
Hospital Service Line Closures — CFO Financial Framework
When Medicaid cuts, ACA dropout, and CMS outpatient migration collide, the closure math becomes inescapable.
Since January 1, 2026, 34 hospitals have closed departments or ended services, according to Becker's Hospital Review. Labor and delivery accounts for the largest single category. Behavioral health, burn units, pediatric rehabilitation, emergency departments, and skilled nursing are on the list too.
None of these decisions were made because the clinical need disappeared. They were made because the financial model broke.
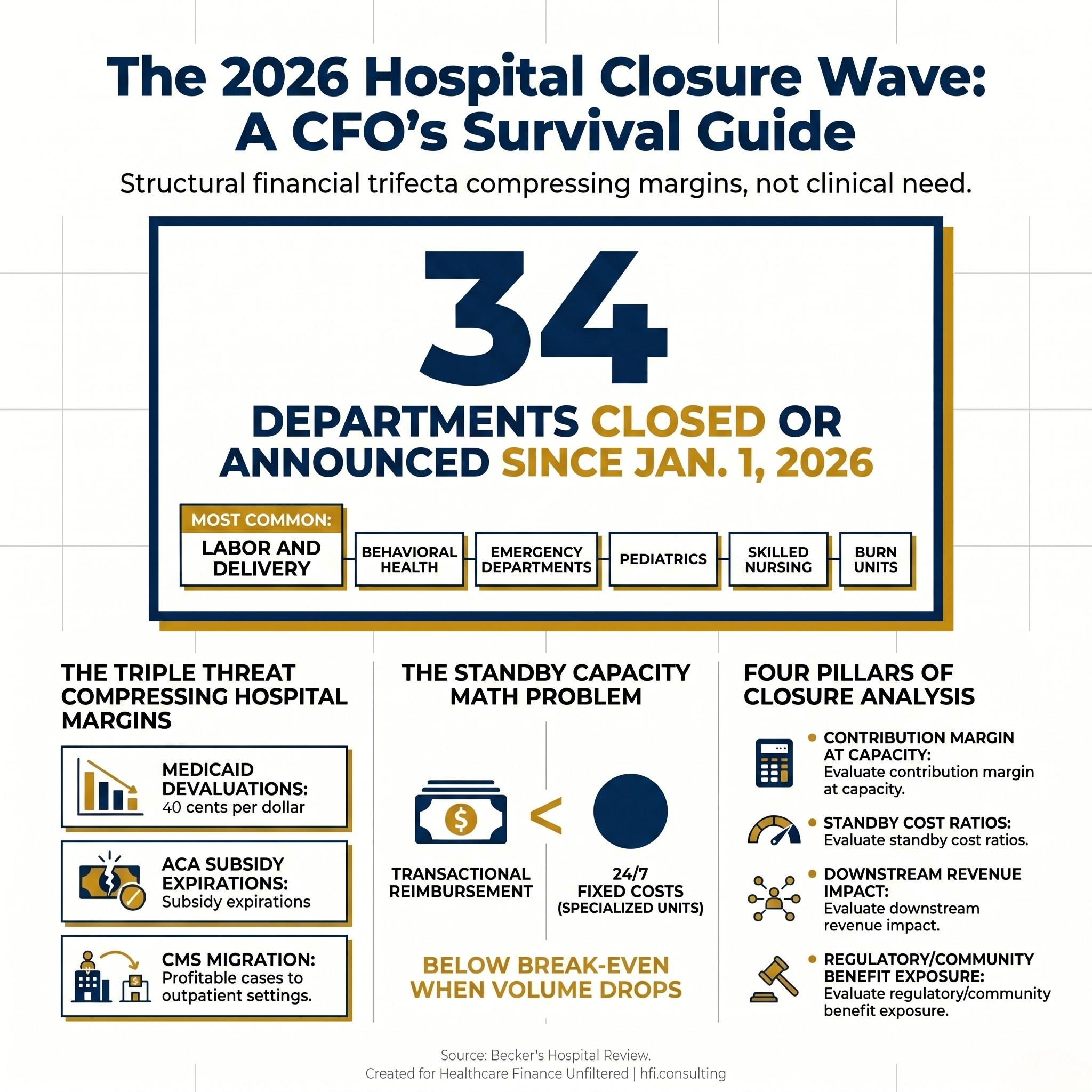
Infographic showing 34 hospital department closures in 2026 with labor and delivery as the most frequently closed service type, followed by behavioral health and emergency departments.
When a department closure announcement is released, the stated rationale almost always includes the same three phrases: declining birth rates, persistent workforce challenges, reimbursement that does not cover the cost of care. Those are real. But they are symptoms. The underlying diagnosis is a reimbursement structure that no longer supports specialized, low-volume, high-fixed-cost departments in the operating environment that hospitals are managing right now.
Understanding why this is happening simultaneously across 34 organizations matters for every CFO who needs to decide which service lines to defend, which to restructure, and which to exit before the board asks the question reactively.
The Three Forces Behind Every Closure
The Becker's list did not emerge from one problem. It emerged from three overlapping financial pressures compressing at the same time.
Medicaid Reimbursement Is Falling at the Worst Possible Moment
The reconciliation legislation passed earlier this year introduced work-documentation requirements for nondisabled, working-age Medicaid beneficiaries. Millions of enrollees are being disenrolled as a result. For hospitals, that does not mean fewer patients. It means more uninsured patients arriving through the emergency department at higher acuity and later in their care episode.
Analytical estimates suggest the effective value of every Medicaid dollar a hospital receives has been reduced by roughly 21 cents under the new framework. For a facility already operating at a negative or break-even margin, a 15% to 30% reduction in effective Medicaid reimbursement is not a budget variance. It is an existential threat to any low-margin, high-fixed-cost department.
The ACA Subsidy Cliff Is Converting Covered Patients Into Self-Pay
The enhanced premium tax credits that stabilized the ACA marketplace expired on December 31, 2025. For millions of enrollees, net premiums more than doubled. More than 21% of people who enrolled during the recent open enrollment period dropped their coverage or were disenrolled after failing to pay the first month's premium.
Those patients do not stop needing care. They arrive at the emergency department uninsured. They become uncompensated care volume. And they drain the cash reserves hospitals use to internally subsidize money-losing specialty departments. The full downstream dynamics of that coverage shift are detailed in the earlier piece on ACA Subsidy Expiration Is Reshaping Your Community Benefit Strategy. The community benefit implications were significant then. The service line implications are now impossible to ignore.
CMS Is Migrating the Revenue That Subsidized Everything Else
CMS finalized a roadmap to fully eliminate the Inpatient Only list by 2028, removing 285 procedures for CY 2026 alone. Profitable orthopedic and cardiovascular cases that historically required an inpatient setting can now be routed to ambulatory surgical centers. The site-neutral payment policy expansion continues to cap off-campus provider-based department reimbursement at 40% of the OPPS rate for certain services.
The practical result: the high-margin surgical volume that cross-subsidized money-losing departments is migrating to lower-cost settings. The internal transfer payment that made keeping a labor and delivery unit or an inpatient behavioral health unit financially viable has been progressively eliminated by policy.
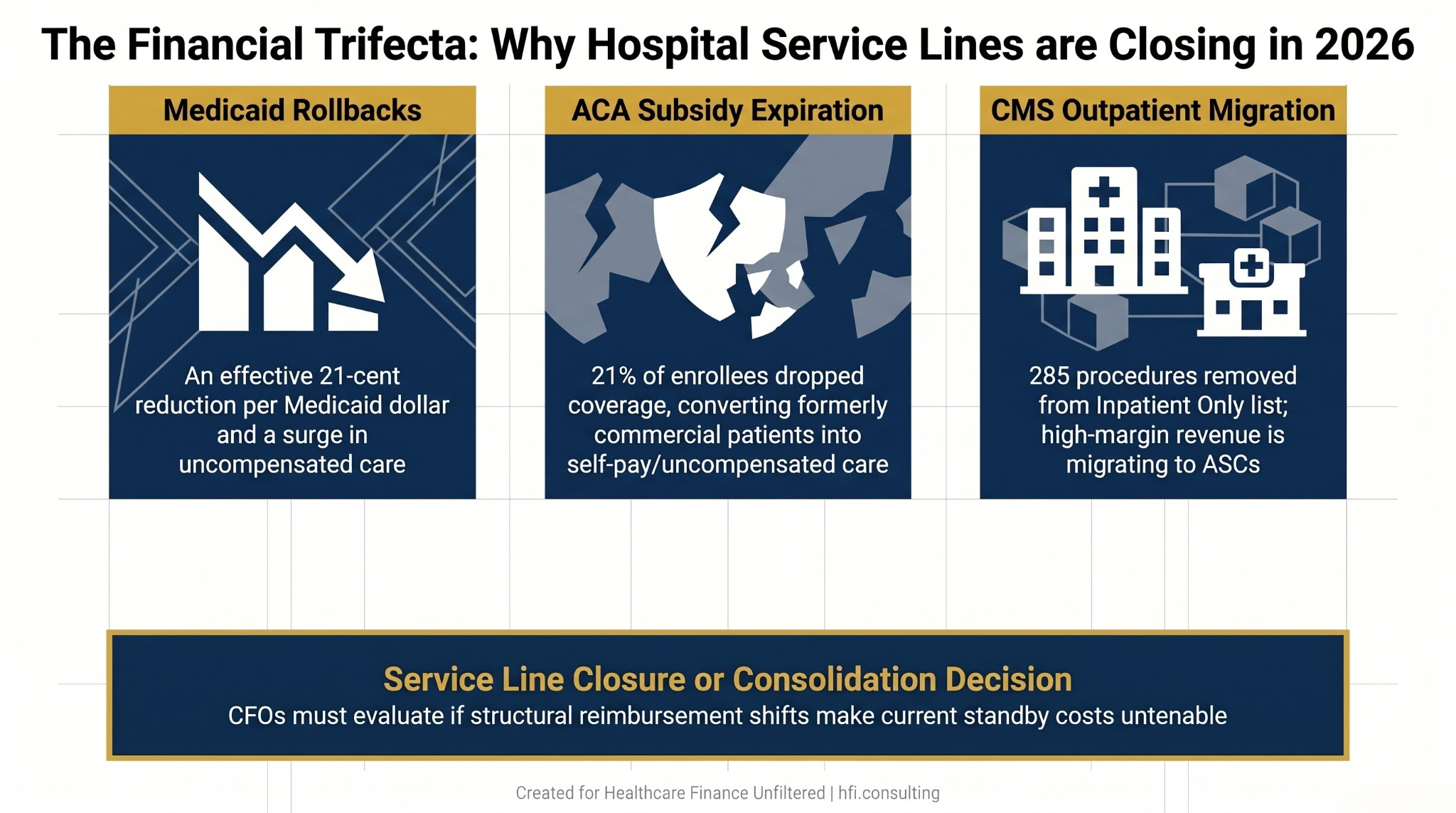
Framework diagram showing three simultaneous financial forces driving hospital service line closures in 2026: Medicaid rollbacks, ACA subsidy expiration, and CMS outpatient migration policy changes.
The Standby Capacity Problem Nobody Talks About
Every service line on the Becker's list shares one structural feature: standby cost.
A labor and delivery unit requires 24/7 specialized staffing coverage whether there are three births that day or zero. An ICU requires intensivist coverage regardless of census. A burn unit requires licensed staff around the clock regardless of how many patients are in the beds. A behavioral health unit requires trained clinical personnel on shift whether the census is full or half-empty.
Current reimbursement frameworks are purely transactional. The hospital gets paid per birth, per case, per procedure. There is no standard mechanism to compensate for the fixed standby cost required to keep a specialized unit safe when volume is insufficient.
When volume is high enough, per-encounter reimbursement covers the fixed standby cost and generates margin. When volume drops below the break-even threshold, the fixed cost becomes an ongoing cash drain with no revenue offset. Ouachita County Medical Center's CEO said it plainly when they closed their labor and delivery unit in January: "We do so few deliveries, and with the cut in reimbursement, it's just not feasible." That is not a strategic failure. That is a math problem that reimbursement policy has not solved.
Labor and Delivery as the Leading Indicator
Of the 34 closures in the Becker's list, labor and delivery accounts for the largest single category. Rochester Regional Health, Baptist Health Fort Smith, Mon Health Stonewall Jackson, MercyOne Clinton, Johnson Memorial Health, Warren General Hospital, Sweetwater Hospital Association, Ouachita County Medical Center, and Southeast Iowa Regional Medical Center have all closed or announced closure of obstetric services this year.
The common thread across every announcement: declining birth rates, specialized workforce shortages, and reimbursement that does not cover the cost of maintaining safe staffing ratios. These are not geographically isolated decisions. The closures span New York, Arkansas, West Virginia, Iowa, Indiana, Pennsylvania, Tennessee, and communities across the rural South, Midwest, and Northeast.
The hub-and-spoke consolidation model is emerging as the most common strategic response among larger health systems. Great River Health in Iowa is transitioning to a model that consolidates labor and delivery at a central site while maintaining pre- and postnatal services locally in outpatient settings. Merrimack Health in Massachusetts is consolidating maternity and neonatal services from Methuen to Lawrence.
That model is not available to standalone rural hospitals. For those facilities, the choice is between continuing to operate a money-losing unit or closing it and leaving the community without local obstetric access. The rural dimension of this problem is addressed in detail in Rural Hospitals Already in the Red: How Medicaid Changes Will Push Them to the Brink.
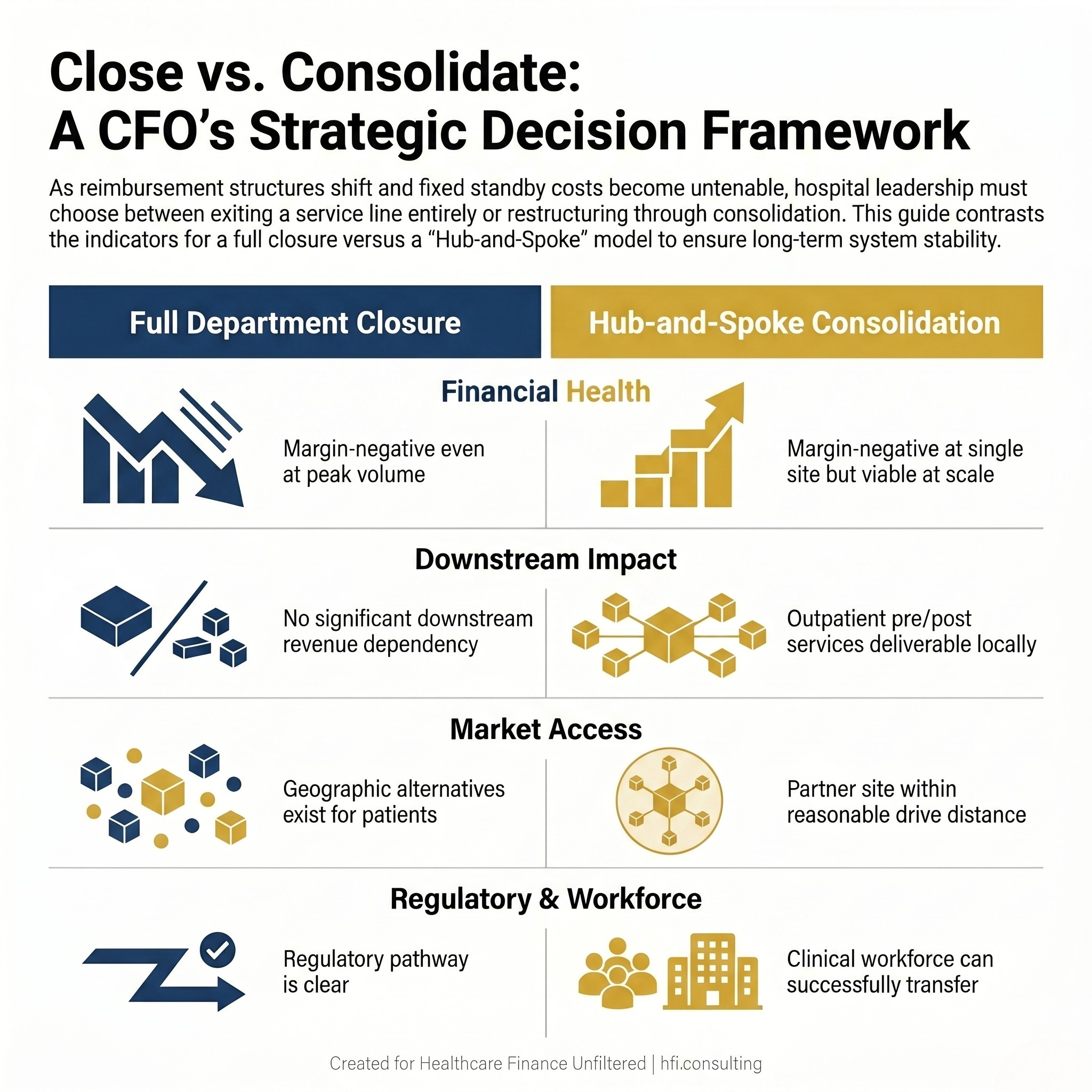
Decision comparison table for hospital CFOs showing when full department closure versus hub-and-spoke service consolidation is the appropriate strategic response to service line margin decline.
The CFO Decision Framework
Service line decisions at this level are rarely presented to the CFO as a clean binary choice. They arrive as a series of escalating signals: one quarter of negative margin, then another, then an unexpected staffing vacancy that triggers an agency contract at premium cost, then a board conversation about whether to continue.
The framework that holds up under scrutiny requires four questions answered before any board presentation.
What is the contribution margin at full operational capacity versus current volume?
If the service line is margin-negative at current volume but margin-positive at historically achievable volume, the problem may be cyclical. If it is margin-negative even at peak historical volume, the problem is structural and no amount of operational improvement closes the gap.
What is the standby cost as a percentage of total operating cost?
Departments with high standby cost ratios are the most vulnerable to volume deterioration. Labor and delivery, ICUs, burn units, and inpatient behavioral health all carry standby cost structures that make low-volume operations financially untenable regardless of operational efficiency.
What happens to downstream revenue if this service line closes?
Labor and delivery is a loss leader in many health systems because obstetric patients become long-term primary care, specialist, and pediatric patients within the same system. Closing the unit may improve the unit-level margin while degrading the system-level revenue picture over a three-to-five-year horizon. That downstream modeling must happen before the closure decision is final, not after the announcement is made.
What is the community benefit and regulatory exposure?
For nonprofit systems, closing a service that disproportionately serves Medicaid and uninsured populations carries Schedule H implications and potential state regulatory review. New York's Department of Health approval is explicitly required for the Rochester Regional Health closure. That is not a formality that can be managed after the fact.
In my consulting work with health systems navigating service line decisions, the downstream revenue modeling and the community benefit analysis are the two pieces most often skipped when a closure case is being built quickly. Both can materially change the decision. If your team is working through a service line review and needs a structured contribution margin and downstream impact model, that is exactly the work we do at HFI Consulting. The framework matters before the announcement. Reach out at hfi.consulting.
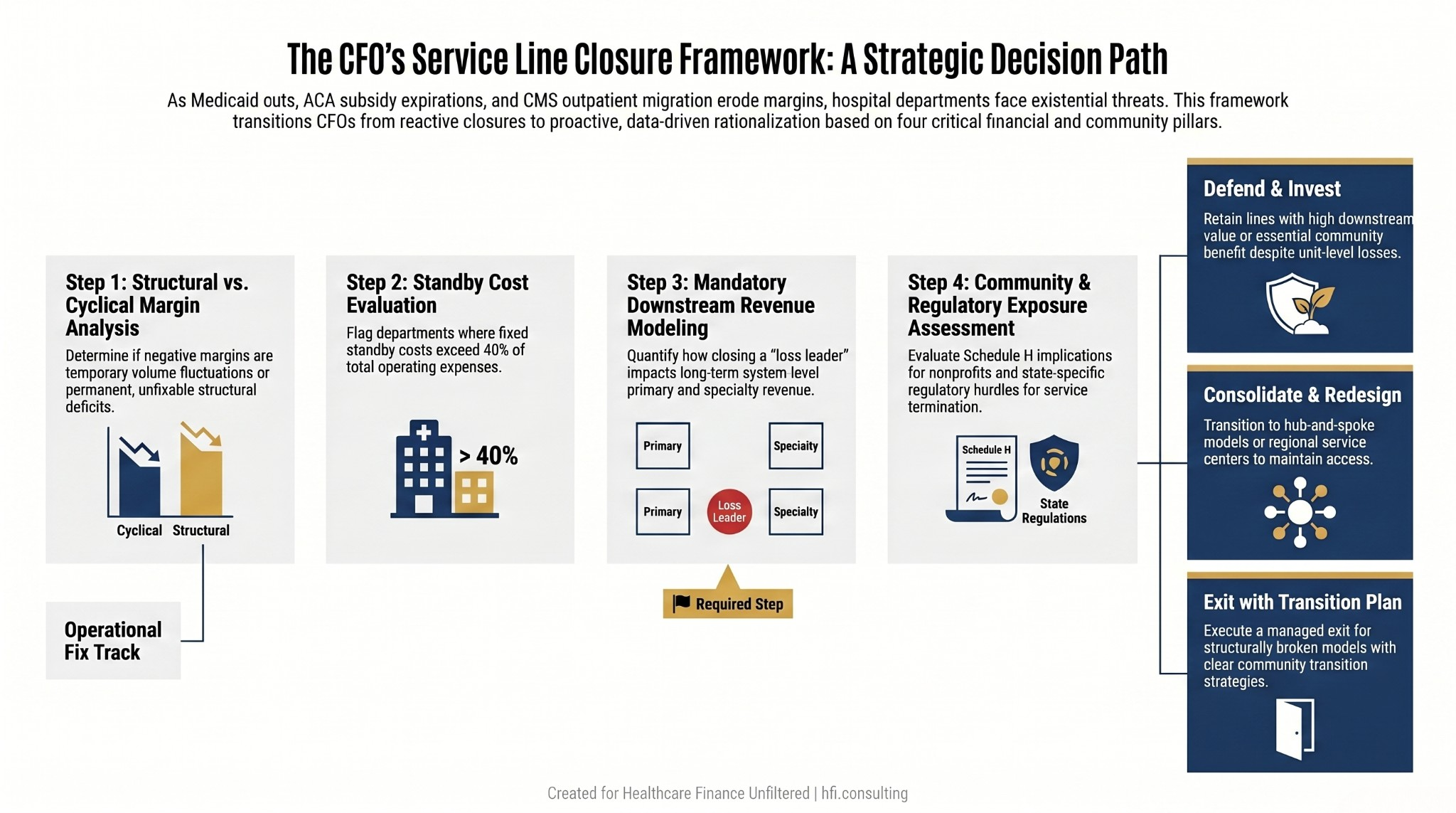
Hospital service line decision flowchart for CFOs with four decision nodes covering contribution margin, standby cost, downstream revenue, and community benefit regulatory exposure, leading to defend, consolidate, or exit recommendations.
What the Closures Signal for Portfolio Strategy
The Becker's list is not a random sample of struggling rural hospitals. Vandalia Health, Providence, Kaleida Health, LifeBridge Health, and Integris Health are all on the list. When organizations of that scale are closing departments, the pressure is systemic, not situational.
The financial model for certain inpatient service lines has changed structurally. The CFOs who recognize that shift now will make better capital allocation decisions than those who wait for the next budget cycle to confirm what the data already shows.
Portfolio rationalization at the multi-hospital level is no longer an academic exercise. As covered in the earlier piece on Health System Portfolio Rationalization: The CFO's Framework for Growing Up Instead of Out, the question is not whether rationalization is necessary. The question is whether it happens proactively with a documented framework or reactively in response to a financial crisis that eliminates the strategic options.
The CFOs who approach these decisions with updated volume projections under the new Medicaid and ACA coverage environment, a clear standby cost analysis, and a documented downstream impact model will make decisions they can defend to the board and to their communities. The ones who close departments reactively, without that analysis, will face board scrutiny and community backlash simultaneously.
The math is driving the decisions. The framework is what determines whether the decision is strategic or just desperate.
If your service line modeling does not yet reflect the post-OBBB Medicaid enrollment projections or the ACA marketplace dropout rate for your specific market, that analysis is overdue. HFI Consulting builds those models. Start at hfi.consulting.
P.S. Which service line in your organization is showing the earliest warning signs right now? Hit reply and tell me. The patterns across organizations are worth a follow-up piece, and I read every response.