
Hospital Workforce Cost Control: CFO Guide to Smarter Pay Strategies and Productivity Tools
Why flat-rate raises are burning your labor budget and what precision compensation actually looks like in 2026
The Labor Budget Reckoning CFOs Cannot Avoid
More than two dozen health systems have announced pay increases since December 2025. HCA invested an additional $10 million in payroll at a single hospital this month, on top of standard merit raises. Providence committed more than $600 million system-wide in merit and market adjustments. Kaiser Permanente finalized agreements covering more than 61,000 employees with average wage growth approaching 30% over the contract period.
The message is clear: labor costs are not coming down. The question every CFO is now facing is whether their compensation strategy is working for them or quietly burning capital they cannot afford to lose.
Running daily productivity dashboards across seven Ascension hospitals in Florida and Alabama gave me a front-row seat to the exhausting rhythm of legacy workforce management. You know the drill. The midnight census comes in. You match it against a static Hours Per Patient Day grid. Someone is over or under on a unit. You spend the next hour trying to pull staff from a sister facility or calling in a nurse at overtime rates. All of it reactive, all of it expensive, and none of it visible until the damage was already done.
That operating model is now colliding with a compensation environment that punishes passivity.
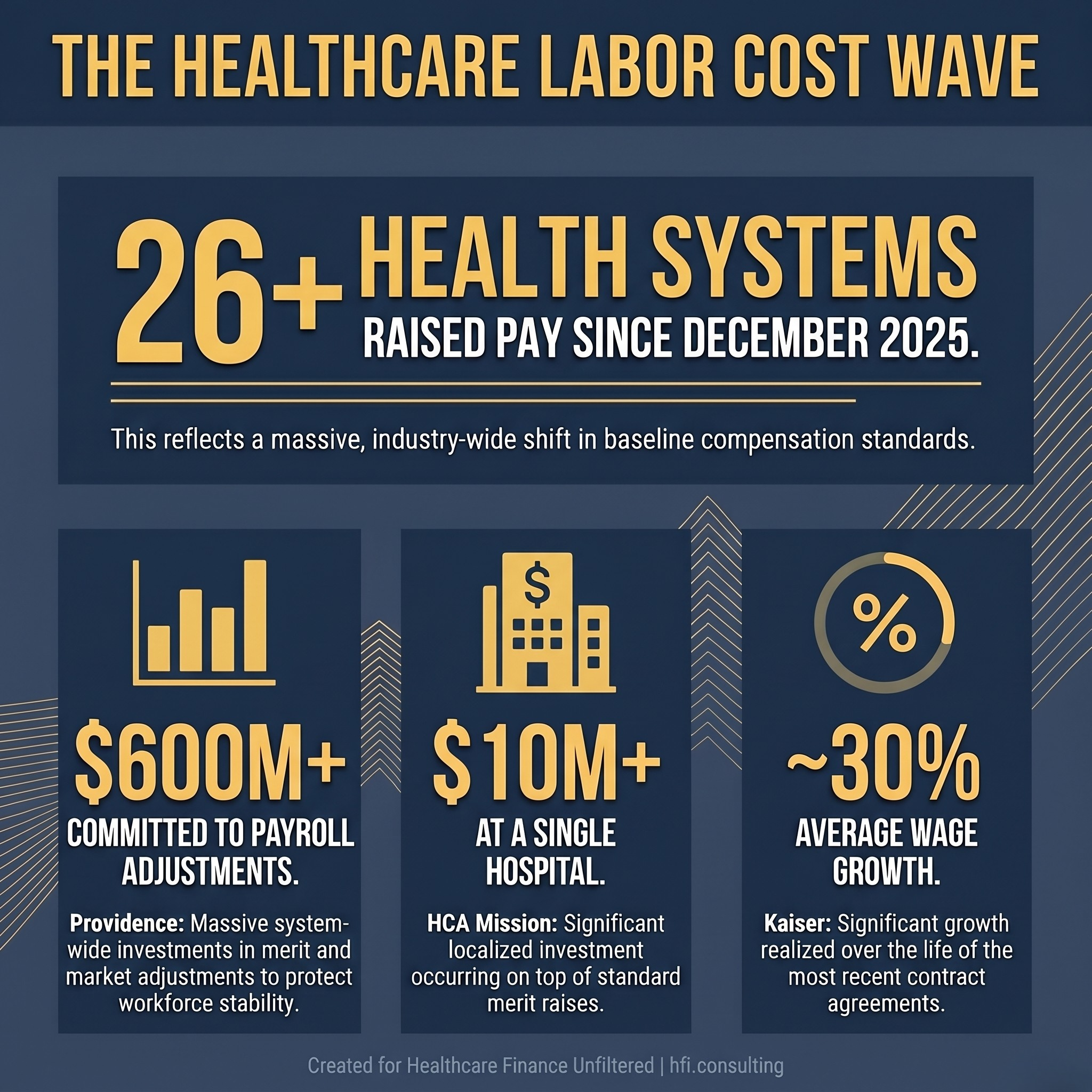
Stat card showing labor cost investments across major health systems in 2026, including Providence at $600 million and HCA Mission Hospital at $10 million.
Why Peanut Butter Raises Are a Margin Problem
The "peanut butter raise" is the practice of spreading a flat percentage increase, typically 2% to 3%, across every position in the organization regardless of market risk, vacancy rate, or clinical impact. It feels administratively clean and culturally safe. It is neither.
When reimbursement rates are fixed and margins are running at 2% to 3%, a misallocated compensation budget is a direct hit to the bottom line. Giving an equivalent raise to a low-turnover outpatient scheduling coordinator and a high-vacancy cardiovascular OR nurse is not equitable compensation. It is misallocated capital.
The operational cost of a single CVOR nurse vacancy goes well beyond a recruitment fee. It degrades surgical throughput, creates downstream scheduling bottlenecks, and frequently results in a travel agency contract at rates two to three times the permanent employee cost. A targeted retention investment in that one position frequently generates more margin protection than a system-wide percentage raise distributed across every role on the payroll.
A recent survey found that 43% of organizations plan to give salary increases to at least 95% of their workforce. The practice is widespread. But health system leaders across the country are pushing back. The CEO of Bronson Healthcare put it plainly: broad-based raises can feel equitable on the surface but fail to distinguish exceptional contribution from average performance. Scripps Health's HR leadership takes it further, noting that merit differentiation compounds over time, creating a growing and sustainable gap between their top performers and what competitors can offer.
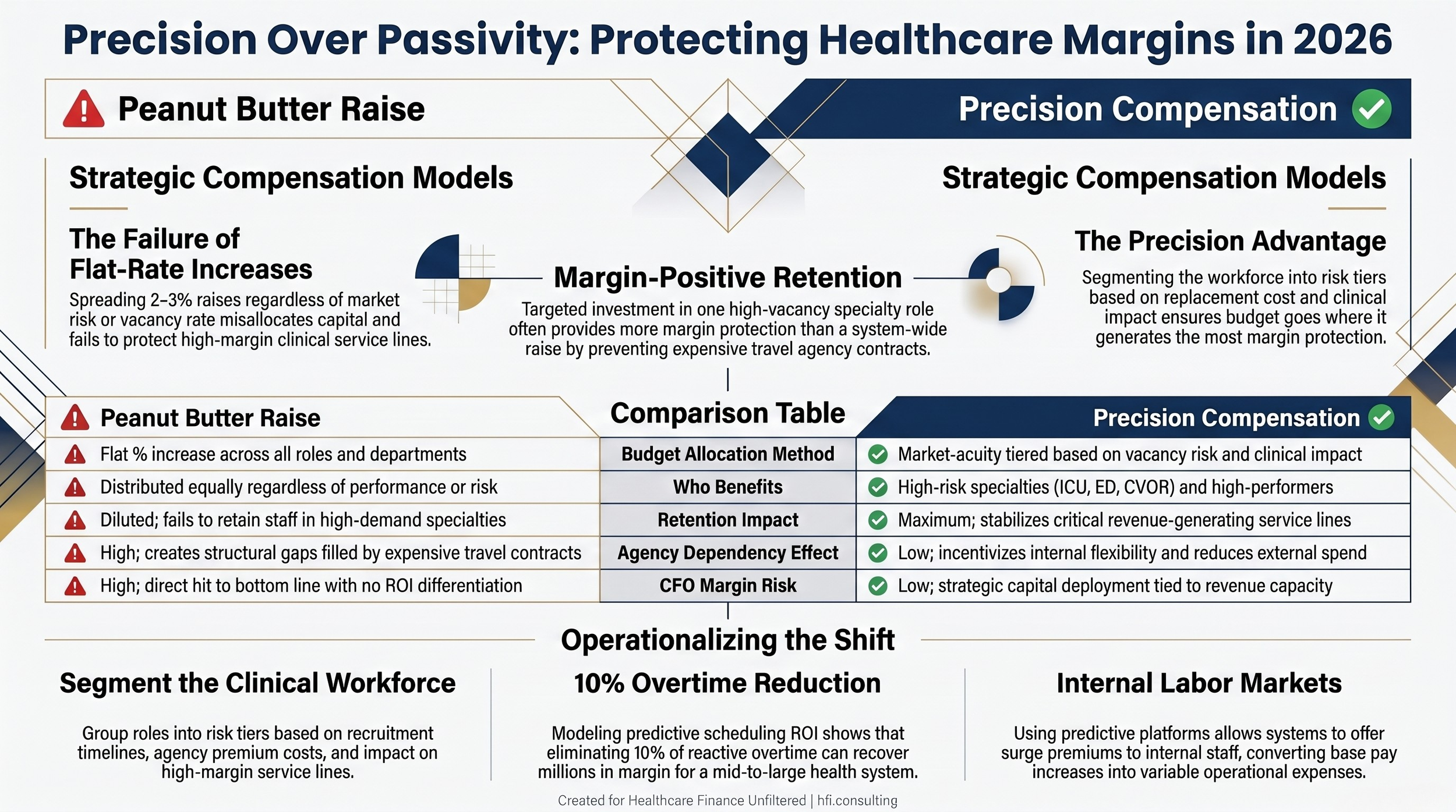
Comparison table contrasting peanut butter raises with precision compensation across five dimensions including retention impact and margin risk.
From Static HPPD to Predictive Workforce Orchestration
The technology gap between how most hospitals still manage labor and what the current platform ecosystem now offers is significant. Most finance leaders I encounter are working with retrospective reporting. The unit had 28 patients last night. The HPPD target was X. The variance was Y. The correction conversation happens the next morning, after the overtime is already on the books.
Modern predictive platforms integrate directly with the EMR and the Admission, Discharge, Transfer data stream to forecast what is called patient churn. That is the velocity of patient movement, not just the headcount at midnight.
Systems like UKG Pro Workforce Management with clinical scheduling extensions and QGenda are embedding this logic at the enterprise level. Instead of a flat census number, the algorithm analyzes historical discharge patterns, current physician rounding times, and OR schedules. It predicts that while a Med-Surg unit has 28 patients now, six will discharge by 2:00 PM and four admissions are coming from the PACU. A productivity manager sees a forecasted surplus or deficit 12 to 24 hours in advance. That means canceling a float nurse before she drives to the hospital rather than paying three hours of reporting time when you send her home at shift start.
The second major shift is dynamic acuity integration. Legacy HPPD treats every patient in a unit identically. A patient ready for discharge and a fresh post-op patient with continuous blood transfusions both count as 1.0 in the old model. Advanced clinical intelligence engines embedded within Epic Cogito or Oracle Health pull clinical parameters directly from nursing flowsheet documentation: IV medication count, wound care frequency, fall risk, and cognitive status. These translate into a dynamic workload intensity score that tells the finance team the true staffing requirement for that shift, not the assumed one.
For a deeper look at how technology platforms are reshaping financial operations across the revenue cycle, see AI-Powered Revenue Leakage Prevention: The CFO's Implementation Guide.
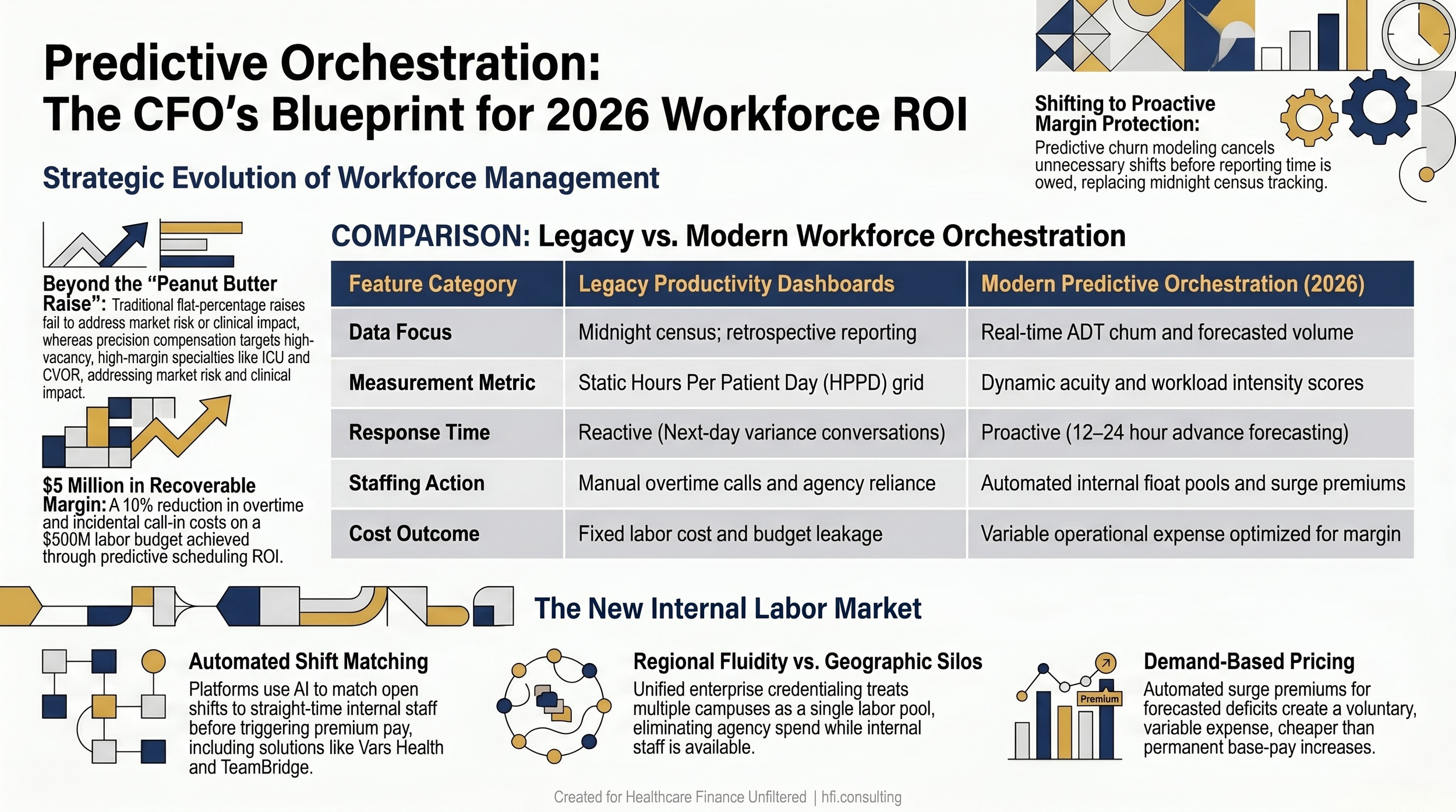
Comparison table showing legacy productivity dashboard capabilities versus modern predictive workforce orchestration across five operational dimensions.
Building an Internal Labor Market to Replace Agency Dependency
The travel nurse crisis of 2022 and 2023 burned through operating reserves at health systems that had no internal flexibility mechanism. The ones that weathered it best had already built enterprise-wide internal float pools capable of moving staff across facilities before calling an external agency.
Platforms like Vars Health and TeamBridge are turning hospital systems into internal per diem marketplaces. When the predictive platform identifies a deficit, it posts the open shift automatically to a mobile app visible to staff across the regional market. AI matching logic scores available employees against orientation history, competencies, and current overtime threshold. The system offers the shift to a straight-time internal float nurse first, then escalates to a part-time employee, then activates premium incentive pay only when a defined threshold is crossed.
What this does for the CFO is convert a fixed labor cost into a variable operational expense that only triggers when the revenue-generating capacity of the service line actually requires it.
In my work across the Ascension Florida and Alabama footprint, one of the most expensive inefficiencies was geographic silos. A hospital in Jacksonville might be paying heavy contract labor while a campus 20 miles away had nurses on low-census standby. Cross-facility regional float optimization solves this directly. Unified enterprise credentialing combined with predictive volume analytics lets regional finance leaders treat the entire market as a single fluid labor pool rather than a collection of competing cost centers.
If your team is still managing productivity from a static HPPD grid and a weekly variance report, the gap between your current approach and what leading systems are deploying is widening every quarter. For a deeper look at how to structure a precision compensation and workforce orchestration strategy tailored to your system, visit hfi.consulting.
Precision Compensation: Where the Budget Actually Goes to Work
Moving from peanut butter raises to precision compensation requires three things: market data at the role level, clinical acuity data at the unit level, and the organizational will to have different conversations with different department heads.
The mechanics are not complicated. Start by segmenting your clinical workforce into risk tiers based on market replacement cost and vacancy impact. Specialty areas like ICU, ED, PACU, and CVOR carry the highest risk. They have the longest recruitment timelines, the highest agency premium when they go vacant, and the most direct impact on high-margin service line revenue. These positions warrant the largest market-acuity adjustments in any given budget cycle.
Second, explore variable compensation structures tied to predictive demand data. When the workforce platform forecasts a critical deficit 48 hours in advance, it can apply an automated surge premium to that specific shift. Staff who want the earning opportunity opt in voluntarily. This converts what would have been a permanent base pay increase into a variable expense that activates only when the organization needs the coverage. Structured correctly, it is the financial equivalent of demand pricing applied to your own internal labor market.
Third, build cross-training into the clinical ladder structure rather than the tenure-based step model. A Med-Surg nurse cross-trained to PCU level care is worth more to the productivity model than two nurses trained at a single acuity level. She floats fluidly when the demand signal shifts. You pay more per person and carry fewer total FTEs. The per-person premium is almost always cheaper than the cumulative cost of the additional headcount and the scheduling rigidity it creates.
Several systems are already executing this well. Saint Francis Health System moved to a true merit-based compensation model in 2025, requiring managers to differentiate meaningfully based on performance rather than applying uniform increases. At Meritus Health, leadership intentionally recognizes approximately 20% of employees as consistent high performers and channels expanded leadership opportunities, specialized development programs, and financial differentiation to that group.
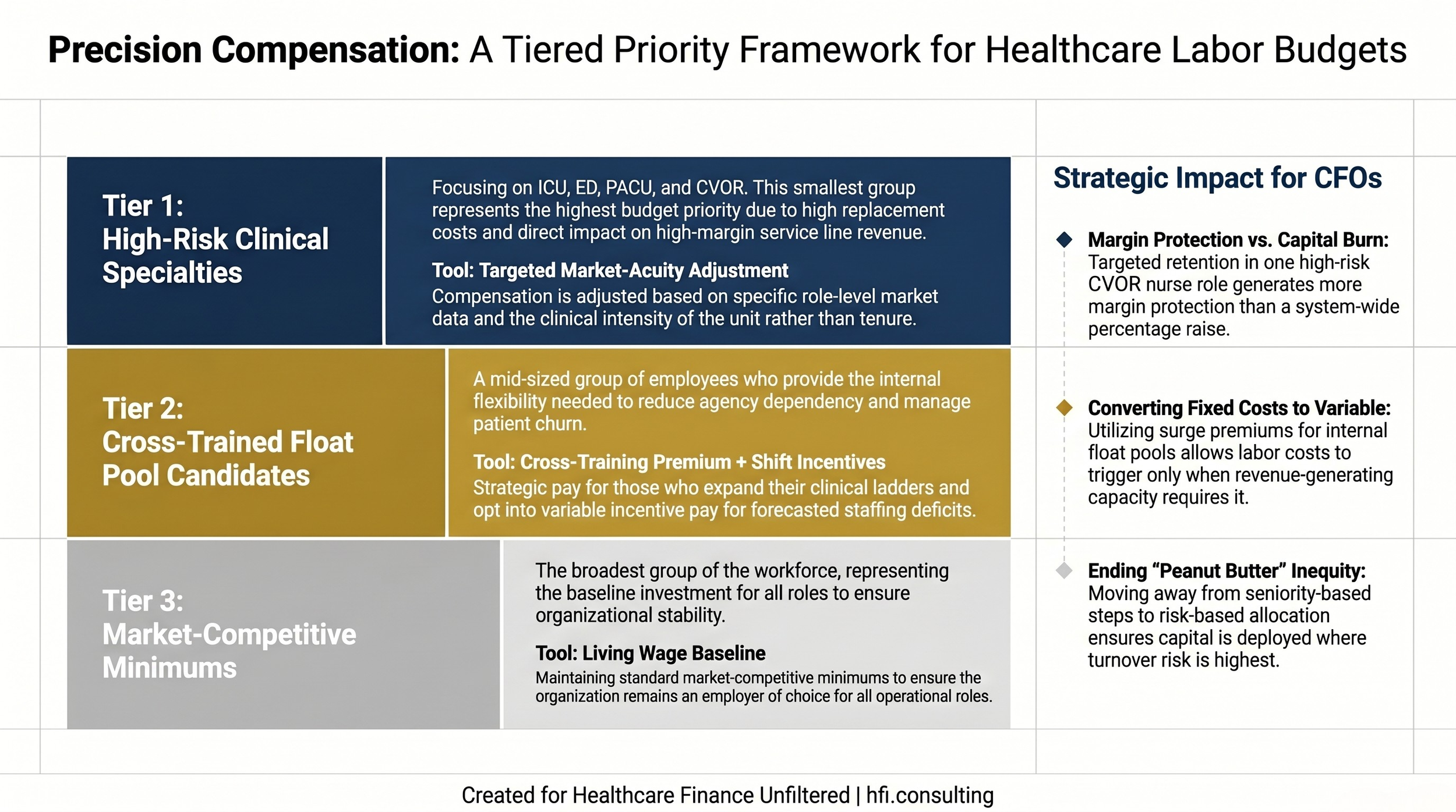
Three-tier compensation priority framework showing how health systems should allocate their labor budget across high-risk specialties, cross-trained float pool staff, and market baseline roles.
The CFO and CNO Alignment Requirement
None of this works without a different kind of conversation between finance and nursing leadership. Precision compensation requires data transparency. It means explaining to the CNO why the ICU is receiving a larger budget allocation than the ambulatory care center this cycle, and why that is strategic capital deployment rather than inequitable treatment.
The systems struggling most are the ones still using tenure-based step programs as their primary compensation mechanism. Seniority is a proxy for experience, not a measure of clinical impact or market risk. A five-year CVOR tech in a high-vacancy specialty carries significantly more retention risk than a ten-year outpatient registration coordinator in a stable, easily recruitable role. The compensation model needs to reflect that distinction explicitly and consistently.
The alignment challenge is real, but the data now exists to support the conversation. Vacancy rates by specialty, market replacement costs, agency premium by unit, and predicted churn by service line are all available in the platforms discussed above. Finance leaders who bring that data to the CNO conversation replace a values debate with an operational one.
What to Model Before Your Next Budget Cycle
Three scenario analyses are worth building before you finalize your next workforce budget.
First, run a vacancy cost model for your five highest-risk clinical specialties. Calculate the full cost of each vacancy: recruitment, onboarding, lost throughput, and agency premium. Then compare that to the cost of a targeted market adjustment that closes the gap between your current pay scale and the competitive market rate for that role.
Second, build a travel agency displacement model. Identify what percentage of your current agency spend is going to roles that a premium internal float pool could fill. The math almost always favors the internal investment at any system size above 200 beds.
Third, model the productivity platform ROI directly. If predictive scheduling eliminates 10% of your overtime and incidental call-in costs on a labor budget of $500 million, that is $5 million in recoverable margin before the platform cost is even factored in. The number is typically large enough to justify the technology investment with significant margin remaining.
Ready to build those scenario models for your system? The workforce cost and precision compensation framework is something I work through directly with finance leadership teams. Connect with me at hfi.consulting to start the conversation.
The Bottom Line
Labor is not going to get cheaper. The union contracts being ratified right now, some with increases exceeding 20% over three years, will set the market benchmark for non-union systems as well. Health systems that continue spreading raises thinly across the entire workforce while relying on agency labor to fill structural gaps are going to face the steepest margin pressure.
The CFOs protecting their margins are doing something different. They are moving the compensation budget to where the retention risk is highest. They are deploying predictive platforms to eliminate the reactive overtime cycle that HPPD spreadsheets cannot prevent. They are building internal labor markets that compete with travel agencies on flexibility rather than trying to match their base wage rates.
The tools are available. The data already exists inside your EMR. The opportunity is there for any finance leader willing to have the harder internal conversations that precision compensation requires.
P.S. If your health system has moved away from flat-rate raises toward a more targeted compensation model, what was the biggest internal obstacle you had to overcome? Hit reply and tell me.