
Women Healthcare CFOs: The Career Moves Finance Leaders Need to Make on the Path to the C-Suite
Structural barriers keeping women out of healthcare CFO seats, and the career moves that close the gap before 2030.
Women make up roughly 70% of the healthcare workforce. They run the nursing floors, manage the clinical teams, handle payer relationships, and sit in a majority of the finance department cubicles that keep a hospital solvent.
Yet across the 667 largest healthcare companies recently studied, women hold only about 11 CFO seats. Healthcare has the fewest women CFOs of any major sector, and that is the paradox every woman in healthcare finance already feels in her bones, even if she has never seen the numbers.
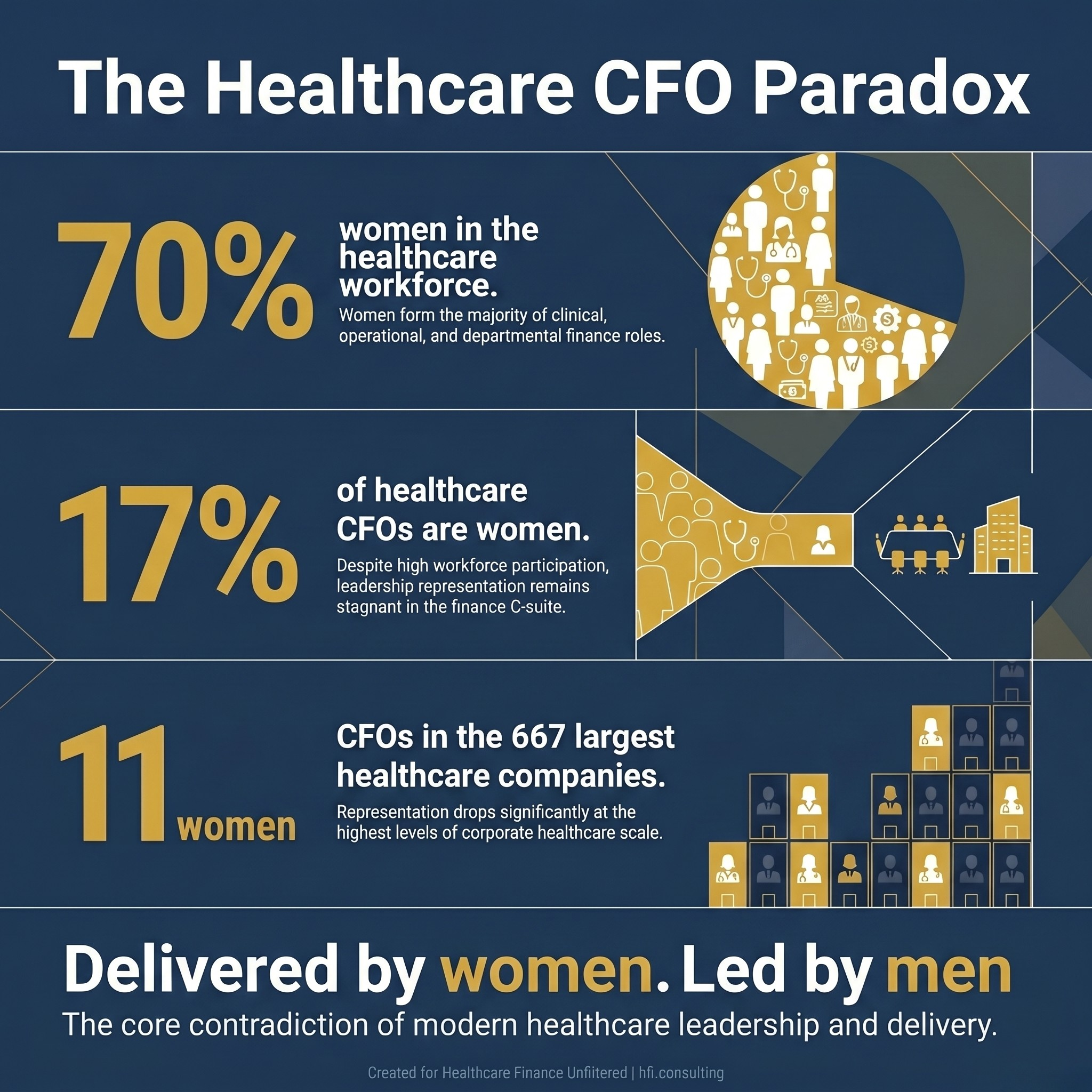
Infographic showing three statistics illustrating the gender gap in healthcare CFO roles: 70% of healthcare workers are women, only 17% of healthcare CFOs are women, and just 11 women hold CFO seats at the 667 largest healthcare companies.
The Paradox: Delivered by Women, Led by Men
At the broader Fortune 500 level, progress is real but slow. Women now hold 17.4% of Fortune 500 CFO roles, up from 12% in 2015, according to a recent analysis from HighRadius. That works out to about half a percentage point of gain per year over the last decade.
Healthcare tracks roughly in line with that number. At the Becker's 16th Annual Meeting, Shelly Schorer, South Region CFO at CommonSpirit Health, noted that healthcare CFOs were 2% female when she started her career, and are now around 17%. Progress, yes. Parity, no.
The deeper problem is that the pipeline narrows fastest in the exact places where the CFO skill set gets built. This is not a story about talent supply. Women earn 60% of accounting degrees and 52% of finance MBAs. It is a story about where the pipeline leaks, and four structural leaks do most of the damage.
Barrier 1: The Broken Rung at Mid-Management
The CFO gap does not start at the top. It starts at the first step up to management.
In healthcare, for every 100 men promoted to their first managerial role, only 93 women are promoted. That gap compounds for 15 to 20 years before anyone conducts a CFO search, and by the time the search happens, the pool of qualified women is already thin.
This matters because most CFO recruiters filter for candidates with at least 15 years of progressive leadership experience. If a woman loses ground at the first promotion, she spends the rest of her career running to catch up to peers who started the climb at the same time.
The move: If you are in a director or senior manager role and you have been there for more than three years without a clear path to the next level, that is your signal to either advocate for a promotion with specific revenue or P&L responsibility attached, or begin quietly looking externally. The first step up is the one that sets your trajectory.
Barrier 2: Line Roles vs. Staff Roles
This is the most important barrier in healthcare finance, and the one that is almost never discussed openly in performance reviews.
CFO candidates are recruited almost exclusively from line roles, meaning positions with direct P&L responsibility, revenue-generating authority, or operational budget accountability. Women in healthcare are disproportionately concentrated in staff roles such as HR, legal, marketing, compliance, and clinical operations. Men are more often routed into line roles such as operations, business development, service line finance, and capital planning.
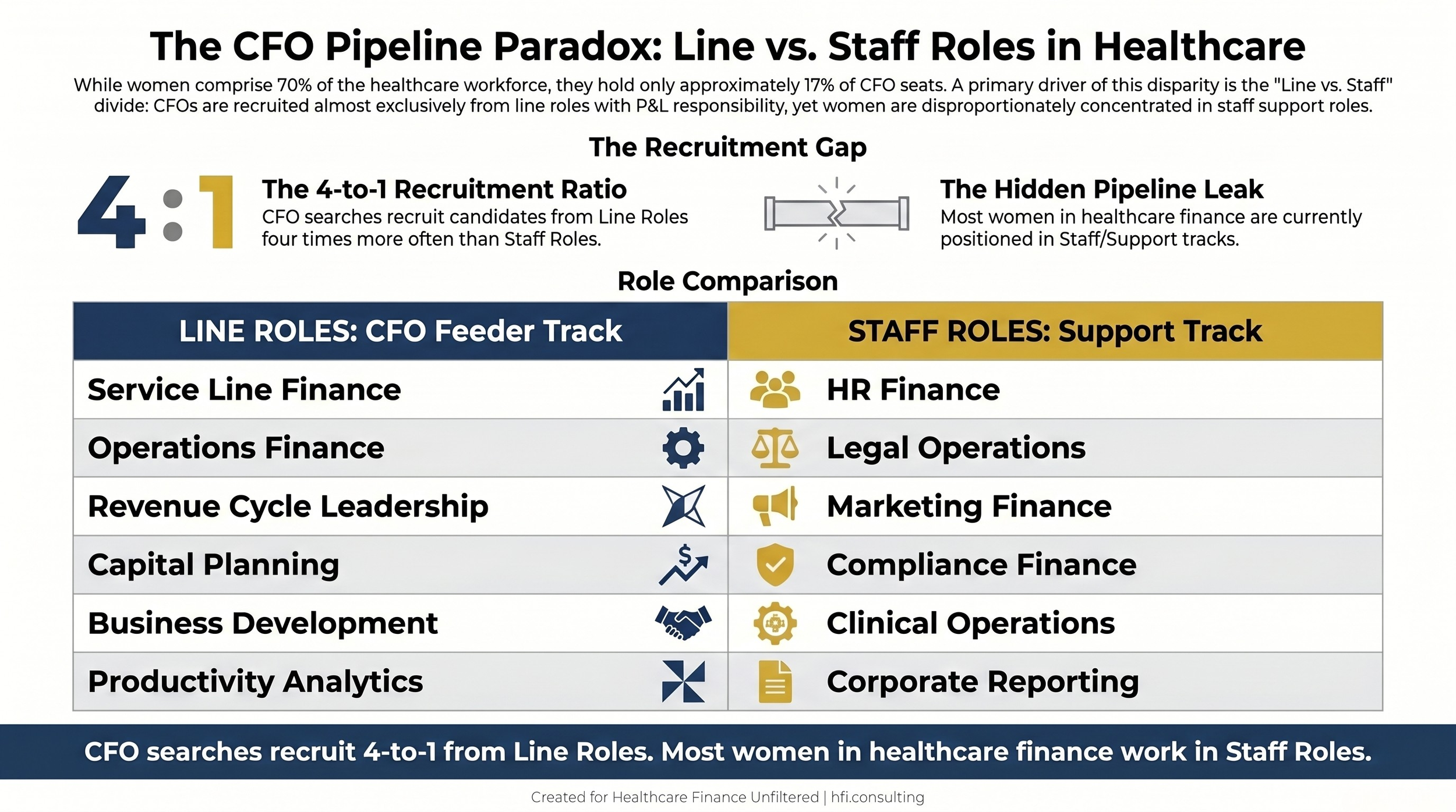
Comparison table showing line roles that feed into healthcare CFO positions, including service line finance, operations, revenue cycle, and capital planning, versus staff roles including HR finance, legal, and compliance, with a note that CFO searches recruit four times more frequently from line roles.
The distinction is often invisible inside an organization until a CFO search begins. A woman who has spent eight years building deep technical expertise in cost accounting or FP&A support is doing essential work. She is also, from a succession planning perspective, in the wrong seat. The skills transfer, but the resume does not tell the story a search committee is looking for.
Capital allocation, service line margin, and P&L accountability are the three areas every CFO interview panel will test. If your resume is heavy on reporting and light on decisions that moved revenue or cost, the panel will draw its own conclusion.
The move: If you are in a staff role, request a rotation into operations, service line finance, or revenue cycle leadership. If your organization does not offer formal rotations, volunteer for the capital project team, the margin improvement task force, or the new service line business case. You need your fingerprints on decisions that changed a P&L line.
Barrier 3: Mentors Are Plentiful, Sponsors Are Rare
Research consistently shows that women in healthcare finance have plenty of mentors. What they lack are sponsors.
The distinction matters. A mentor gives you advice. A sponsor spends political capital on your behalf when you are not in the room. In healthcare finance, 31% of women report having a senior sponsor, compared to 45% of men. That 14-point gap is roughly the difference between being considered for a stretch assignment and being handed one.
Sponsors get you into the meetings where large capital requests are debated. They put your name forward for board presentations. They call the search firm when a CFO role opens in a neighboring market. Mentors, by contrast, mostly tell you to believe in yourself and to read one more book on executive presence.
Sponsorship in healthcare finance is also unusually concentrated. A handful of senior finance leaders influence dozens of promotion decisions across regional networks, system offices, and board search committees. Reach one of them with a useful track record and your name travels further than any internal performance review will.
The move: Identify one senior executive who has actually recommended someone for a promotion in the last twelve months. That is your sponsor candidate. Build a relationship around giving them useful work product, not around coffee chats. Sponsorship follows utility, not rapport.
Barrier 4: The Flexibility Tax and Visibility Bias
Return-to-office mandates in 2025 and 2026 reintroduced a variable that had almost disappeared during the remote-work era. Call it visibility bias, or the informal flexibility tax.
Women, who are statistically more likely to use flexible or remote arrangements to manage caregiving responsibilities, are now 16% less likely to be promoted than peers who work primarily on-site, even when performance metrics are identical. That number comes from multiple recent corporate surveys, and it is not specific to healthcare. But healthcare is a physical-plant industry where executive presence has always mattered more than the data suggests it should.
This is one of the harder barriers to name out loud, because it feels uncomfortable to say that being in the building changes how you are evaluated. The evidence, however, is clear.
The move: If flexibility matters to you, choose your battles. Be on-site for the meetings that generate sponsorship, even if you work the other three days remotely. Capital planning sessions, board prep, CEO staff meetings, and service line strategy reviews are the rooms where promotion decisions are incubated months before they happen. The rest can be done from anywhere.
Barrier 5: The Mobility Question
The four structural barriers above have been widely studied. The fifth, which gets less attention in the research literature, is mobility.
Healthcare leadership is an unusually mobile profession. The CommonSpirit, Mayo, and CommonSpirit regional appointments announced in the first quarter of 2026 span moves from Ohio to Chicago, from California to the South region covering five states, and from Milwaukee to Wisconsin. Many of the women now in visible CFO roles earned their last promotion by moving to take it. Amy Crouch and Katina Williams, both profiled recently by HealthLeaders, followed the same pattern.
Mobility is not neutral with respect to family structure. Women in healthcare finance more frequently have spouses whose careers cannot relocate on twelve months’ notice. They more often have elderly parents whose care depends on proximity. They more often have school-aged children in specialized programs or special education plans that cannot be recreated in a new market.
This is not a character flaw and it is not a lack of ambition. It is geometry. The denominator of available opportunities shrinks when you cannot move.
The move: If you are place-bound, you need to double the quality of your network inside your metro area and triple the quality of your external visibility. Conference speaking, industry association leadership, and published writing create what a physical move used to create, which is a wider pool of executives who already know your work when a local seat opens up.
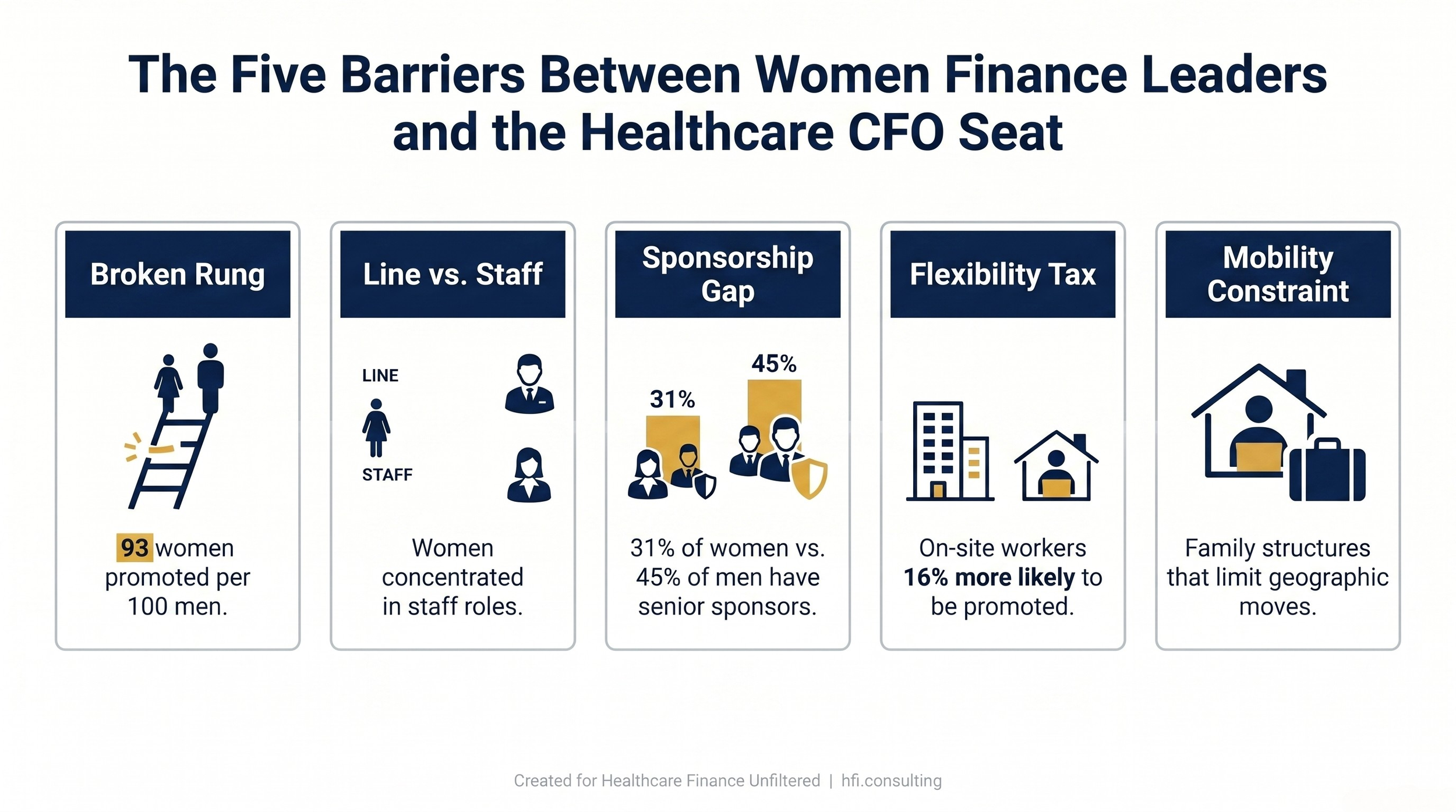
Horizontal framework diagram showing five barriers to women reaching healthcare CFO roles: the broken rung at mid-management, line versus staff role concentration, the sponsorship gap, the flexibility tax, and mobility constraints.
What This Means for Healthcare Finance Leaders Right Now
The structural barriers above are not going to be solved in the next budget cycle. They took twenty years to compound, and they will take a decade to unwind. The question for finance leaders, both women who are climbing and the CFOs who influence who climbs, is what can actually be done inside an organization in the next twelve months.
For women in finance positions below the CFO level, the honest answer is that the career moves are specific and a little uncomfortable. Ask for the line role. Request the capital project. Build sponsorship around useful work, not around networking. Accept that visibility matters more than it should. Know the mobility constraints you have, and compensate with external visibility that does not require relocation.
One underappreciated angle here: women finance leaders on the payer side often have stronger line exposure than their provider counterparts at the same career stage. Medicare Advantage bid strategy, risk adjustment operations, and utilization finance are P&L-heavy roles that translate directly to a provider CFO search. A payer-side VP Finance with direct accountability over a $500 million MA bid is a credible candidate for a provider CFO seat even without hospital tenure, and that crossover path has moved people faster in the last five years than most internal promotion ladders have.
If you are in a director or VP finance role in healthcare, the single highest-leverage move this year is to get your name attached to one decision that moved a P&L line. That one line on your resume is worth more than three years of reporting excellence.
For current CFOs and search committee members, the honest answer is different. The research on sponsorship suggests that intentionality beats good intentions. Most sponsorship happens informally, which means it tracks existing relationships, which means it perpetuates existing demographics. Organizations that have meaningfully moved the needle on women in finance leadership did so by formalizing sponsorship pairings for high-potential mid-career women and by tracking line role rotations by gender.
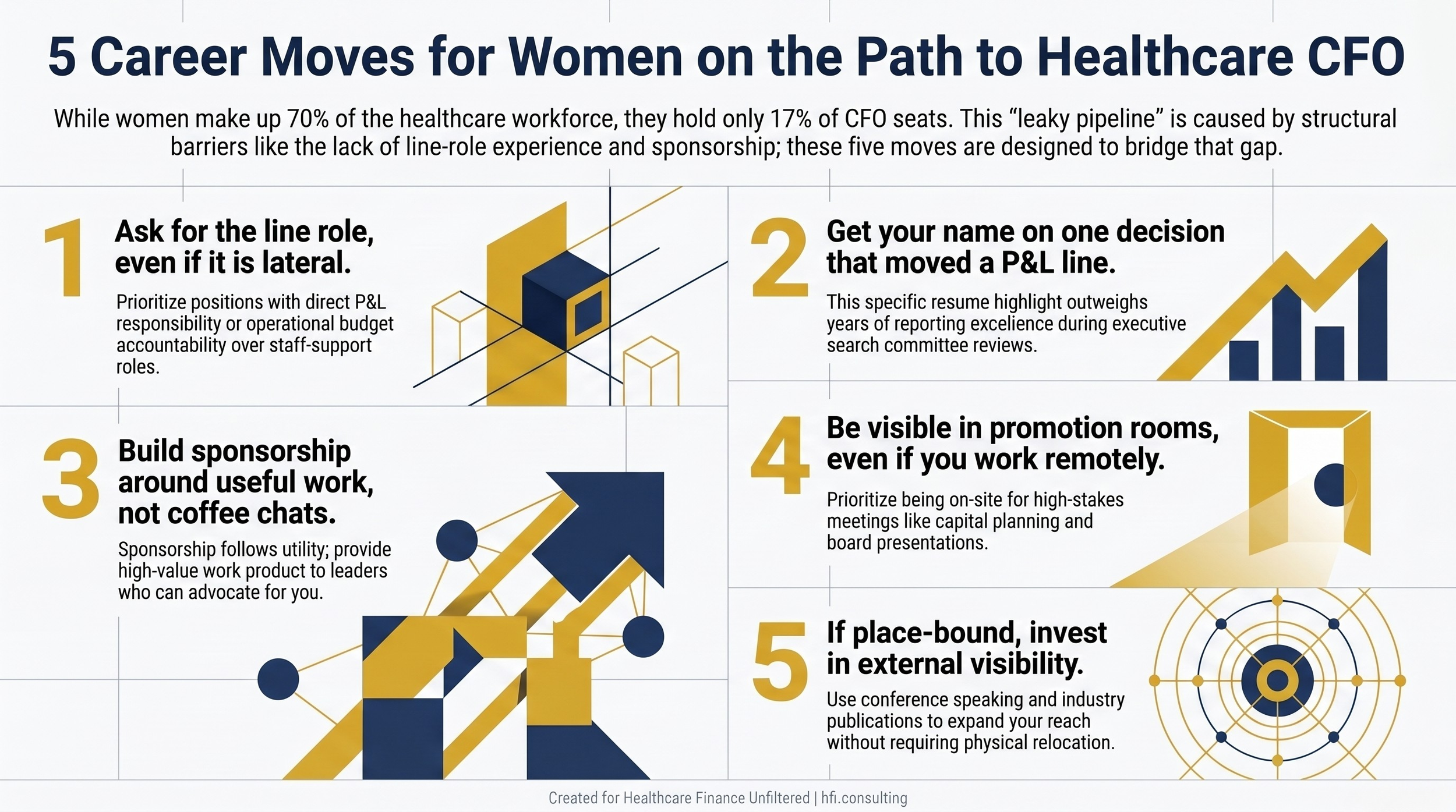
Portrait infographic listing five career moves for women in healthcare finance aiming for the CFO seat: request line roles, own P&L decisions, cultivate sponsors, stay visible in key rooms, and build external credibility.
The Moves That Compound
Five moves that compound over a five-year horizon are worth more than any single big promotion:
Get direct P&L exposure, even if it means a lateral move. Build a relationship with one senior executive who has actually recommended someone for promotion in the last year. Be visible in the rooms that make promotion decisions, not just the rooms that execute them. Invest in external credibility through speaking or writing that does not depend on your employer. And when you do look at a new role, evaluate it against the three questions every CFO search asks: what revenue did you influence, what margin did you improve, and what capital decision did you lead.
These are not radical ideas. They are the same moves that have worked for the men who now hold most of the seats. The work is in applying them consistently across a decade, which is exactly how most of the women now in CFO roles got there.
P.S.
What barrier have you actually seen at work in your own organization or career? The line-versus-staff divide, the sponsorship gap, the flexibility tax, or something else entirely? Hit reply and tell me. I read every response, and the patterns across answers are often more useful than any single study.