
Healthcare Price Transparency for Hospital CFOs: From Compliance Liability to Contract Strategy
CMS enforcement is tightening, your competitors are mining your MRF data, and the Patients Deserve Price Tags Act is coming. Here is your playbook.
The No Surprises Act started it. CMS standardization enforcement accelerated it. The Patients Deserve Price Tags Act, which carries proposed penalties up to $10 million for willful violations, is positioned to complete the transformation.
Three data points on healthcare price transparency enforcement escalation for hospital CFOs, including the $10M penalty proposed under the Patients Deserve Price Tags Act.
What the most sophisticated health systems and the most aggressive self-insured employers in your market have already figured out is that price transparency is no longer a compliance problem. It is a competitive intelligence tool. The question for every provider CFO right now is whether your organization is on the using end of that intelligence or the receiving end.
This is a structural shift in how commercial rates get negotiated, how outpatient volume gets retained, and how revenue cycle operations get funded. Here is the CFO framework for getting ahead of it.
What Changed: From Reluctant Compliance to Standardized Enforcement
For the first few years after hospital transparency mandates took effect in 2021, the dominant strategy was minimal compliance. Health systems published machine-readable files that technically satisfied the rule but were organized in formats so fragmented and inconsistent that automated parsing tools struggled to use them.
CMS ended that era. The standardized data dictionary requirement now forces hospitals to publish MRFs using a CMS-specified template hosted on GitHub. Terms like gross charge, discounted cash price, and payer-specific negotiated charge must be formatted identically nationwide. There is no longer a structural advantage to publishing data in formats that defeat the purpose of the rule.
The Patients Deserve Price Tags Act, which has bipartisan support in both chambers, would tighten the requirements further. Under the pending legislation, hospitals could no longer satisfy transparency requirements by posting price estimator tools. Exact dollar amounts for cash prices and insurance-negotiated rates would be required before service, with itemized billing or flat-rate bundled pricing options provided to patients upfront. Willful violations could reach $10 million.
For provider CFOs, the compliance calculus has changed. The penalty exposure is real, but the larger operational risk is what happens when your pricing data becomes fully machine-readable by every employer, data aggregator, and competing health system in your market.
Your Competitors Are Already Mining Your Rates
The practical impact of standardized MRFs is already visible in commercial negotiations. Technology companies have built business models entirely around ingesting hospital MRF data, cleaning it, and reselling it as competitive market intelligence. Your competitors do not need a consultant engagement or a FOIA request to access your negotiated rates. They need an internet connection and the right parsing platform.
That means the health system across town can know exactly what United, Aetna, and BCBS are paying you for a level-4 emergency department visit, an orthopedic bundle, or a C-section. They can know it by payer, by procedure, and by service line. If they are paying attention, they know it before you walk into your next contract renewal meeting.
The asymmetry that historically protected dominant systems has narrowed significantly. A regional competitor or independent ASC that could not obtain your negotiated rate data three years ago now has access to a machine-readable file that tells them precisely where you are priced and where the spread is largest between your rates and theirs.
For health systems managing rate structures built on historical market dominance, this is not a future concern. It is a current operational reality.
Flipping the Script: Using Transparency Data in Your Next Negotiation
The same data environment that exposes your rates to competitors also gives you access to theirs. This is the most underutilized strategic opportunity for provider CFOs right now.
If a competitor system in your market is receiving reimbursement 25 to 30 percent above your rates for the same procedure from the same payer, that gap is now documentable. You walk into the negotiation with verified, third-party machine-readable data rather than anecdotal benchmarks or consultant survey estimates. That is a fundamentally different negotiating position than the one most health systems occupied before MRF standardization.
The flip side is equally critical to understand. Payers are using this same data to target what they internally call positive outliers. If your system has historically enjoyed premium rates due to market dominance or a long-standing payer relationship, that payer's finance team has already run the benchmarking analysis. They know precisely where your rates sit relative to the market median, and they will bring that data to your next renewal.
Your defense is not to pretend the data does not exist. Your defense is to document, in advance of every negotiation cycle, the quality metrics, acuity mix, clinical outcome data, and patient complexity indicators that justify your rate premium. The CFO who walks into a payer negotiation armed only with historical yield data is going to lose ground to a payer analyst who arrives with a market MRF rate spreadsheet and a median benchmark line.
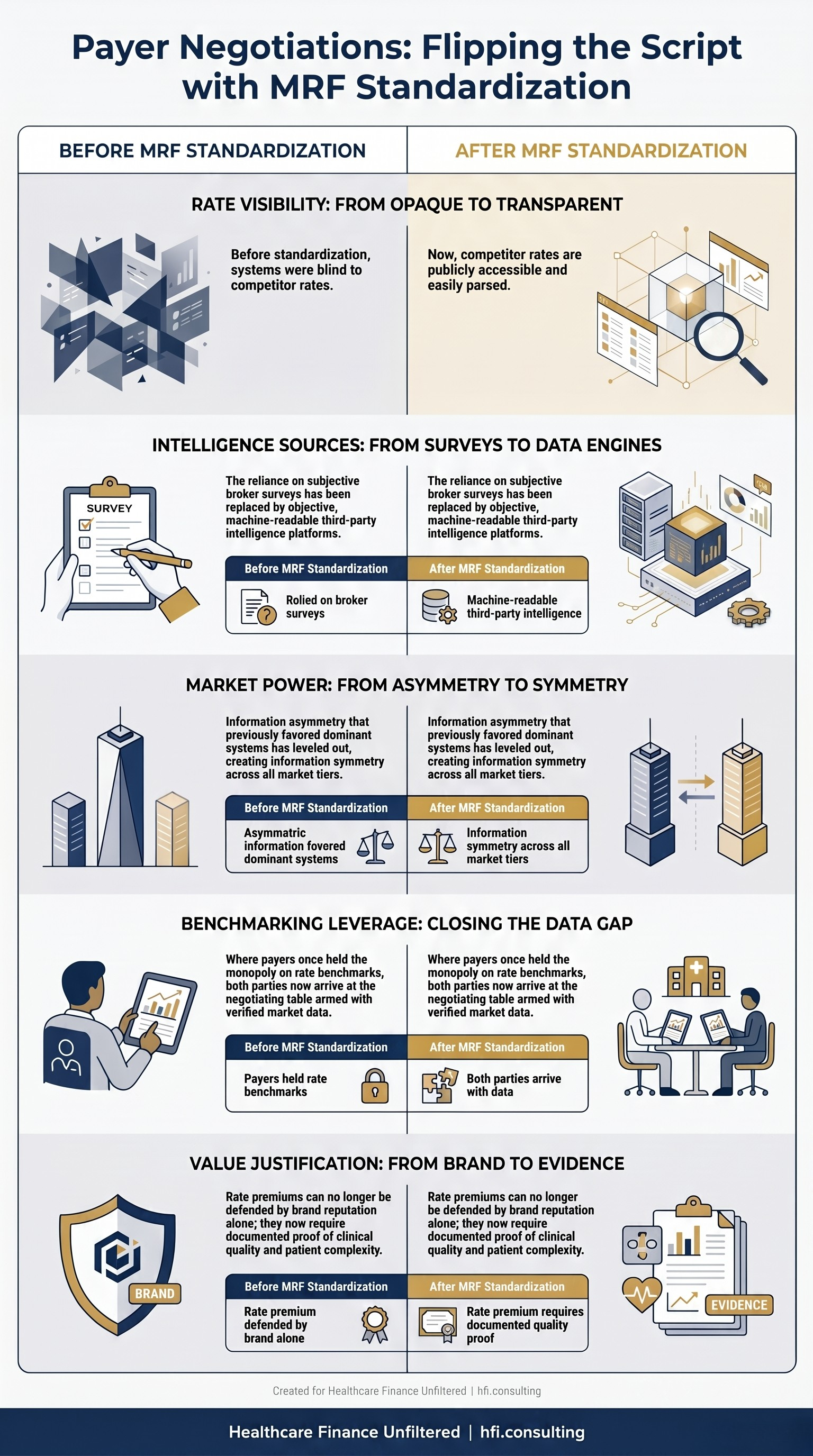
Comparison table showing how MRF standardization changed payer contract negotiation dynamics for hospital CFOs, from blind rate guessing to symmetrical market intelligence.
Revenue Cycle Integration: Moving Transparency to the Front End
For most health systems, price transparency has lived in the IT department or the compliance function. The finance leaders extracting measurable margin value from it have moved it into revenue cycle operations.
The core architecture is this: pull your standardized MRF data and real-time eligibility APIs into your pre-service workflow. Build or license a consumer estimator tool that generates a contract-verified out-of-pocket cost estimate before the patient arrives. The estimate does not need to be exact to the dollar. It needs to be defensible, directionally accurate, and delivered in a format the patient can act on.
Health systems that have implemented this architecture consistently report measurable reductions in downstream billing disputes, administrative write-offs, and time-to-collection. Patients who receive an accurate upfront estimate are significantly more likely to authorize a payment arrangement, complete a digital payment at point of care, or accept structured financing before discharge. That revenue lands in a fundamentally different place in your cash flow timeline than a bill that cycles through a 60-day collections workflow.
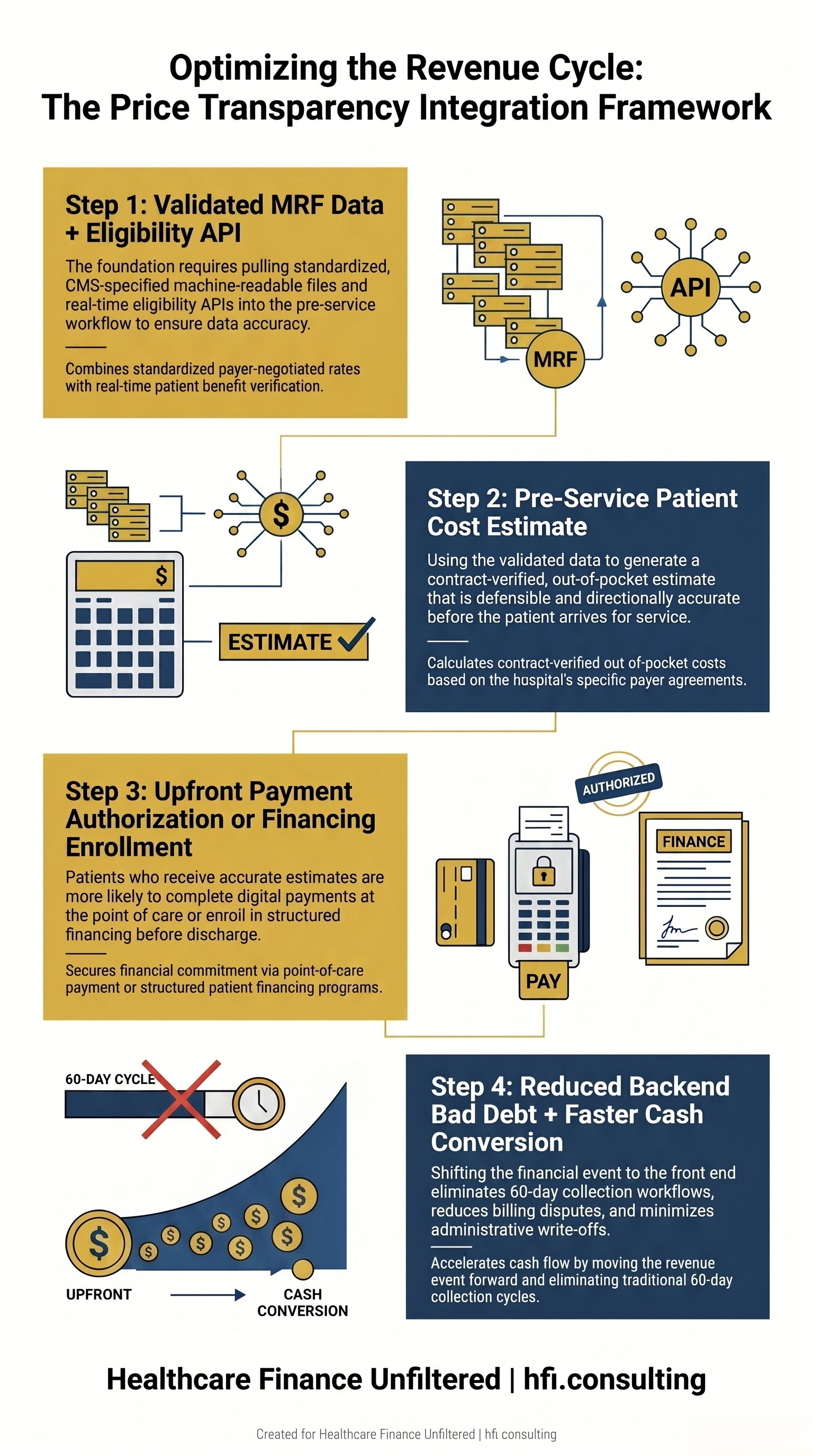
Four-step process flow showing how hospital CFOs can integrate MRF data into front-end revenue cycle operations to reduce bad debt and accelerate cash collection.
The cost accounting precision required for this model is non-trivial. In working with health systems on service line contribution margin analysis, the organizations that generate accurate front-end estimates almost always share a common characteristic: they have already done the upstream work of reconciling their chargemaster to actual payer contract terms. The systems that cannot produce a reliable pre-service estimate tend to also be the ones with the most significant margin leakage in their surgical service lines. These problems typically share the same root cause. For a deeper look at how that service line analysis works, see Service Line Financial Assessment: A CFO Framework.
The ASC Threat: Defending Outpatient Volume With Transparent Pricing
Ambulatory surgery centers and freestanding imaging centers have always competed on price. What changed is that they now compete with your verified published data.
An independent ASC operator can pull your hospital's MRF, identify the procedures where facility fees create the largest price differential between their rates and yours, and build a direct-to-employer pitch around that exact procedure list. They do not need to estimate your pricing. They can reference it directly.
For procedures in the shoppable services category, including MRIs, colonoscopies, arthroscopies, and elective orthopedic surgeries, hospital outpatient departments are increasingly vulnerable. The facility fee premium that historically justified the higher cost is now visible to every employer with a benefits consultant and access to a data aggregator.
The CFO response is not to abandon facility fees across the board. It is to be deliberate about which service lines can sustain the premium and which ones are actively leaking profitable commercial volume to competitors. For the service lines where the price differential has become indefensible, restructuring pricing to protect volume is a better outcome than watching the case mix shift to a setting where your system collects nothing.
Some health systems are going further. By building transparent all-inclusive bundled pricing packages marketed directly to local self-insured employers, they bypass the traditional payer network and compete directly on price, quality documentation, and volume commitment. The employer receives a predictable per-episode cost. The health system receives committed procedure volume and a direct commercial relationship. It is the same direct-contracting model that freestanding ASCs have used successfully for years, applied at the health system level.
This is a good moment to connect with what you are working on.
If your organization is evaluating how MRF data is affecting your payer contract positioning, your outpatient volume retention strategy, or your direct-to-employer contracting opportunities, the contribution margin and competitive benchmarking analysis that supports those decisions is what HFI Consulting does. You can reach out directly through hfi.consulting or reply to this email.
Building Cross-Departmental Governance for Pricing Data
The compliance dimension of MRF management has escalated beyond what most health systems anticipated when they built their initial publishing workflows. CMS is now levying direct public financial penalties rather than issuing warning letters. Maintaining static or fragmented pricing files is an active operational liability.
Because standardized pricing data touches compliance, IT, legal, revenue cycle, and managed care contracting simultaneously, health system CFOs are establishing formal governance structures rather than leaving MRF ownership to a single department.
The governance model that holds up in practice requires several components. A designated data steward who is accountable for MRF accuracy and update timeliness. A reconciliation cycle that validates published files against current payer contract terms on a regular cadence. A cross-functional review process that catches contract modifications before they create a compliance gap between what is published and what the current allowable rates actually are.
That reconciliation is not a once-a-year audit. Payer contracts are amended throughout the year, and any modification to allowable amounts that does not trigger a corresponding MRF update creates regulatory exposure. For systems managing dozens of payer contracts across multiple facilities, the operational burden of keeping the published files current is significant and should be resourced accordingly.
The CFO's role in this governance structure is to ensure that pricing data management carries the same organizational priority and the same audit discipline as financial reporting controls. Both carry regulatory consequence. Both require a repeatable, documented process. And in both cases, the position that your organization did not know the published data was inaccurate is not a viable defense with the regulator.
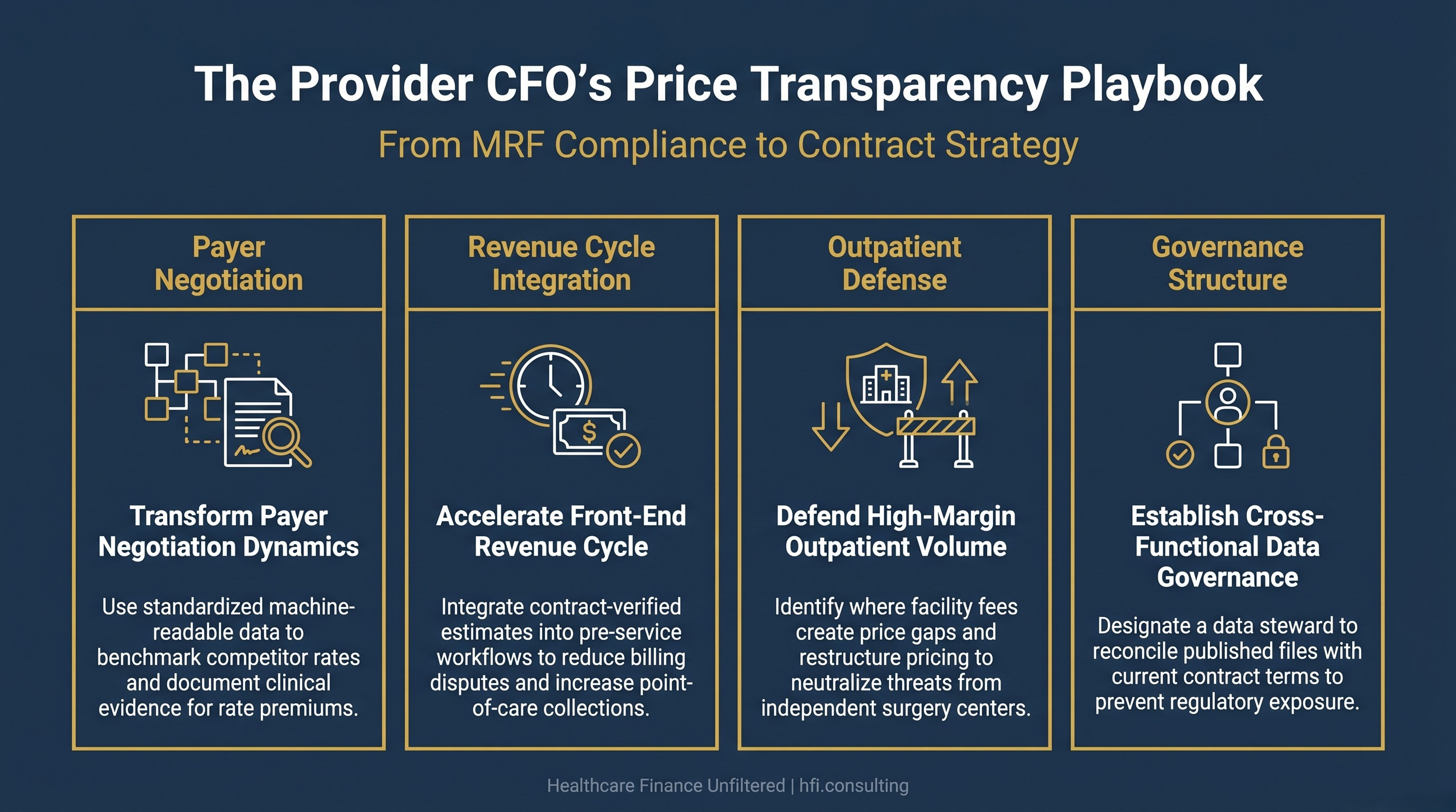
Healthcare Finance Unfiltered featured image for hospital CFO price transparency article covering payer negotiation, revenue cycle integration, outpatient defense strategy, and compliance governance.
What the Next Phase Looks Like
The federal transparency agenda is accelerating. A May 2026 Senate HELP Committee field hearing on healthcare affordability highlighted that AI tools capable of parsing public explanation-of-benefit data and pricing individual procedures at the provider level are already operational in the market. Pending legislation would add a claims-data transparency layer on top of existing MRF mandates, giving self-insured employers audit access to pharmacy and medical claims at a level of detail that is not currently available.
For provider CFOs, the direction of travel is clear. The data environment governing commercial pricing is going to become more structured, more machine-readable, and more actionable for the institutional buyers who fund the largest share of your commercial volume. Health systems that build internal infrastructure to use that data as a strategic asset will be better positioned in every contract cycle going forward.
The CFOs who continue to treat transparency as a compliance function will manage it reactively, defending against penalty exposure while watching competitor and employer strategies evolve around them. The CFOs who treat it as a contract strategy tool will use it to protect outpatient volume, improve front-end collections, and document rate premiums with verified clinical and financial evidence.
The data is already public. The question is who is using it better.
For more on the operational frameworks that connect price transparency to service line margin management, see AI-Powered Revenue Leakage Prevention: The CFO Implementation Guide and How Much Revenue Is Your Hospital Losing to Implant Billing Gaps?.
Healthcare Finance Unfiltered covers the operational and financial dynamics that affect health system CFOs every week. If this analysis was useful, subscribe at hfi.consulting or forward it to a colleague in managed care contracting or revenue cycle leadership.
Part 2 of this series covers the payer and insurance CFO perspective on price transparency, including the TiC compliance burden, PBM reform under CAA 2026, and the strategic pivot from proprietary network discounts to value-based plan design. It publishes tomorrow.
P.S. For the provider CFOs reading this: how is your organization currently using competitor MRF data in payer contract preparation? Are you pulling it directly, working through a data platform, or not yet incorporating it into the negotiation cycle? Hit reply and tell me where your team is on this.