
The Latest Prior Authorization Reform: The CFO's Financial Planning Guide for CMS-0057-F
Tighter timelines, mandatory APIs, and public denial metrics are live. What changes in your budget starts now.
Why This Matters Right Now
CMS published its roadmap for electronic prior authorization on May 5, 2026, and the headline is not that change is coming. The headline is that part of it already arrived. As of January 1, 2026, impacted payers across Medicare Advantage, Medicaid, CHIP, and Marketplace plans are legally required to return prior authorization decisions within 72 hours for urgent requests and 7 calendar days for standard requests. That is not a proposal. It is an operational mandate with public accountability attached.
For CFOs on both sides of the payer/provider divide, the 2026 PA reform cycle is not a single deadline. It is a phased infrastructure overhaul with financial consequences at each stage. Getting the sequence wrong will cost you more than the PA process itself.
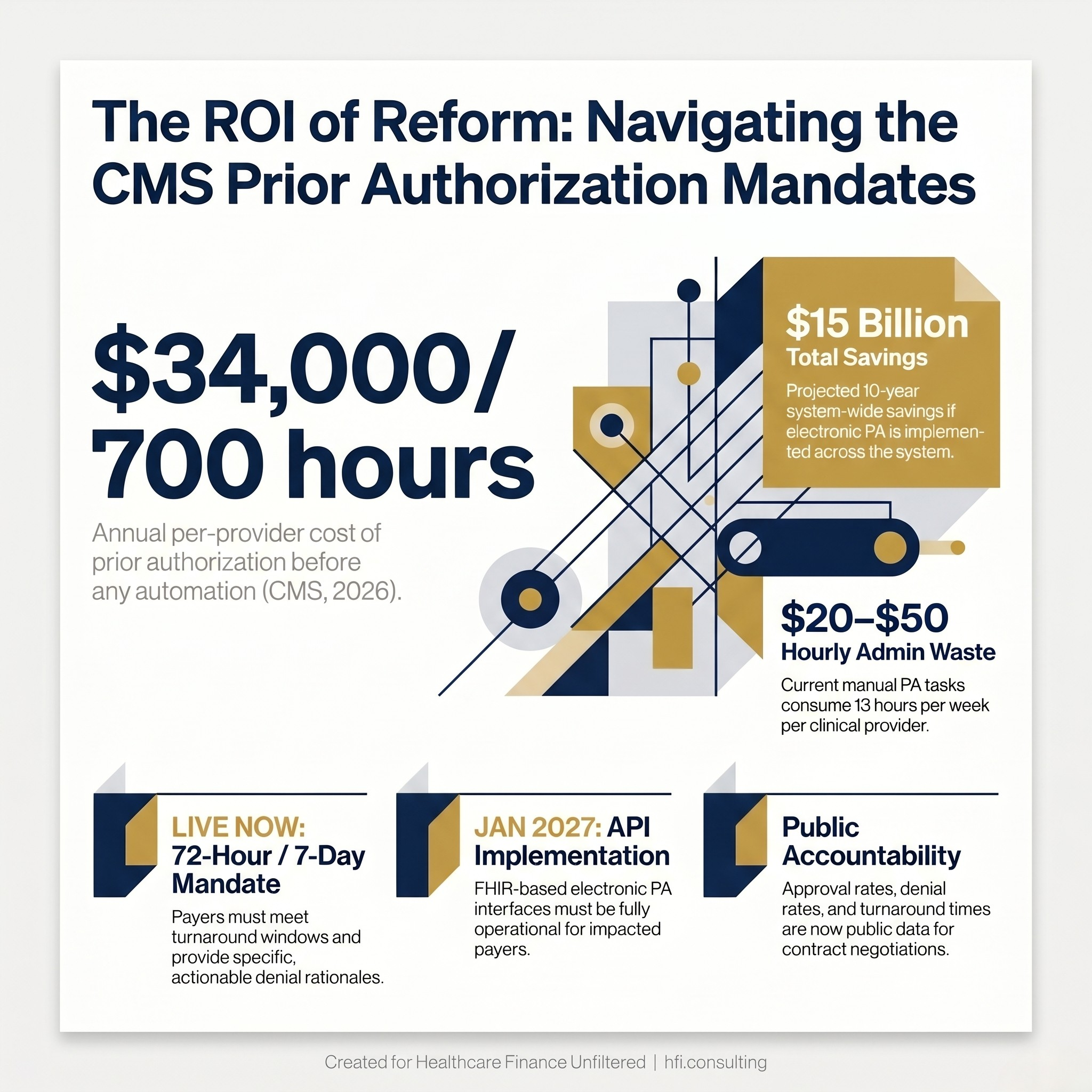
Infographic showing prior authorization costs $34,000 and 700 hours per provider annually, with $15 billion in projected system-wide savings from CMS electronic PA reform.
What CMS Actually Changed (And What's Still Coming)
The prior authorization problem has been documented for years. CMS Administrator Dr. Mehmet Oz put the numbers in plain terms in the May 5 blog: completing prior authorizations costs healthcare providers $20 to $50 per hour and consumes an average of 13 hours per week per provider. That adds up to roughly $34,000 and 700 hours per year, per clinician, in administrative overhead that does not contribute one dollar of clinical value.
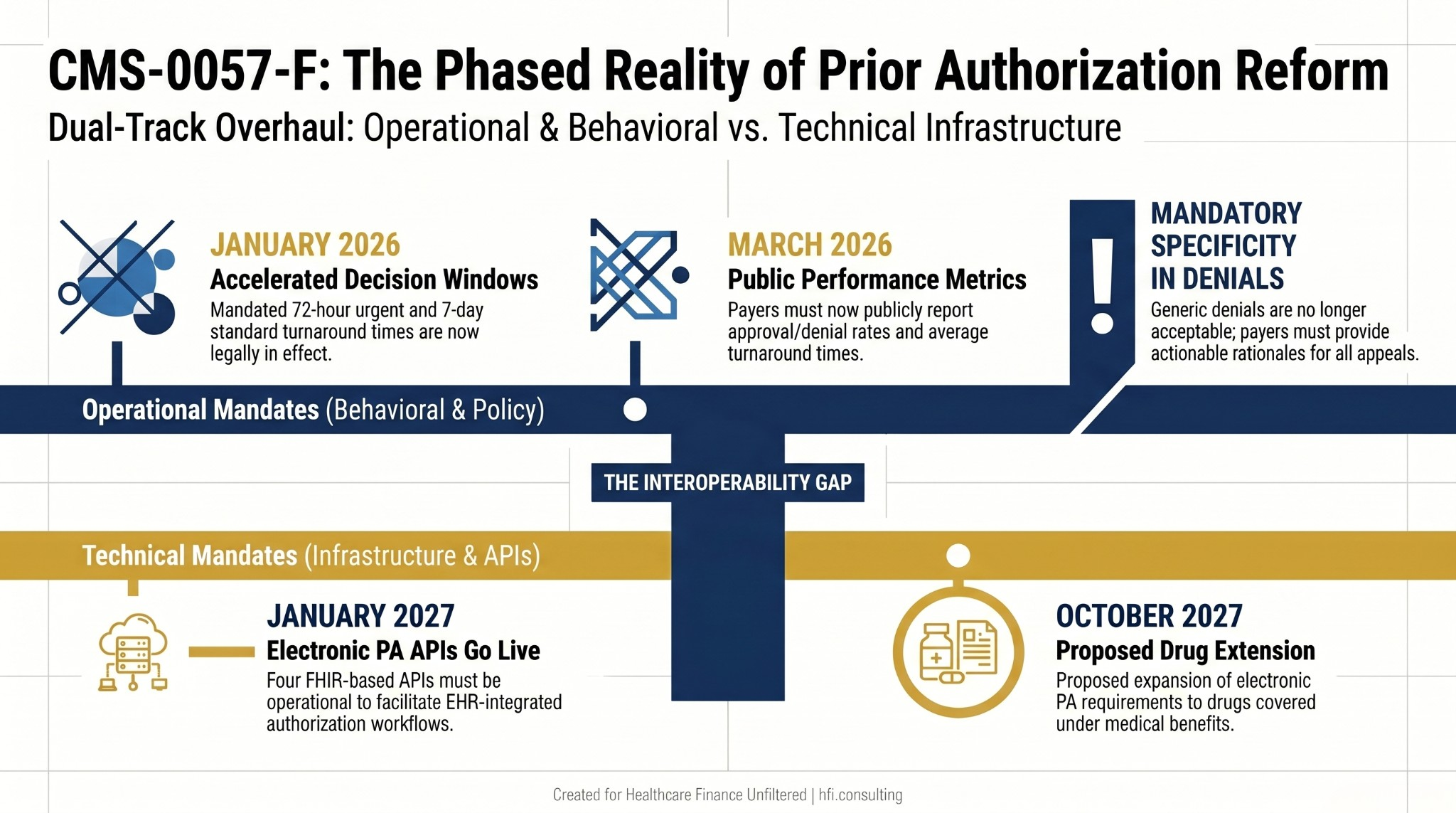
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) is the regulatory vehicle trying to close that gap. Here is the full implementation timeline:
What is live now (January 2026): Impacted payers must meet the 72-hour urgent and 7-day standard turnaround windows. Generic denials are no longer acceptable. Payers must provide specific, actionable denial rationales to support appeals and resubmissions.
What went live in March 2026: Public reporting requirements. Payers are now required to publish approval rates, denial rates, and average turnaround times. This means your payer relations team can now run a comparison before contract negotiations, and your patients can see it too.
What is coming January 2027: Electronic PA APIs go live. Four FHIR-based interfaces (Patient Access, Provider Access, Payer-to-Payer, and Prior Authorization) must be operational at impacted payers. EHR-integrated electronic PA workflows will become the standard, with eventual incorporation into Medicare Promoting Interoperability and MIPS scoring for clinicians.
What is proposed for October 2027: Extension of electronic PA requirements to drugs covered under medical benefits, using NCPDP standards for pharmacy and FHIR for medical items. This is still in the proposed rule stage, but the direction is clear.
The 10-year savings estimate from CMS is $15 billion across the system. The question is who captures those savings and who absorbs the transition cost to get there.
Timeline showing CMS prior authorization reform in two tracks: operational mandates effective 2026 and technical API mandates effective 2027, with proposed drug coverage extension in October 2027.
The Revenue Impact: Health Systems and Payers Are Not in the Same Position
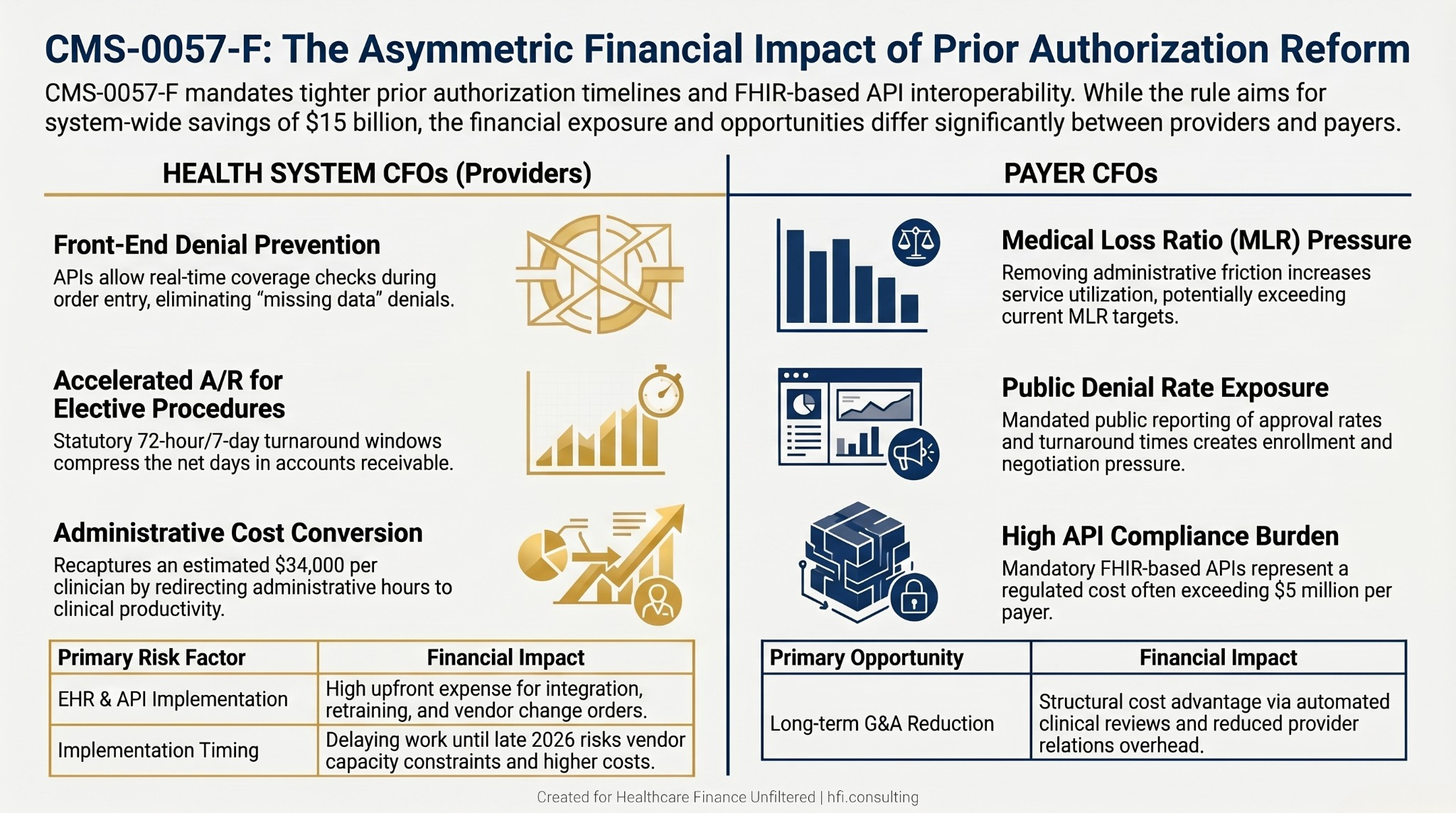
This rule does not affect providers and payers symmetrically. The financial exposure and the financial opportunity are distributed differently, and CFOs need to model both.
For Health System CFOs
The revenue upside from PA reform falls into three categories.
Denial prevention at the front end. Electronic PA APIs allow providers to check coverage requirements before submitting the authorization request. This addresses the "missing data" denial problem, which is one of the most preventable and most expensive failure points in the revenue cycle. If your team is receiving denials for incomplete documentation on authorization requests, that cost profile changes when the payer's requirements are visible in your EHR at the time of order entry.
Accelerated cash flow for elective procedures. The 7-day standard timeline replaces a process that often stretched to 14 or 21 days under manual workflows. For high-dollar elective procedures in orthopedics, cardiovascular, and oncology service lines, that compression in turnaround time directly improves net days in A/R. The administrative cost of follow-up on pending authorizations is also reduced when the timeline is statutory rather than negotiated case by case.
Operational conversion of administrative hours to clinical productivity. The $34,000 per provider per year estimate from CMS is not a fixed cost. It is recoverable capacity. Organizations that redesign PA workflows around electronic tools can redirect clinical staff time toward care delivery activities. That is a margin recapture argument, not just a cost reduction argument.
The risk profile for health systems is implementation cost and timing. EHR upgrades, API integration, staff retraining, and workflow redesign all carry upfront expense. Organizations that delay this work until late 2026 will compete for constrained vendor capacity heading into the January 2027 API deadline.
For Payer CFOs
The calculus runs in the opposite direction on several dimensions.
Medical loss ratio pressure. Electronic PA that is genuinely faster and more transparent reduces the "soft denial" effect: the abandonment rate that occurs when prior authorization is difficult enough to navigate that patients and providers give up. When that friction is removed, utilization goes up. Payers who model next year's MLR using current utilization assumptions without accounting for the friction removal effect are going to miss their targets.
Implementation cost is the primary regulated entities' burden. The four FHIR-based APIs must be built and maintained by payers. CMS has engaged with EHR vendors and health IT developers directly, but the compliance obligation sits on the plan side. The February 2026 WEDI survey finding that 25% of payers estimate API implementation will exceed $5 million reflects the real cost range, and that estimate was reported to be rising.
Competitive exposure through public reporting. As of March 2026, denial rates and turnaround times are public. Plans with materially higher denial rates or slower turnaround will face enrollment pressure during open enrollment periods. "Easy access to care" is now a measurable metric, not a marketing claim.
Long-term G&A reduction. The case for investing in electronic PA is not purely defensive. Plans that automate the clinical review and provider relations components of PA workflows will see sustained reductions in G&A expense. The organizations that front-load the infrastructure investment in 2026 will have a structural cost advantage by 2028.
Side-by-side comparison table showing prior authorization reform revenue drivers and risks for health system CFOs versus payer CFOs under CMS-0057-F.
The CFO Action Framework: Five Steps for the Next 90 Days
Step 1: Quantify Your Current PA Cost Burden Before You Budget for Reform
Before you can model the ROI on electronic PA investment, you need a baseline. Most health systems and health plans do not have this number sitting in a report. Building it requires pulling data from three places: labor hours in your authorization processing workflow, denial volume and root cause codes attributable to authorization failures, and days-in-limbo for high-dollar elective procedures pending PA decisions.
When I was tracking productivity and operational metrics across seven hospitals at Ascension, the administrative cost of clinical workflows was almost always underestimated on the cost report because the time was embedded in nursing, case management, and physician office staff hours rather than captured as a discrete PA cost center. That measurement gap makes it harder to build the business case for investment. Fix the measurement before you go to the capital committee.
Step 2: Map Your 2027 API Readiness Gap Right Now
The January 2027 deadline for electronic PA API implementation is eight months away. EHR vendors are the primary integration point, and Epic, Cerner/Oracle Health, and MEDITECH are at different stages of readiness for different plan configurations.
Your readiness assessment needs to answer four questions. Is electronic PA functionality available in your current EHR version? Which payer APIs have gone live and are testable today? What workflow redesign is required before your clinical staff can use the tool effectively? And what does your vendor contract say about implementation costs for new API functionality?
If your current contract is silent on API implementation costs, you are likely to get a change order. Negotiate that before the deadline creates leverage for the vendor.
Step 3: Model the MLR and Utilization Impact Before Next Budget Cycle
Payer finance teams should build a scenario where the 11% reduction in prior authorization volume that leading health plans have already implemented becomes the industry floor. CMS documented that one large national plan is eliminating authorization requirements for 30% of healthcare services. If that becomes a competitive standard, plans that maintain high authorization volume will face network access pressure and enrollment risk simultaneously.
The utilization modeling question for plan CFOs is not whether removing PA friction increases utilization. It does. The question is how much, across which service lines, and whether your network contracts are structured to absorb that volume at sustainable rates. Build three scenarios: conservative (utilization increases 3-5%), moderate (5-8%), and stress (8-12%). Know which one breaks your MLR before your actuary tells you.
Step 4: Leverage the Public Denial Data in Payer Contracting
For health system CFOs, the March 2026 public reporting requirement is a contract negotiation tool that most organizations have not yet built into their managed care strategy. If a payer's denial rate for a specific service line is materially higher than peers, that data now exists in a format you can present in a contract discussion.
This is the connection between the CMS Interoperability and Prior Authorization Rule 2027 compliance requirements and your managed care contracting team's work. They need to be in the same conversation.
If your revenue cycle or payer relations infrastructure needs a diagnostic before you can execute this framework, HFI Consulting works with health systems and payer organizations on exactly this kind of assessment. You can reach us at hfi.consulting.
Step 5: Build the Whistleblower Risk Into Your Compliance Model
The False Claims Act implications of PA processes that are knowingly designed to delay or deny legitimate claims are not hypothetical. The enforcement environment in 2026 is active, and CMS has made clear through the Aetna settlement and related enforcement actions that documentation asymmetry creates exposure.
For payer compliance teams: if your denial rationale documentation does not meet the specificity standard that CMS-0057-F requires, your current denial volume is not just a provider relations problem. It is a compliance exposure.
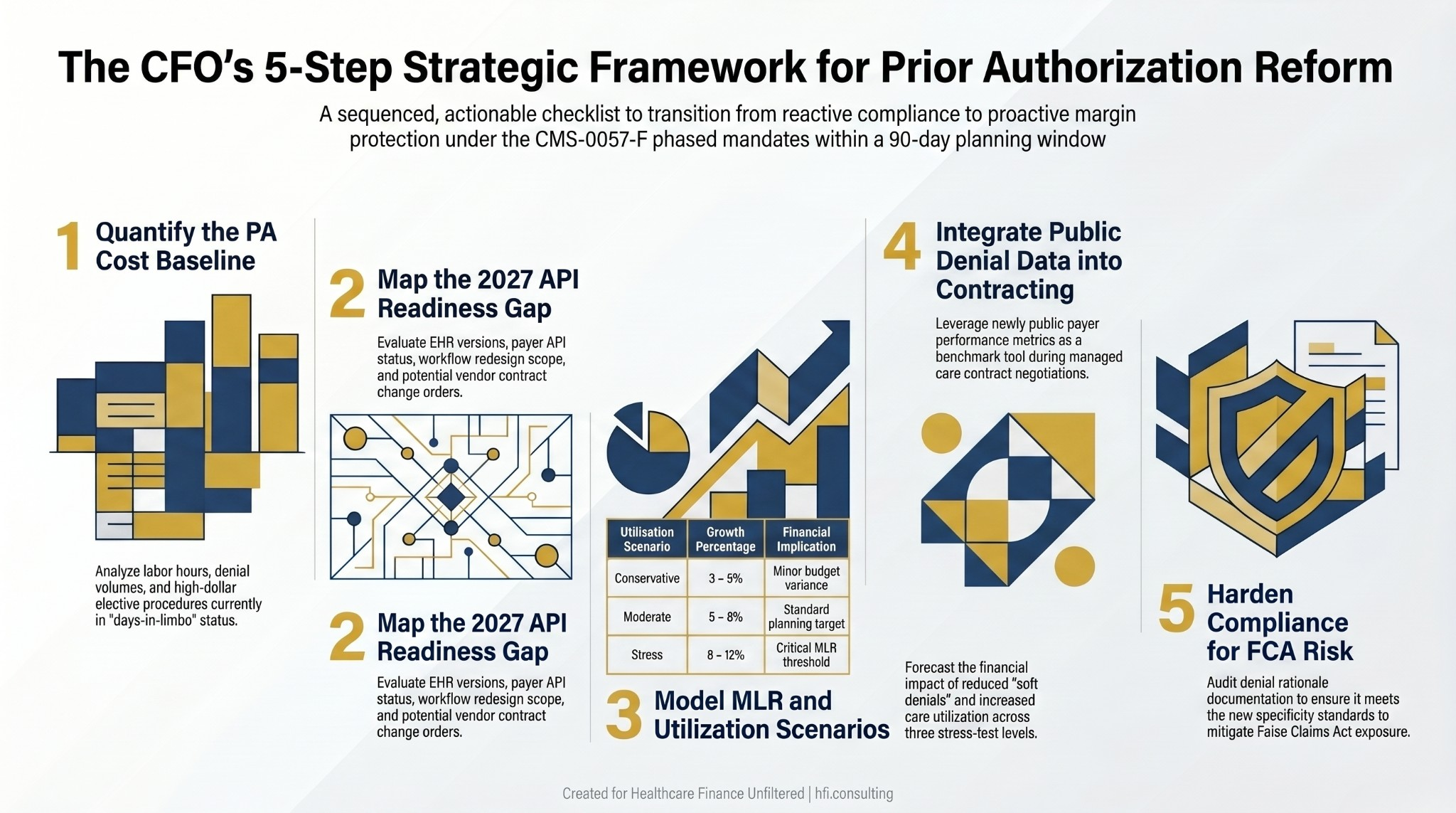
Five-step CFO action framework for CMS prior authorization reform compliance, covering cost baseline, API readiness, MLR modeling, contracting strategy, and compliance risk.
What This Signals for Healthcare Finance Infrastructure
The prior authorization reform is not happening in isolation. It is part of a pattern: CMS is mandating that the administrative layer of healthcare move onto modern electronic infrastructure, one rule at a time. The claims attachment standards rule with its May 2028 deadline, the interoperability requirements, and now the PA electronic API mandate all follow the same architecture.
For CFOs who have read the CMS interoperability rules as a series of disconnected compliance deadlines, the frame to adopt instead is infrastructure investment with a phased schedule. The organizations that build electronic data exchange capability proactively will pay lower transition costs on every future mandate. The organizations reacting at each deadline will keep paying the premium.
The $15 billion in projected 10-year savings that CMS cites is real. The question is whether your organization is positioned to capture the margin improvement or absorb the compliance cost while the benefit flows elsewhere.
For an analysis of how the FHIR workflow changes connect to broader healthcare process automation, see the Healthcare Process Automation CFO Guide at rachelbarksdale.substack.com/p/healthcare-process-automation-cfo?r=1077bg.
For the payer-side revenue cycle implications of denial pattern changes, the analysis in The Denial Loop Is Breaking Healthcare remains directly relevant: rachelbarksdale.substack.com/p/the-denial-loop-is-breaking-healthcare?r=1077bg.
What CFOs Should Do Before the Next Planning Cycle
The 2027 API deadline is close enough that budget planning decisions made in the next 60 to 90 days will determine whether your organization is in front of this transition or reacting to it.
For health systems: complete the PA cost baseline, start the EHR vendor conversation about API readiness, and integrate public denial rate data into your next managed care contracting cycle.
For payer finance teams: run the MLR sensitivity analysis on PA utilization changes, get a realistic implementation cost estimate from your IT team, and validate that your denial rationale documentation meets the specificity standard now in effect.
The goal posts have moved. The CFOs who update their models before the next budget season will have more options than the ones who update them after.
If your organization wants a structured review of your PA cost burden, denial root cause profile, or payer API readiness before the 2027 deadline, connect with HFI Consulting at hfi.consulting.
P.S. Prior authorization reform affects payers and providers differently. Which side of this is creating more urgency in your organization right now: the revenue capture opportunity or the compliance and implementation cost? Hit reply and let me know. I'm tracking how finance leaders on both sides are prioritizing this.