
When the Front Office Fails: What Medical Practice Inefficiency Really Costs Patients and CFOs
A broken IVR and an unresponsive portal aren't IT problems. They are a CFO-level revenue failure.
I fired a doctor I genuinely liked.
Not because the clinical care was poor. Not because the diagnosis was wrong or the bedside manner left something to be desired. I fired a physician who was excellent at medicine because his front office made it functionally impossible to be his patient.
For two years, I navigated a phone tree where Option 1 rang indefinitely or held me past 30 minutes with no resolution. The patient portal had gone through a system migration that left a required location field with no selectable options, which meant no messages could be sent at all. Prior authorization questions went to a voicemail with a three-day callback window. The only reliable way to communicate with this practice was to drive 20 minutes and show up in person.
When I finally needed to cancel an appointment and could not reach anyone to do it, I just did not show. That was my exit.
What I experienced as a patient is what a Medical Group CFO should be reading as a financial emergency.
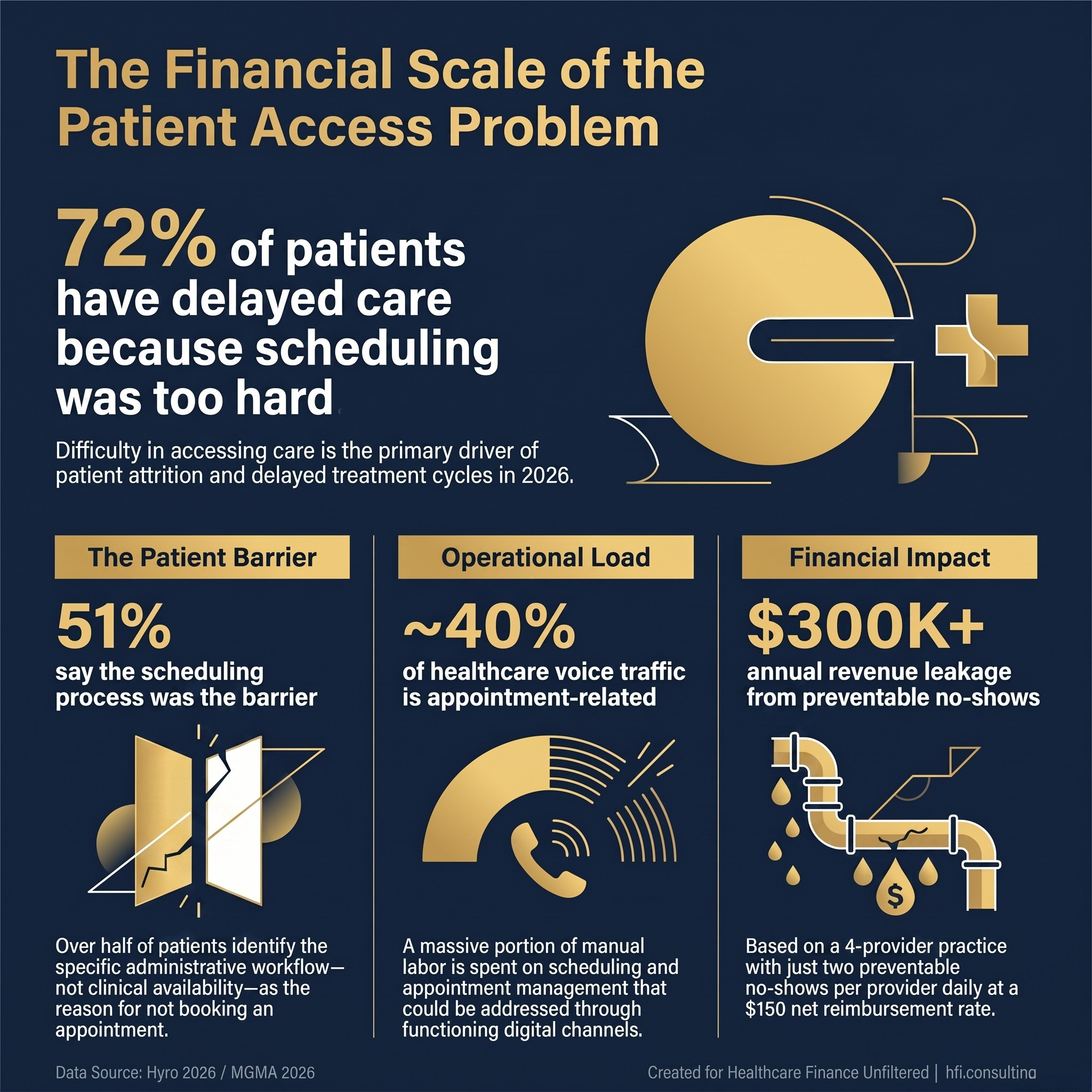
Stat card showing patient access barriers: 72% delayed care, 51% frustrated by scheduling, 40% of calls are appointment-related, $300K no-show revenue leak
The Front Office Is a Revenue Function, Not an Administrative One
Healthcare finance leaders have spent years optimizing the back end of the revenue cycle. Denial rates, clean claim percentages, days in AR, prior authorization turnaround times. The metrics are well-understood, the benchmarks are published, and the vendor landscape is mature.
The front office rarely gets the same treatment. It is staffed, it is managed, and it is largely left alone until patient complaints become loud enough to warrant attention.
That framing is a mistake.
Every patient interaction at the front desk, on the phone, or through a portal is a revenue event in disguise. A scheduled appointment generates revenue. A cancelled appointment that was preventable generates nothing. A patient who cannot reach the practice to reschedule becomes a no-show. A no-show on a four-provider schedule, conservatively estimated at two per provider per day at $150 net reimbursement per visit, is $300 in unrecoverable lost revenue per provider per day. Across a small medical group running 250 days a year, that number compounds to $300,000 in annual leakage before anyone runs a single denial report.
That math does not appear on most contribution margin dashboards. It should.
What the Data Is Telling Practice Leaders in 2026
The operational pressure on medical practice front offices is not an isolated or anecdotal problem. A January 2026 MGMA Stat poll of 226 practice leaders found that automation and process fixes were the top two cost-cutting priorities, together representing more than half of all responses, specifically targeting front-desk tasks, contact center workflows including call routing, callbacks, and self-service, and IVR systems.
That result is significant because it reflects where practice administrators believe their cost pressure actually lives. The back-office billing team is not the primary target. The phone queue is.
According to Hyro's 2026 patient communications analysis, 72% of patients have delayed care because getting an appointment was too difficult, and 51% say the scheduling process itself was the barrier. Meanwhile, 93% of providers say they expect patients to be comfortable using digital tools, and 86% of patients say they are. The gap is not about willingness. It is about whether the system can actually complete the task.
That distinction matters to a CFO because it reframes the problem. The question is not whether the practice has a portal. The question is whether the portal works end to end. In my case, it did not. The system could start a request. It could not finish one.
MGMA polling data from early 2026 shows that medical groups are directing 37% of new strategic budget dollars toward workforce stabilization, 30% toward health IT and cybersecurity, 12% toward revenue cycle automation, and 12% toward patient access channels. Patient access channels are receiving real investment. The question is whether that investment is being governed well enough to prevent exactly the kind of failure I experienced.
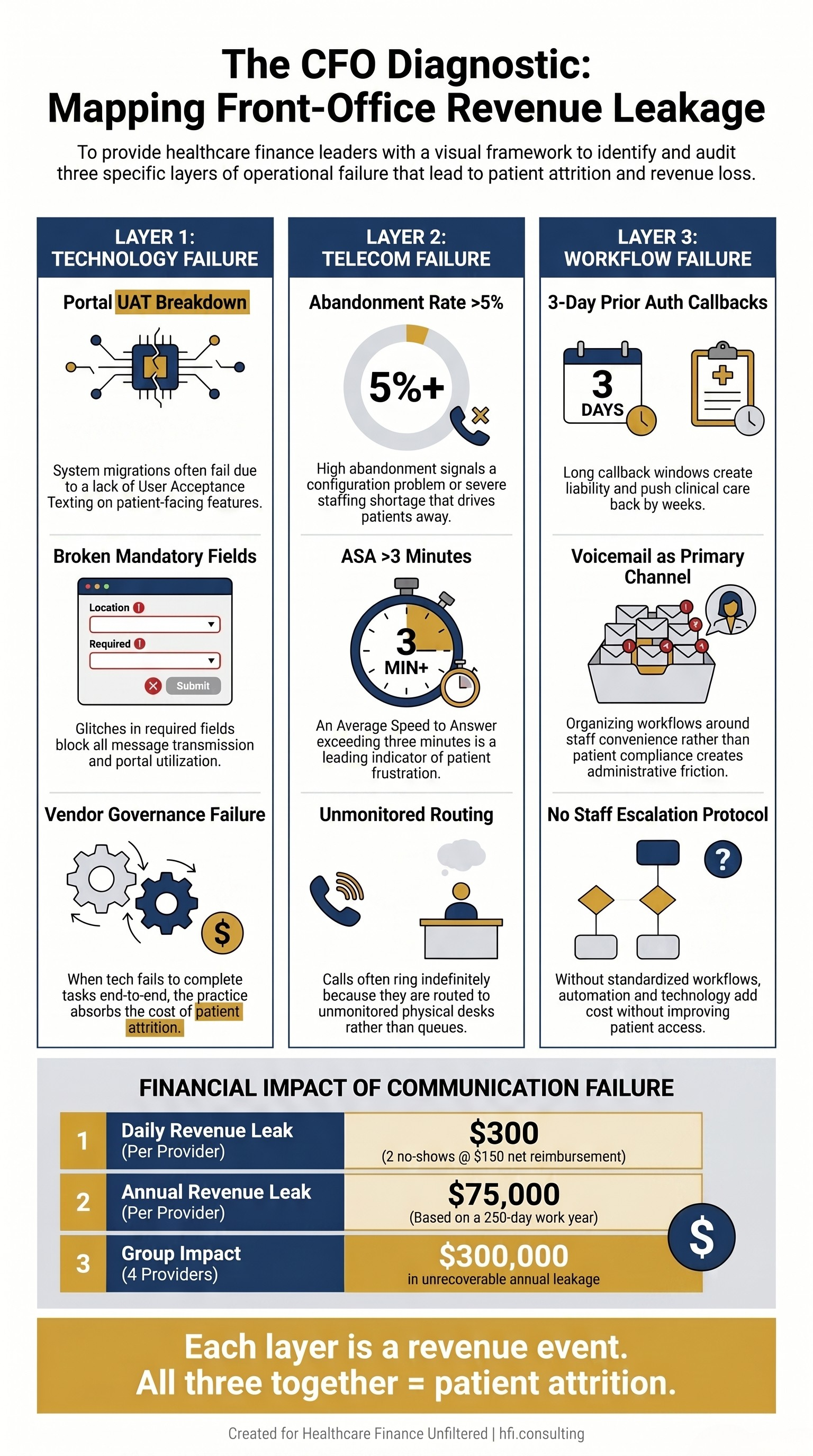
The Three-Layer Breakdown Finance Leaders Need to Audit
When I describe what happened at that practice, I am describing three distinct operational failures that a CFO would recognize immediately if they were mapped as revenue cycle events.
Layer One: Technology Rollout Without User Acceptance Testing
The portal migration that left a blank location dropdown was not a minor glitch. It was a complete failure of pre-launch quality control. A clinical workflow audit is the standard first step for identifying EHR bottlenecks. When a patient-facing system goes live with a broken mandatory field that blocks all message transmission, it means the practice management or IT team failed to run basic test cases mimicking a patient's journey before launch.
From a finance perspective, this is vendor governance failure. If a technology vendor delivered a broken implementation and the practice did not catch it through UAT, the practice absorbed the full cost of that failure in the form of suppressed portal utilization, elevated inbound call volume, and patient attrition.
Layer Two: Telecom Metrics Nobody Was Watching
A phone line that rings indefinitely is not a staffing problem. It is a configuration problem that a basic telecom audit would surface immediately.
Two KPIs should trigger automatic escalation in any well-managed practice: call abandonment rate and average speed to answer. In healthcare call center management, a call abandonment rate above 5% is a standard threshold for intervention. A 30-minute wait time that consistently ends in abandonment means the scheduling department is severely understaffed or the phone routing logic is broken. A line that rings without hitting a voicemail or queue cap typically indicates the phone system is misconfigured, routing calls to unmonitored physical desks rather than a centralized queue.
Neither of those conditions is invisible. Both show up clearly in standard telecom reporting. The practice I left was generating those signals every single day. Nobody was reading them.
Layer Three: Asynchronous Voicemail as a Primary Workflow
A three-day callback window for prior authorizations is not a workflow. It is a liability.
Prior authorization timelines are time-sensitive by definition. A three-day administrative delay on the practice side can push a patient's actual care back by weeks. It signals a culture that has organized itself around staff convenience rather than patient compliance. And it creates a downstream documentation gap that shows up as denial exposure when the authorization clock runs out.
Dedicated prior authorization software can reduce time spent on this process by over 50% by electronically checking payer requirements in real time, auto-populating request forms from EHR data, and submitting requests directly to insurance portals. The technology exists. The decision not to use it is a finance decision, whether it is recognized as one or not.
Three-column framework showing technology, telecom, and workflow failure layers in medical practice patient access and their revenue impact
No-Shows Are Not a Patient Behavior Problem
Here is the part of this story that tends to get missed in the clinical framing of no-show rates.
When I did not show for that final appointment, I was not being irresponsible. I was responding rationally to a system that had made cancellation impossible. I tried to cancel through the portal. The portal was broken. I tried to call. The wait time was more than 30 minutes, I even tried faxing my cancellation from the office fax machine. I had no other option the practice had made available to me.
By making it impossible for patients to get through to cancel, a practice forces those patients into no-show status. From a healthcare finance and operations perspective, no-shows are an absolute drain on clinic revenue. Every empty time slot represents unrecoverable lost revenue. The fixed costs, including rent, salaries, and utilities, remain identical whether the provider sees a patient or sits in an empty room.
The practice I left built a communication structure that made responsible patient behavior structurally impossible. Then they absorbed the financial cost of the behavior they created.
Interaction data shows that nearly 40% of healthcare voice traffic is appointment-related, including new scheduling and appointment management. When that volume still lands on human agents, it is not because patients prefer the phone. It is because the phone remains the most reliable way to force an outcome in systems that cannot complete tasks end to end.
This is the operational reality that a CFO needs to understand. Patients are not calling because they want to. They are calling because the digital option failed them.
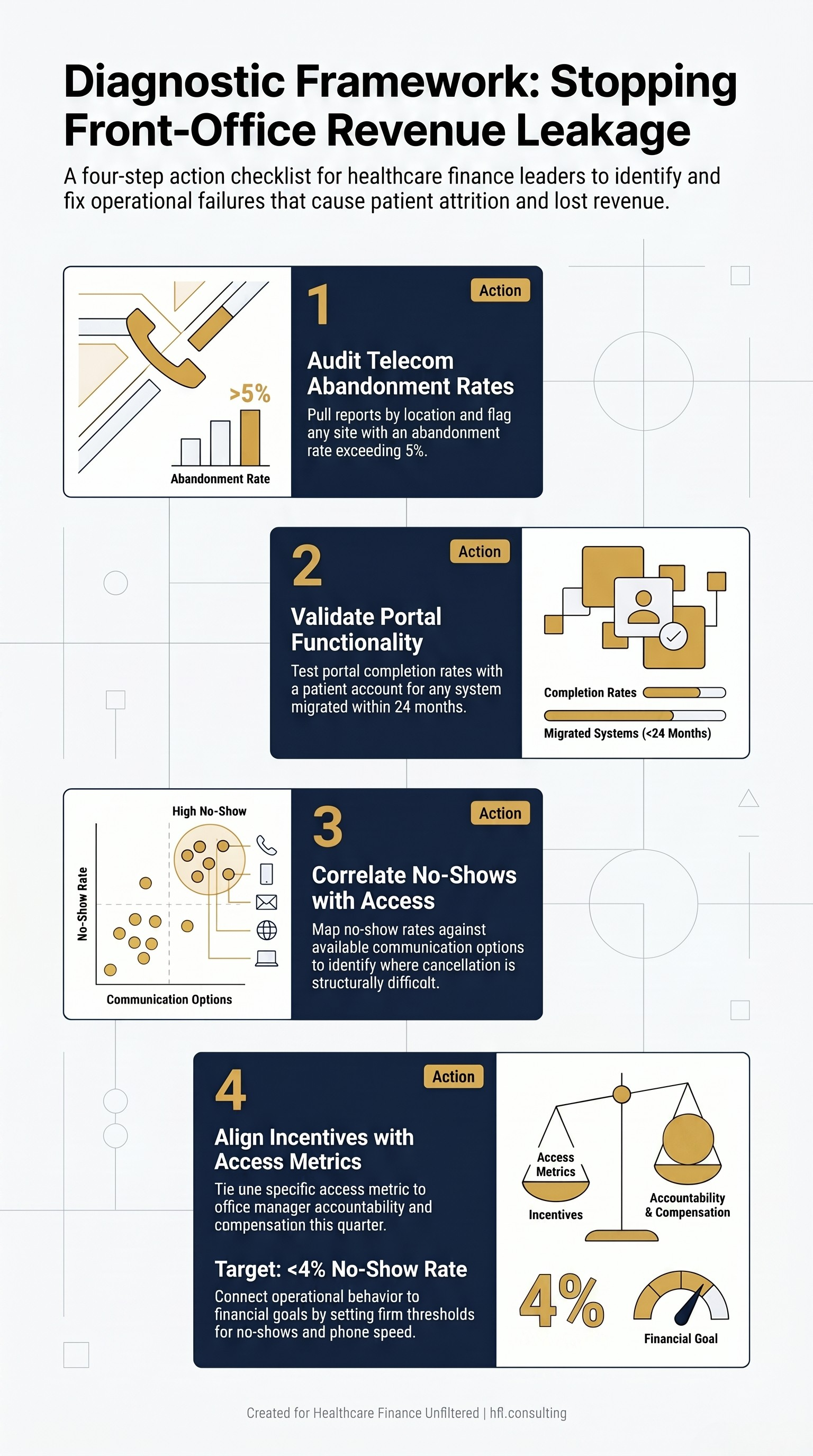
The CFO Diagnostic Framework
If you are a Medical Group CFO reading this and wondering whether you have a version of this problem in one of your locations, the answer is almost certainly yes somewhere in your portfolio. Here is where to look.
Start with telecom reporting. Pull abandonment rates and average speed to answer by location. Any location running above a 5% abandonment rate or above a 3-minute average speed to answer is generating patient attrition you are not capturing in your financial statements.
Audit portal completion rates after any system migration. A drop in portal message volume following an EHR transition is not a patient behavior change. It is a broken workflow. Confirm with a test patient account before assuming the new system is functioning.
Map your no-show rate against your patient communication options. If a location has above-average no-show rates and limited ways for patients to cancel, you are not managing a clinical problem. You are managing a revenue leak that has an operational solution.
Tie office manager accountability to access metrics. A strategic CFO aligns operational behavior with financial goals by connecting office manager compensation directly to specific operational targets: bringing the no-show rate below 4%, reducing phone abandonment to under 3%, and maintaining patient satisfaction scores above a defined threshold. When access metrics are tied to manager compensation, workflows change quickly.
This is the lever that transforms patient access from a service issue into a managed financial function.
Four-step CFO diagnostic checklist for auditing medical practice patient access and identifying no-show revenue leakage
What This Looks Like at the Health System Level
The medical group context is the most direct, but this dynamic scales.
Health systems that own physician practices or employ medical groups inherit these operational failure modes. A broken front office at a primary care location does not just generate no-shows. It leaks referrals. Patients who cannot reach their primary care physician to coordinate a specialist referral find another path, often outside your network.
MGMA data indicates that AI-driven call centers and automated self-check-in kiosks are gaining traction as strategies to remove low-value tasks from front desk staff, specifically targeting the front-office churn driven by administrative burden and the compounding costs of turnover in medical assistant and scheduling roles.
The investment case for these tools is not primarily about patient satisfaction scores. It is about revenue protection, referral retention, and labor productivity. That framing belongs in a CFO conversation, not just an operations review.
If you are assessing a physician practice acquisition or a medical group integration, front office operational metrics should be on your due diligence checklist alongside payer mix and AR aging. A location with a 15% no-show rate and a broken portal is not an IT problem you are inheriting. It is a revenue problem you are paying for at acquisition price.
The Tools Exist. The Governance Does Not.
I want to be direct about something the source data makes clear.
The technology to prevent everything I experienced exists and is widely available. Voice AI for call routing and scheduling. Patient portal automation. Prior authorization workflow tools. Telecom analytics dashboards. MGMA polling shows that practice leaders plan to automate revenue cycle management workflows, clinical documentation, scheduling, contact center call routing, callbacks, self-service, message categorization, and front-desk tasks as primary cost-cutting initiatives in 2026.
The problem is not technology availability. The problem is that adding technology without removing broken steps adds cost without fixing access. MGMA's own analysis notes explicitly: if you add tech but do not remove steps, you add cost. The most important caveat in the automation investment case is that process fixes are the glue that makes automation work. Automation fails without standardized workflows.
The practice I left almost certainly thought they had modernized when they migrated their portal. They had added a channel. They had not fixed access. The distinction cost them a patient, and it cost the patient two years of unnecessary friction with a physician who was otherwise worth keeping.
That is the story a CFO should be telling their operations team.
At HFI Consulting, I work with CFOs on service line financial assessments that include front-office operational metrics as part of the contribution margin picture. If you are managing a medical group or physician enterprise and want to pressure-test your patient access infrastructure against your financial performance, I would be glad to connect. Reach out at hfi.consulting.
What Finance Leaders Should Do in the Next 90 Days
The diagnostic work here is not complicated. It is just undervalued.
Pull your telecom abandonment data. Run a portal UAT on any system migrated in the last 24 months. Map no-show rates against communication channel availability at each location. Tie one access metric to office manager accountability this quarter.
None of that requires a capital investment. It requires treating the front office as a revenue function with the same rigor you apply to your denial rate.
The patients you are losing to broken phone trees are not switching practices because they found better clinical care. They are switching because your operations made it easier to leave than to stay.
That is a fixable problem. And it is a finance problem.
If this article surfaced a gap you are actively navigating, I would like to hear about it. Hit reply and tell me: what is the single biggest front-office operational failure driving financial leakage in your organization right now?
P.S. Have you ever left a provider because of front-office dysfunction rather than clinical quality? I would genuinely like to know how common this is among the finance leaders reading this. Hit reply.