mid-implementation, or trying to measure ROI on something already deployed? Hit reply and tell me what stage is creating the most friction for your finance team.