
The $1 Billion Medicare Fraud Playbook: What the HealthSplash Conviction Means for Healthcare CFOs
Federal jury convicts HealthSplash CEO for $1B Medicare fraud. Here's the CFO compliance framework to stop it at your organization.
A federal jury in the Southern District of Florida just convicted Brett Blackman, founder and CEO of HealthSplash, on multiple counts of healthcare fraud, wire fraud, and conspiracy to pay and receive illegal kickbacks. The scheme billed Medicare and other federal programs more than $1 billion for medically unnecessary durable medical equipment. Taxpayers absorbed more than $450 million in actual payments before investigators shut it down.
This was not a billing error. It was an engineered fraud machine built on software acquisition, foreign telemarketing, corrupt telemedicine networks, and shell companies designed to outpace automated CMS audits.
The finance leadership question is not whether your organization would knowingly participate in something like this. The question is whether your current controls would catch it if elements of this scheme crossed into your vendor network, your affiliated providers, or your digital health partnerships.
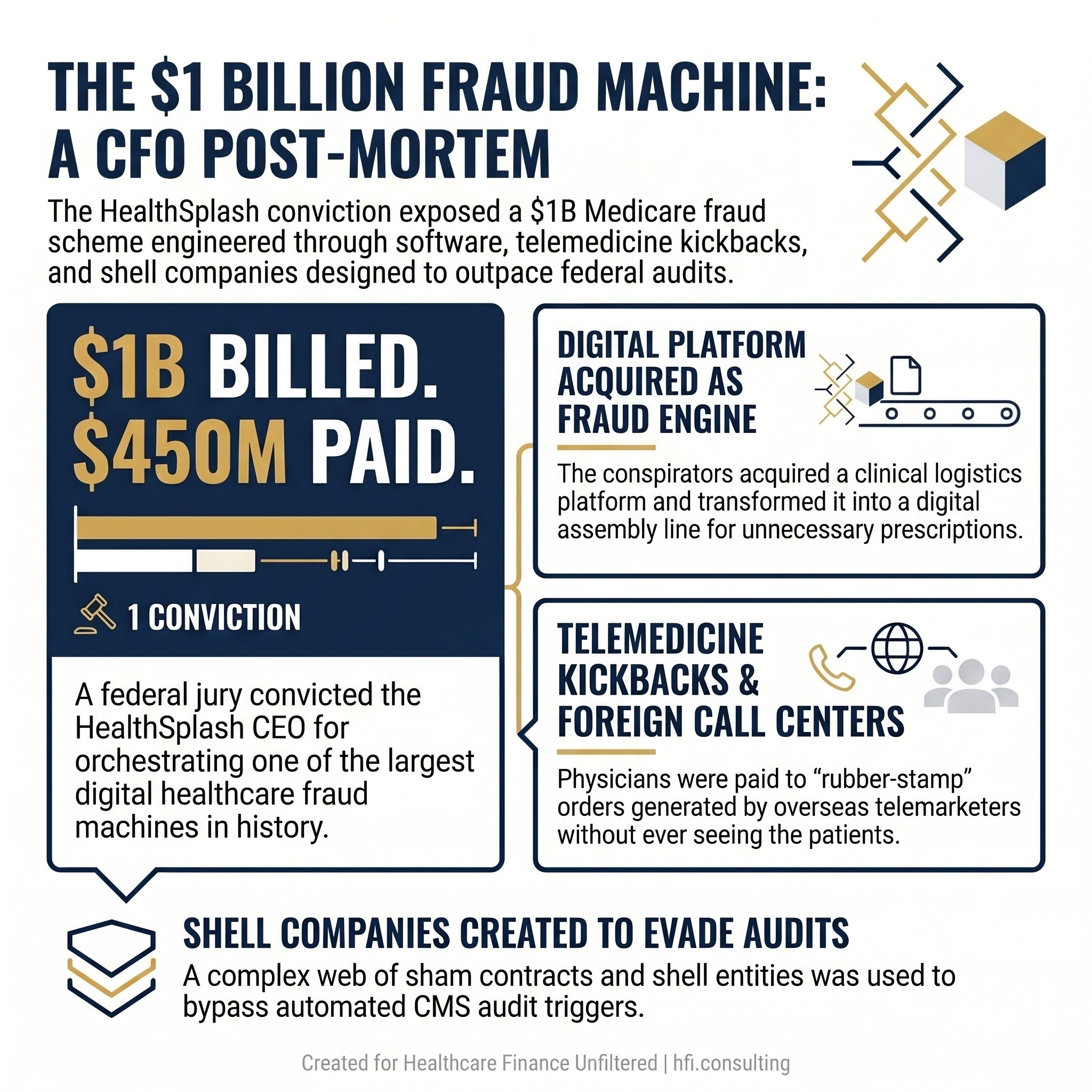
Infographic showing HealthSplash Medicare fraud conviction key stats: $1B billed, $450M collected, scheme built on software, telemedicine kickbacks, and shell companies.
How the HealthSplash Machine Actually Worked
In 2017, HealthSplash acquired an internet-based platform called Power Mobility Doctor Rx, LLC, known as DMERx. The platform was designed to connect physicians, DME suppliers, and pharmacies. Blackman and his co-conspirators turned it into a digital assembly line for fraudulent prescriptions.
Foreign call centers and spam mail campaigns targeted hundreds of thousands of Medicare beneficiaries, pressuring elderly patients to accept orthotic braces and other equipment they did not need. Telemedicine doctors were paid kickbacks disguised as consultation fees to sign pre-populated prescription orders without meaningfully examining patients. In documented cases, the physicians signed orders without speaking to the patient at all.
To stay under the radar of CMS automated audit systems, the conspirators built a web of shell companies, sham marketing contracts, and manipulated digital medical records. Suppliers and pharmacies billed more than $1 billion and collected more than $450 million before the Southern District of Florida prosecution dismantled the network. Blackman is scheduled for sentencing on August 26, 2026, and faces up to 20 years in prison.
Why This Is a CFO Risk Conversation, Not Just a Compliance Story
The HealthSplash architecture exploited three specific vulnerabilities that live in the CFO's portfolio: vendor due diligence gaps, EHR and billing system monitoring blind spots, and contract structures that transferred fraud risk to the organization without its knowledge.
If your compliance team is the primary line of defense on digital health vendor risk, that is already a structural problem. The CFO controls the capital allocation, the vendor contract terms, and the analytics infrastructure. That makes fraud prevention a finance function.
CMS's own enforcement posture has made this point clearly. The CRUSH initiative, the WISeR Model, and the sustained DOJ healthcare fraud strike force presence in South Florida all signal that federal investigators are deploying the same predictive analytics tools your finance team should already be running internally. If CMS finds an anomaly in your data before your internal audit does, you have already lost the ability to manage the situation on your own terms.
For a deeper look at how CMS is deploying data analytics in fraud detection, the earlier piece on CMS Medicaid Fraud Crackdown 2026 lays out the enforcement signal every finance leader needs to understand.
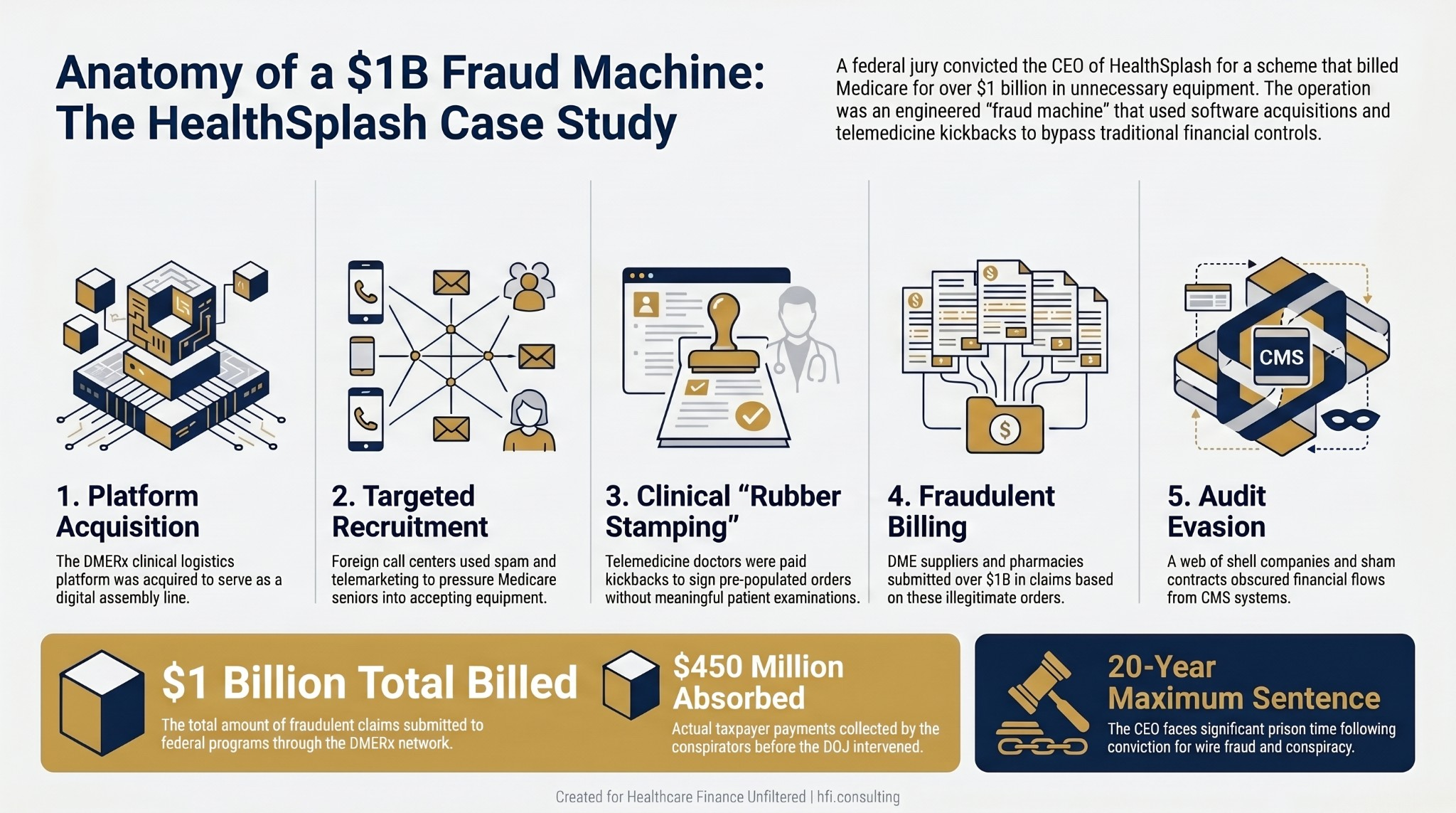
Five-step process flow showing how HealthSplash used software acquisition, call centers, telemedicine kickbacks, and shell companies to execute over $1 billion in Medicare fraud.
The Five-Point CFO Framework for Digital Fraud Prevention
1. Flag High-Risk Billing Categories at the System Level
Fraud schemes thrive on volume. The HealthSplash operation processed prescriptions for DME at a scale that should have triggered internal anomaly detection long before federal investigators arrived.
CFOs should require automated flags within EHR and billing systems for sudden spikes in DME orders, genetic testing billing, and topical compounding prescriptions, particularly when those orders correlate with specific digital platforms, telemedicine encounters, or out-of-state patient populations. A compliance freeze protocol tied to these triggers needs to exist before the volume becomes a pattern.
This is not about creating friction for legitimate clinical operations. It is about building the monitoring infrastructure that distinguishes between organic ordering trends and volume anomalies that signal something else is happening.
2. Apply Real Due Diligence to Platform and Vendor Acquisitions
The HealthSplash scheme was built on a software acquisition. DMERx was a legitimate-looking clinical logistics platform. The fraud was baked into how the platform was deployed, not into its stated function.
When your organization acquires, partners with, or integrates a third-party digital health tool, the financial and compliance due diligence cannot stop at the software's surface. Review the compensation structure of vendor contracts carefully. If payments are structured around transaction volume rather than service delivery, that is a red flag for Anti-Kickback Statute exposure.
Review who the actual end-users of the platform are and what data flows between the platform and your billing systems. The IT Governance Is Now a Finance Problem framework covers exactly this kind of third-party integration risk and why it belongs on the CFO's risk register.
3. Enforce Three-Way Matching on Telehealth Claims
The clinical failure in the HealthSplash scheme was straightforward: physicians signed orders without examining or even speaking with patients. The billing failure was that no internal mechanism existed to catch the gap between the order and the actual clinical encounter.
A rigorous three-way match protocol for telehealth and DME-linked claims requires three elements before a claim moves to submission. First, a verified time-stamped log of an actual physician-patient interaction. Second, a clinical progress note demonstrating individualized medical necessity. Third, the final order and claim matching the exact items and services documented.
If a platform or vendor cannot produce audited interaction logs that match the date of service, billing must stop. That is the operational standard, not a high bar.
4. Give Compliance Independent Authority Over Operations
One of the structural vulnerabilities that allows tech-enabled fraud to scale is a compliance function that reports through operational leadership rather than directly to the board. When a revenue-generating business line is controlled by the same executive chain that oversees compliance, the incentive structure works against early intervention.
The Chief Compliance Officer needs a direct board reporting line that bypasses the CEO and operational executives. If a high-margin billing stream is being pushed through a proprietary digital platform and the compliance team flags a concern, they need the structural authority to halt billing and initiate a forensic audit without facing retaliation.
This is a governance question before it is a compliance question. The CFO can influence this structure. Most do not, because the conversation is uncomfortable until a federal indictment makes it unavoidable.
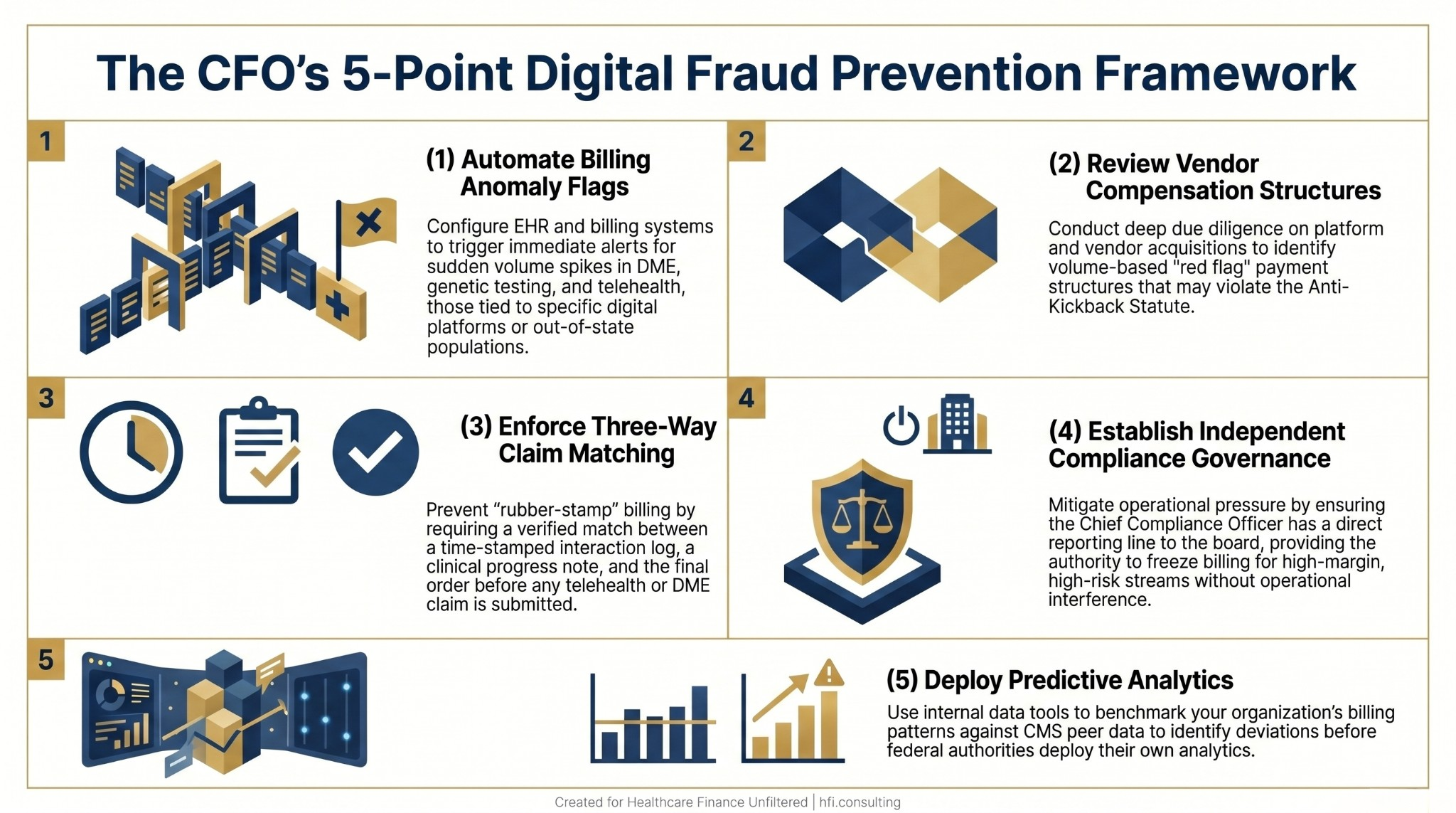
Five-point CFO framework for digital Medicare fraud prevention covering billing flags, vendor due diligence, claim matching, compliance governance, and predictive analytics.
If your organization partners with digital health vendors, telemedicine platforms, or third-party DME suppliers, the HealthSplash conviction is your compliance review trigger. The vendor due diligence and billing integrity framework at hfi.consulting is built for exactly this kind of platform risk assessment.
5. Deploy Predictive Analytics Before Federal Investigators Do
The same data signals federal investigators used to unravel the HealthSplash network are accessible to your finance team right now. Billing volume relative to documented patient activity. Service line cost patterns relative to peer benchmarks. Ordering patterns by affiliated provider. Supplier enrollment status.
Modern revenue cycle analytics platforms can benchmark internal provider billing behavior against national CMS peer averages in near real time. A sudden deviation from peer norms should trigger an internal review before a CMS audit request arrives. The AI-Powered Revenue Leakage Prevention piece covers how leading health systems are building exactly this kind of monitoring infrastructure.
The organizations that identified compliance exposure early in the current enforcement cycle had one thing in common: internal analytics running the same logic federal investigators use. The ones that did not know until the subpoena arrived had monitoring gaps that were entirely addressable.
The Whistleblower Option Is Already Built Into Federal Law
The HealthSplash prosecution was driven by federal investigators, but schemes this large rarely collapse without internal participants or observers who eventually talk. The False Claims Act whistleblower provisions create a direct financial incentive for employees and auditors who identify fraud and report it.
The Aetna $117.7M False Claims Act Settlement 2026 illustrates how internal coding auditors can become the source of qui tam actions that generate nine-figure liability. The structural lesson for CFOs is that your own billing and coding staff are always potential enforcement channels, for both legitimate concerns and, in a well-structured organization, for reporting problems they cannot escalate internally.
Building clear internal escalation paths for billing concerns is not soft HR policy. It is material risk management. If the only way for a coder or auditor to report a concern is to go to a supervisor who is also part of the problem, the external qui tam option becomes more likely.
What This Means for Payer CFOs Specifically
The HealthSplash scheme targeted Medicare beneficiaries and billed government programs. But the fraud infrastructure connected to private payer networks through the same telemedicine and DME supplier pipelines.
Payer finance leaders are positioned to identify anomalous billing patterns from affiliated DME suppliers and telemedicine networks that providers may never see. Claims volume analysis, provider ordering pattern benchmarking, and supplier credentialing verification are all payer-side tools. If your payer organization is not running these analytics on DME and telehealth billing at the supplier level, the HealthSplash case is the evidence that the risk is real.
CMS has made DMEPOS supplier revocation lists public, including National Provider Identifiers and reasons for revocation. Payer contracting and credentialing teams should be cross-referencing those lists against active supplier networks now.
The CFO's 30-Day Action List
The HealthSplash conviction landed last week. Here is the internal review it should trigger in the next 30 days.
Pull your DME, genetic testing, and telehealth billing volume for the past 12 months. Look for ordering concentration: are specific affiliated providers or telemedicine vendors generating a disproportionate share of these claims? Does the volume correlate with specific platforms or out-of-state patient populations?
Review your current telemedicine vendor and DME supplier contracts. Does the compensation structure include transaction-based or volume-based payments? Do your agreements include audit rights that would allow you to pull physician-patient interaction logs?
Verify that your compliance function has a documented direct board reporting line and a formal protocol for initiating a billing freeze without operational approval.
Run your active DME and pharmacy supplier list against the CMS DMEPOS revocation database.
Brief your board audit committee on the HealthSplash conviction and the digital fraud risk framework your organization has in place. If the answer is that no framework currently exists, that gap is itself the finding.
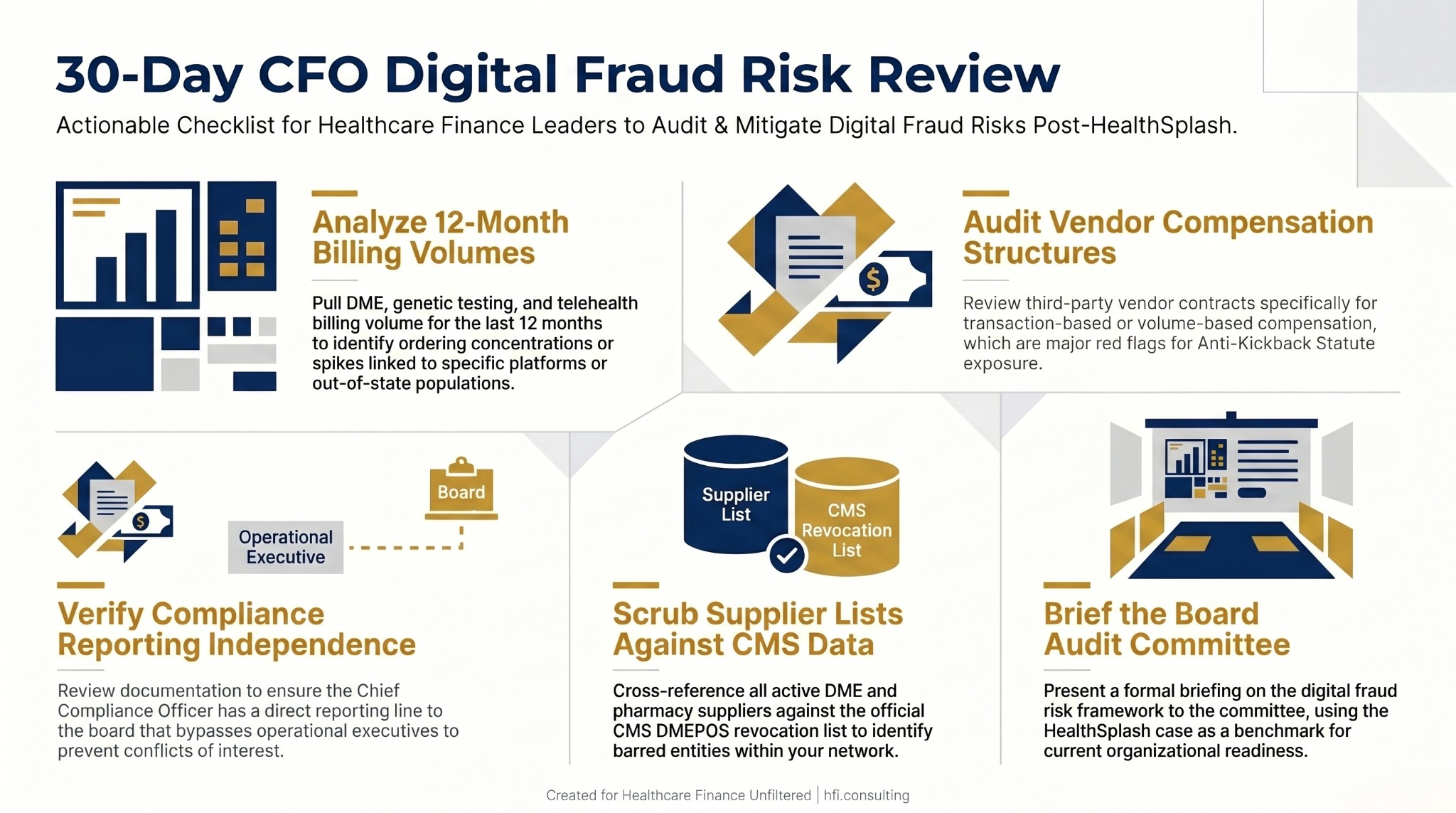
30-day CFO audit checklist for digital Medicare fraud risk covering billing volume review, vendor compensation structure, compliance governance, and CMS supplier verification.
The finance function owns the budget, the vendor contracts, and the analytics infrastructure. That makes digital fraud prevention a CFO responsibility before it becomes a federal enforcement one. If you are working through a platform vendor review or building out billing integrity monitoring, hfi.consulting is a resource for finance leaders navigating exactly this kind of compliance-adjacent operational work.
The HealthSplash case will become a standard reference in healthcare compliance training for years. The $1 billion figure is the headline. The operational mechanism is what finance leaders actually need to understand.
A software platform acquired for clinical logistics. A telemedicine network paid to rubber-stamp orders. A billing volume engineered to outpace automated audit systems. None of these elements required the CFO to be complicit. They only required the CFO to not be looking.
That is the part worth carrying into your next leadership meeting.
P.S. Does your organization currently run automated billing anomaly flags for DME, genetic testing, or telehealth ordering patterns tied to specific vendor platforms? Hit reply and tell me what your internal monitoring setup actually looks like. I am tracking what finance leaders are building in this space and it may become a follow-up piece.