
DSH Lawsuit 2026: Should Your Hospital Join 131 Plaintiffs or Stay on the Sidelines?
131 hospitals are suing HHS over billions in lost DSH payments. Here's the CFO framework for deciding where you stand.
A federal lawsuit filed this week names 131 hospitals as plaintiffs against HHS Secretary Robert F. Kennedy Jr., alleging that a two-decade-long manipulation of Disproportionate Share Hospital payment calculations has illegally withheld billions in funding from the facilities that need it most. The Court of Appeals has ruled against HHS three times. And the hospitals are still not being paid correctly.
For CFOs at safety-net and teaching hospitals, this is not a legal story. It is a balance sheet story.
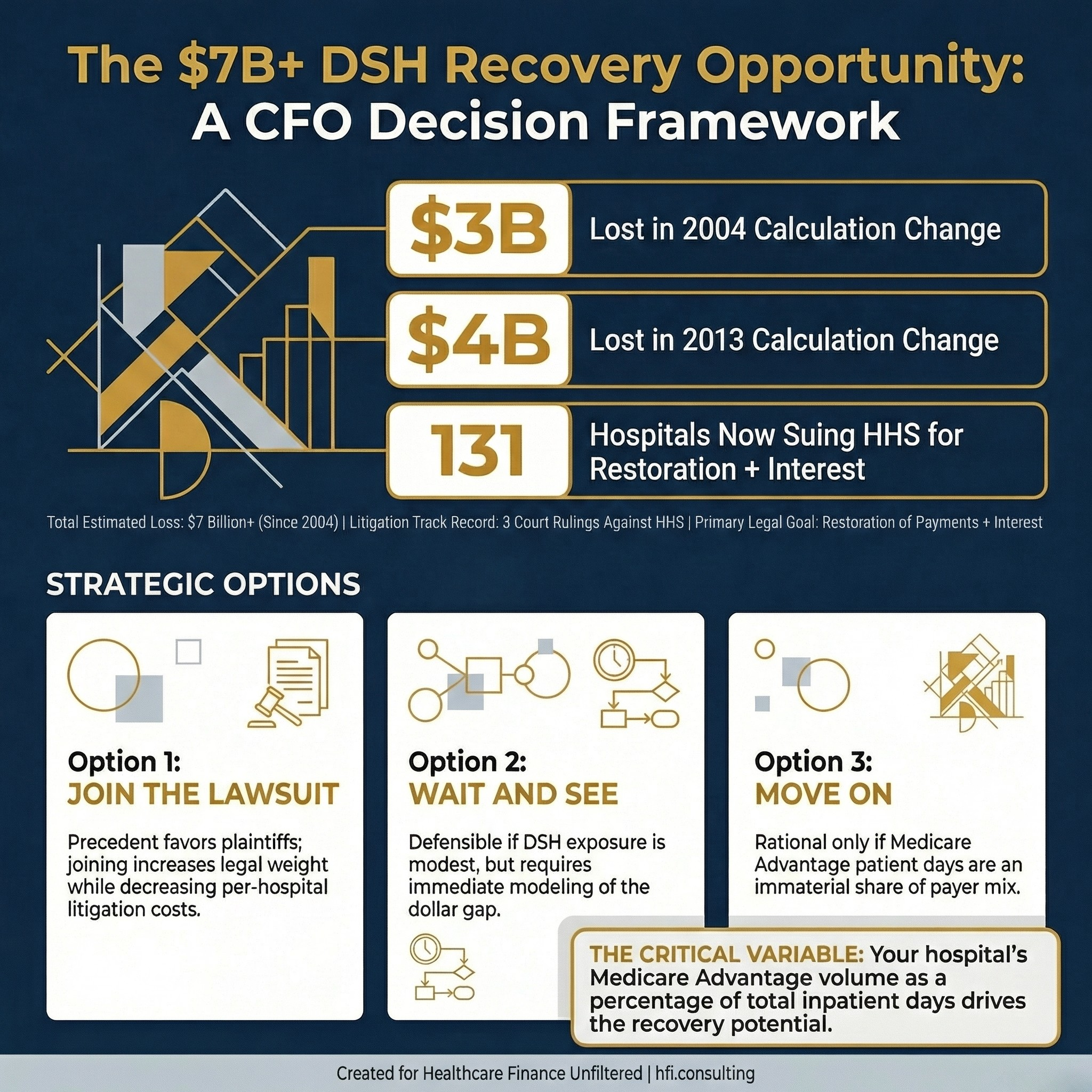
Infographic showing $3 billion lost in 2004, $4 billion lost in 2013, and 131 hospitals suing HHS in 2026 over DSH payment calculation changes
What DSH Payments Are and Why the Calculation Matters
Disproportionate Share Hospital payments exist for a specific reason: some hospitals treat a disproportionate share of low-income patients and incur costs that standard prospective payment rates do not cover. Congress designed DSH as a percentage adjustment applied on top of base DRG rates to account for that burden.
The calculation uses two fractions. The Medicare Part A/SSI fraction estimates low-income Medicare patients based on Supplemental Security Income enrollment. The Medicaid fraction counts Medicaid-eligible patient days in the numerator. Combined, these produce the disproportionate patient percentage that determines whether a hospital qualifies for DSH and how large the payment adjustment will be.
The dispute at the center of this lawsuit is about one question: how Medicare Advantage patients are counted in those fractions. HHS changed the methodology in 2004. Courts threw it out. HHS tried again in 2013. Courts ruled against the agency again. In 2023, HHS issued a final rule attempting to retroactively restore the 2004 methodology. That is the rule now being challenged by 131 hospitals, including facilities owned by HCA Healthcare.
A Two-Decade Pattern of Regulatory Overreach
This is not a new fight. It is a pattern.
The 2004 change shifted how Medicare Part C days were counted in the SSI fraction, effectively reducing the numerator that drives higher DSH payments. Courts later vacated that rule. The 2013 changes to SSI measurement cost hospitals another $4 billion. The 2023 rule was HHS attempting to lock in retroactively what the courts kept rejecting.
The plaintiff hospitals are asking the court to do three things: declare the 2023 rule invalid, restore the pre-2004 DSH calculation standard, and direct HHS to pay the additional amounts owed, plus interest. The Court of Appeals has already ruled against HHS three times in disputes arising from the same underlying calculation methodology.
That legal track record matters when you are building a CFO case for joining this litigation.
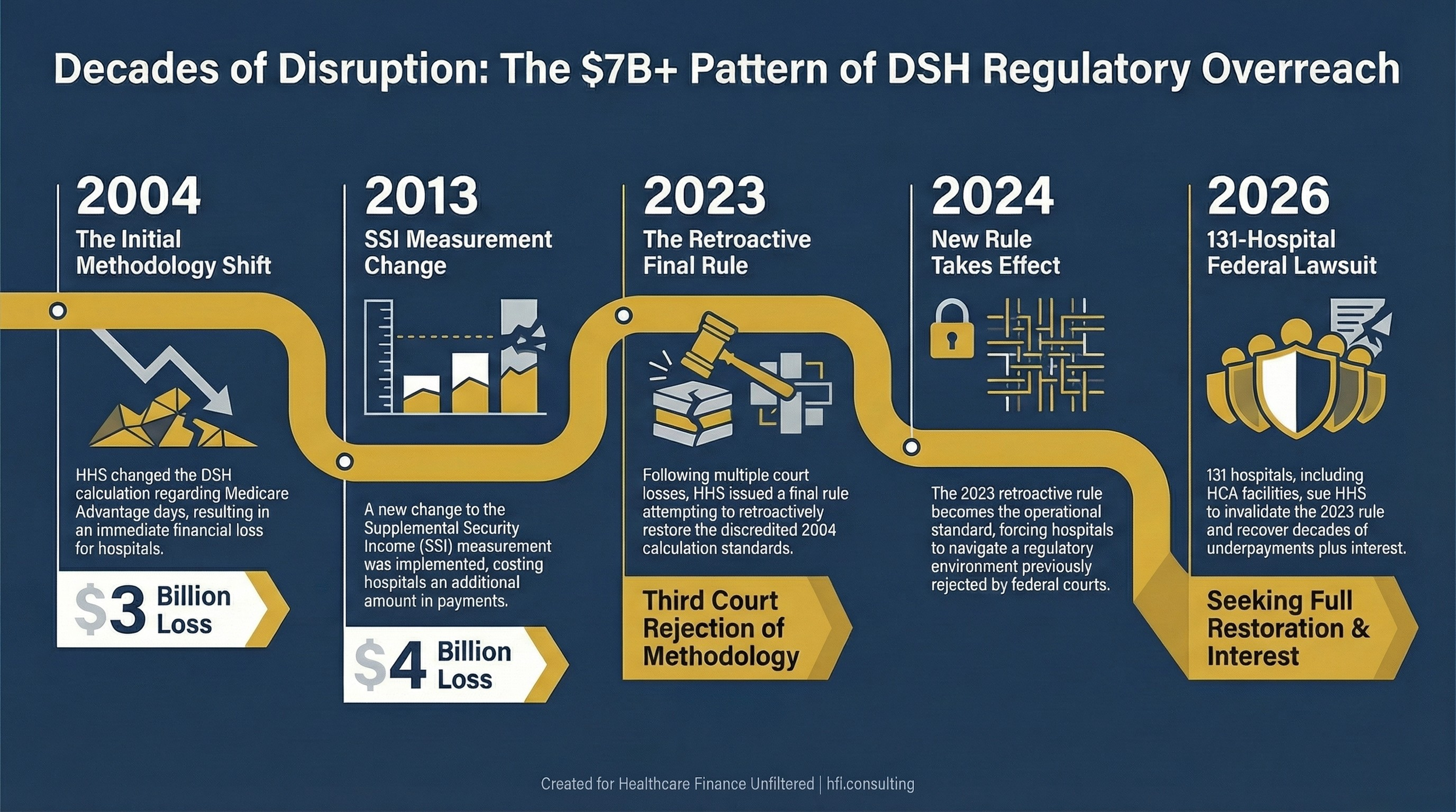
Timeline showing DSH payment calculation changes from 2004 to 2026 and their cumulative financial impact on safety-net hospitals
What This Looks Like from Inside a Safety-Net Hospital
I was the cost accountant for UF Health Jacksonville, a Trauma I facility, a Level 3 NICU, and a hospital with a mission built around serving Jacksonville's most vulnerable population. Part of my annual work involved the reporting required to support DSH payment calculations.
The City of Jacksonville maintained a separate indigent care fund, independent of federal DSH payments. That fund was $18 million. It has never increased since 2004. To put that number in context: the City expected that $18 million to cover the low-income care needs of an entire metropolitan area with one of Florida's highest poverty rates.
DSH payments were a reliable revenue line, but reliable did not mean adequate. What it meant in practice was that UF Health operated on the assumption that government funding would cover a fraction of indigent care costs and that the gap would have to be filled by grants, philanthropy, and internal cross-subsidy.
The other calculation that drove constant internal conversation was case mix index. UF Health's CMI needed to reflect what the patient population actually looked like: sicker, more complex, burdened by social determinants of health that compounded clinical acuity. When a patient is choosing between insulin and groceries, their health outcomes reflect that choice by the time they reach your ED. The CMI captures the clinical reality of social deprivation. The DSH calculation is supposed to capture the financial reality of serving that same population. When either calculation is manipulated, safety-net hospitals absorb the loss.
The CFO Decision Framework: Three Options
This lawsuit creates a decision point that finance leaders at eligible hospitals should not outsource entirely to legal counsel. The decision has a financial dimension that belongs in the CFO's office.
Here are the three positions available to you, with the considerations attached to each.
Option 1: Join the Lawsuit
The financial case for joining is straightforward at the portfolio level. Courts have ruled against HHS three times on this same methodology. The precedent favors the plaintiffs. As more hospitals join, the legal weight of the complaint increases and the per-hospital cost of litigation decreases. If the court orders restoration of the pre-2004 standard and back payments with interest, hospitals that joined the lawsuit position themselves to recover funds that have been calculated incorrectly for up to two decades.
The cost of inaction is real. If you have operated under the post-2004 calculation since 2004, you have been leaving money on the table for 20 years. The question is whether the cost of joining the litigation is justified by the recovery potential given your hospital's DSH exposure level.
Option 2: Wait and See
A wait-and-see posture makes sense if your legal team has significant concerns about resource allocation, if your DSH exposure is relatively modest, or if you need to assess how the case proceeds through the courts before committing. This is a defensible position, not a passive one.
If you choose this path, do the financial work now. Model your DSH exposure under the pre-2004 calculation methodology versus the current methodology. Understand the dollar gap between those two scenarios across the years affected. That analysis will tell you whether joining later, if the case succeeds and creates a broader remedy, is worth pursuing. Do not let the wait-and-see position become an ignore-and-miss position.
Option 3: Move On
Some hospitals have limited DSH exposure. If Medicare Advantage patient days represent a small share of your payer mix, the calculation difference between pre-2004 and current methodology may not generate a material financial recovery. In that case, the rational decision is to monitor the case for any precedent that affects your reimbursement strategy and allocate your legal resources elsewhere.
The mistake is making this decision without running the numbers first. "We'll let legal handle it" is not a financial strategy.
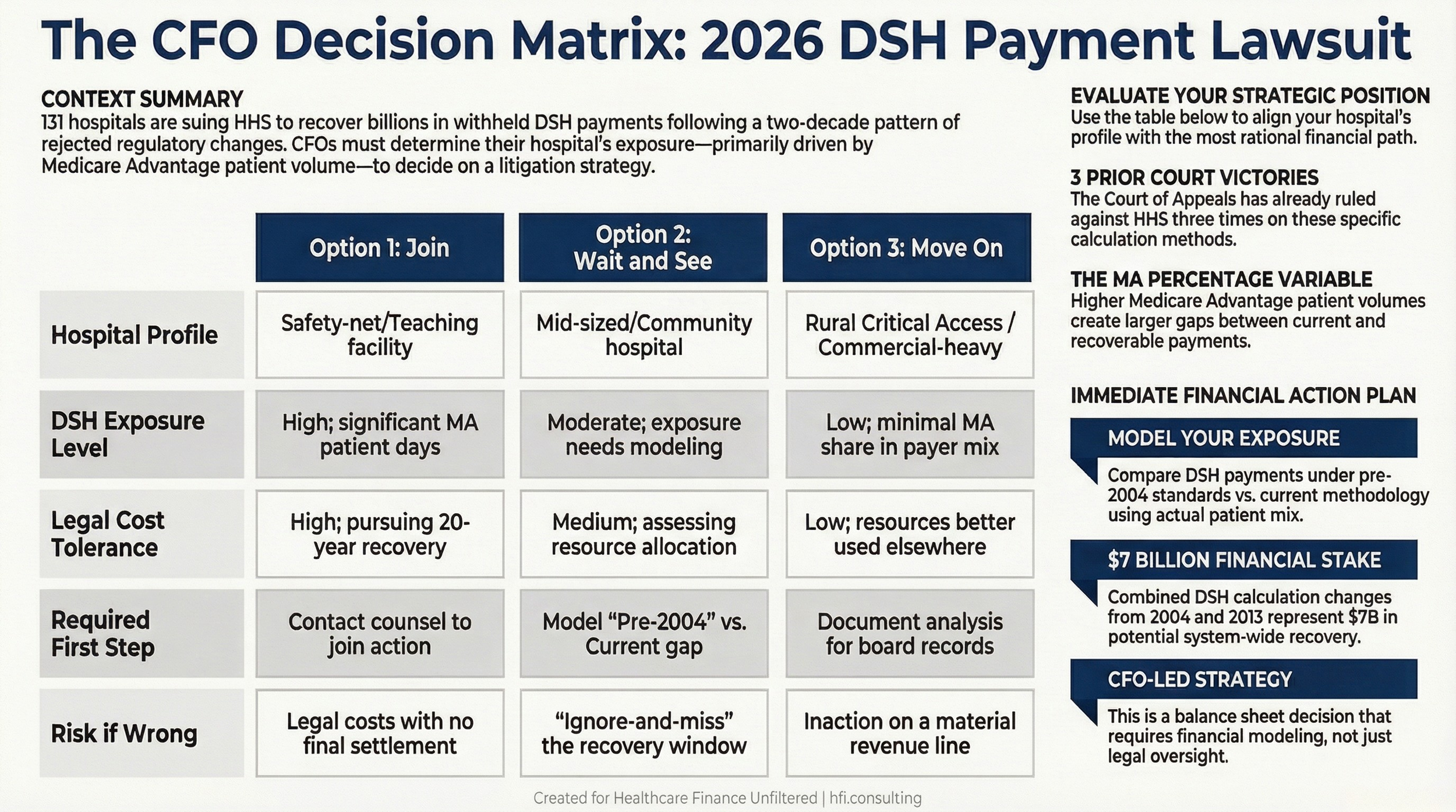
Decision matrix comparing the financial tradeoffs of joining, watching, or bypassing the 2026 HHS DSH payment lawsuit for hospital CFOs
Who Benefits Most from This Litigation
Not all hospitals have equal exposure. Safety-net hospitals and academic medical centers with high Medicaid and uninsured volumes stand to recover the most if the pre-2004 methodology is restored.
Here is why. The DSH calculation is driven by the concentration of low-income patient days in your total volume. Teaching hospitals and safety-net facilities typically carry higher SSI fractions and Medicaid fractions than community hospitals. The calculation changes that shifted how Medicare Advantage patient days were counted had a proportionally larger impact on hospitals where those fractions were already elevated.
Rural Critical Access Hospitals operate under a different DSH methodology and may have limited exposure to this particular calculation dispute. Community hospitals with primarily commercial and Medicare fee-for-service payer mixes will see smaller gaps between the pre-2004 and current calculation. The hospitals with the most to gain are the ones already serving the populations DSH was designed to protect.
If you are building the financial case for your executive team or board, the DSH Compliance and Recovery Planning Checklist I have outlined below gives you a structured starting point. Reply to this email and I will send you the framework directly.
What Your Finance Team Should Do This Week
Regardless of which option your hospital chooses, these steps belong on your near-term work plan.
First, pull your cost reports and identify your DSH payment history under the current methodology. Go back as far as your records allow, but prioritize fiscal years 2021 through present as a starting point.
Second, identify your Medicare Advantage patient day volume as a percentage of total Medicare inpatient days. This is the core variable driving the calculation difference between pre-2004 and current methodology. The higher that percentage, the larger the gap in your scenario analysis.
Third, contact legal counsel to understand the mechanics of joining the existing lawsuit versus a separate action. There are cost and timing considerations that will vary by hospital and jurisdiction. Do not assume this option has closed simply because the lawsuit has already been filed.
Fourth, model both scenarios explicitly. Pre-2004 calculation versus current calculation, applied to your actual patient day mix. If the recovery potential is material, the decision about whether to join or wait becomes significantly easier to make.
Finally, document your analysis. If the case succeeds and creates a broader remedy, having your financial analysis completed now positions you to act quickly.
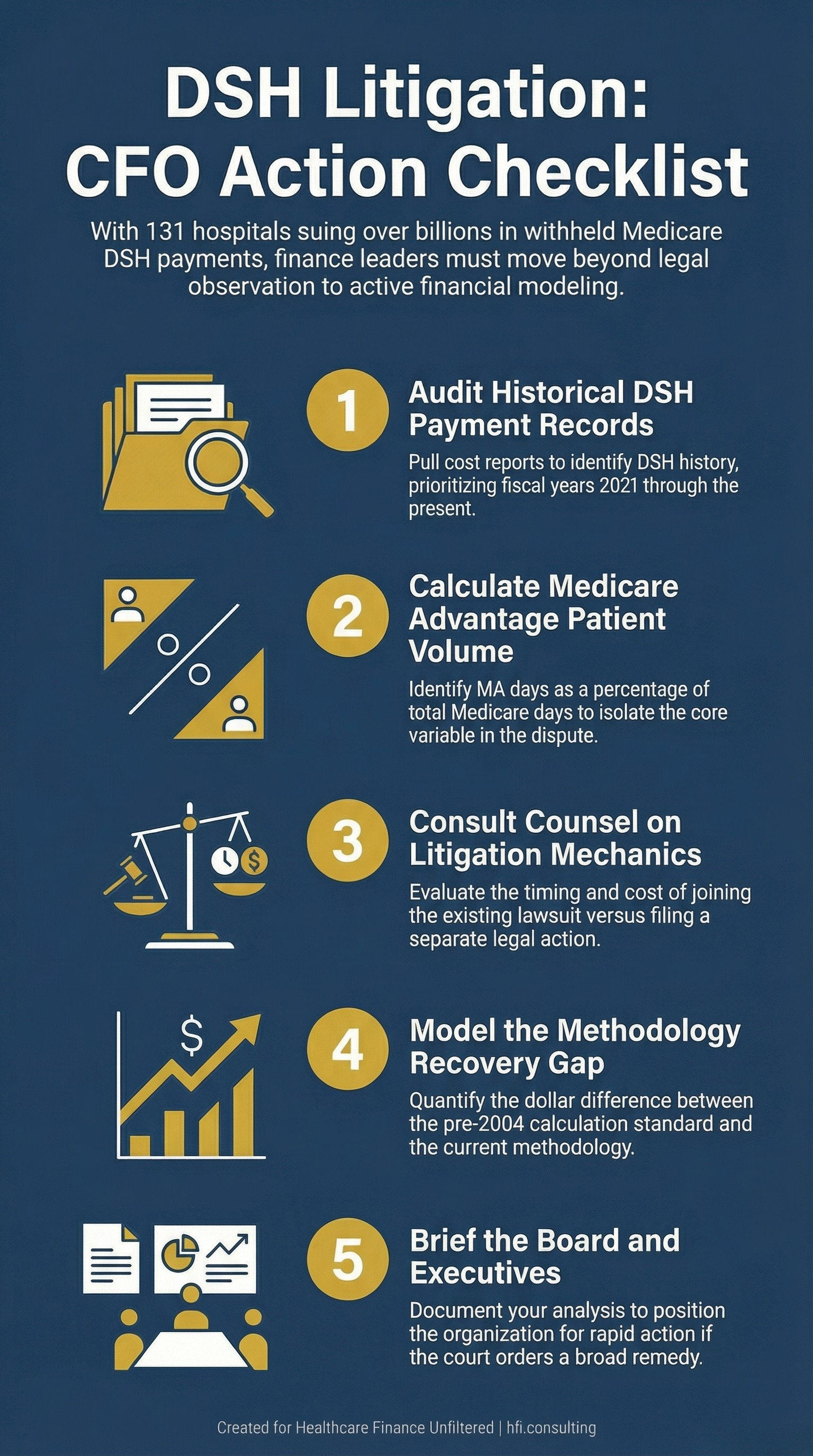
Five-step action checklist for CFOs assessing DSH lawsuit exposure and deciding whether to join the 2026 HHS litigation
The Bigger Picture
This lawsuit is not just about DSH payments. It is about whether federal agencies can repeatedly change reimbursement methodology in ways that courts have repeatedly rejected, absorb the adverse rulings, and then attempt to retroactively restore the same changes under a new regulatory vehicle.
For CFOs, the pattern has implications beyond this specific litigation. The same dynamic has played out in 340B program reimbursement disputes, in Medicare Advantage rate-setting challenges, and in prior authorization rule enforcement. CMS and HHS have a documented history of using rulemaking to achieve outcomes that courts have declined to authorize.
For more on how federal regulatory disputes translate into balance sheet risk, see my earlier analysis of the $172 billion Medicaid cut facing hospital facility fees. "Hospital Facility Fees Under Siege"
The rural hospital impact of Medicaid funding uncertainty is covered in detail here. "Rural Hospitals Already in the Red"
The safety-net hospital system in this country operates on the assumption that the government will be a reliable, if limited, partner. When that assumption is undermined by methodological manipulation over two decades, the financial consequences compound in ways that are difficult to reverse.
Safety-net and teaching hospitals are not the only ones watching this case. The outcome will signal to the entire provider sector how aggressively the current administration will defend regulatory positions that have already been rejected by the courts.
Healthcare Finance Unfiltered covers regulatory and reimbursement developments through a CFO lens, without the policy advocacy framing. If this analysis is useful to your team, a paid subscription keeps this work going. Visit hfi.consulting to learn more.
The Bottom Line
The 131 hospitals that filed this lawsuit are not making a political statement. They are attempting to recover money that courts have repeatedly said they are owed. The financial stakes, $3 billion in the 2004 change alone, $4 billion in the 2013 change, are not rounding errors for safety-net facilities operating on 2 to 3 percent margins.
For CFOs at eligible hospitals, the question is not whether this litigation is justified. The courts have already weighed in on that question three times. The question is whether your hospital's DSH exposure level makes joining, waiting, or watching the right financial decision.
Run the numbers before you answer.
If your team is working through DSH exposure analysis or needs a framework for presenting this decision to your board, I am happy to connect. Reply directly to this email or reach out through hfi.consulting
P.S. Safety-net and teaching hospital CFOs: what percentage of your total Medicare inpatient days are currently Medicare Advantage? Hit reply and tell me. That single number is the starting point for calculating your exposure in this lawsuit, and I am curious how broadly it varies across your organizations.