
CY 2027 Medicare Advantage Final Rule: What MA Finance Leaders Must Plan For Now
CMS just cut 11 Star Ratings measures and dropped health equity mandates. Here's what it means for your 2027 budget.
CY 2027 Medicare Advantage Final Rule: What MA Finance Leaders Must Plan For Now
On April 2, 2026, CMS dropped the Contract Year 2027 Medicare Advantage and Part D Final Rule. If you manage finances for an MA plan, this one hits your quality budget, your compliance infrastructure, and your actuarial models for 2027.
The headline is deceptively simple: CMS is cutting administrative burden. But the details carry real financial implications, and plans that move slowly on modeling these changes will find themselves behind on Star Ratings strategy before open enrollment.
Here's what you need to know and how to build it into your planning cycle now.
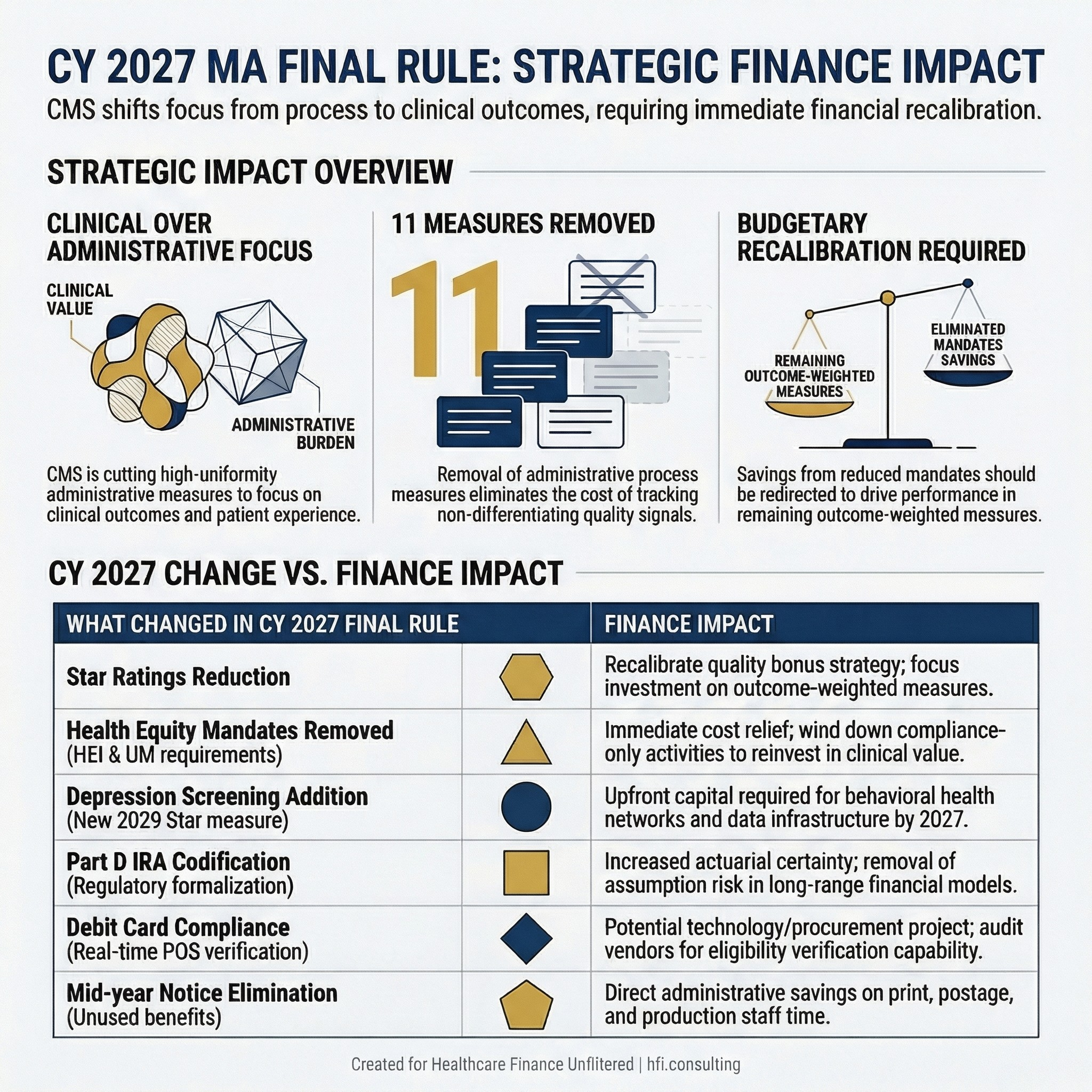
Table comparing CY 2027 Medicare Advantage Final Rule changes with corresponding finance and operational impacts for MA plan leaders
The Star Ratings Overhaul: Fewer Measures, Cleaner Signal
The CY 2027 final rule removes 11 measures from the Star Ratings calculation. These are administrative process measures and high-uniformity measures where nearly all plans perform at or near the same level, making them poor signals of actual plan quality.
For finance leaders, this matters for two reasons. First, the cost of tracking, reporting, and operationalizing measures that carry no meaningful scoring differentiation is not zero. Staff time, vendor contracts, and quality committee hours have all been directed at measures that CMS itself now acknowledges offer "little meaningful distinction between plans." Second, with a leaner measure set, your quality bonus payment strategy has to be recalibrated against what remains.
The measures staying in place are weighted toward outcomes, intermediate outcomes, and patient experience. That's the right direction for a quality program, but it means plans that have been coasting on strong administrative process scores while underinvesting in clinical outcomes will feel this shift in their bonus calculations.
Review your current Star Ratings performance breakdown before your next QI committee meeting. Know which of your top-performing measures are being removed and which remaining measures represent the greatest gap opportunity.
The Health Equity Provisions: A Significant Rollback
This is the change that will draw the most industry attention, and MA finance leaders need to understand it clearly before commenting internally or externally.
CMS is eliminating three health equity requirements under Executive Order 14192's burden-reduction mandate:
The requirement for MA Utilization Management Committees to include a health equity expert member is gone. The requirement to conduct annual health equity analyses of UM decisions is gone. The requirement to publicly post those analyses is gone.
CMS is also eliminating the requirement for MA quality improvement programs to include activities specifically designed to reduce health disparities.
Separately, the Health Equity Index reward (previously called the Excellent Health Outcomes for All reward) is not being implemented for 2027 Star Ratings. CMS is instead continuing the historical reward factor that incentivizes high performance across all enrollees rather than targeted performance for a subset.
From my experience on the payer side at Florida Blue Medicare, health equity analytics programs are not cheap to administer. Data infrastructure, vendor relationships, and committee governance around equity-specific reporting represent real budget line items. The removal of these mandates creates immediate cost relief for plans that were building or maintaining these programs primarily for compliance purposes.
However, plans operating in markets with significant dual-eligible or vulnerable population concentrations should not treat this as permission to exit equity-focused programs entirely. The regulatory mandate is gone; the business and reputational case for serving these populations well is not.
Model the budget impact of winding down compliance-only health equity activities separately from programs with demonstrated clinical or retention value. These are not the same decision.
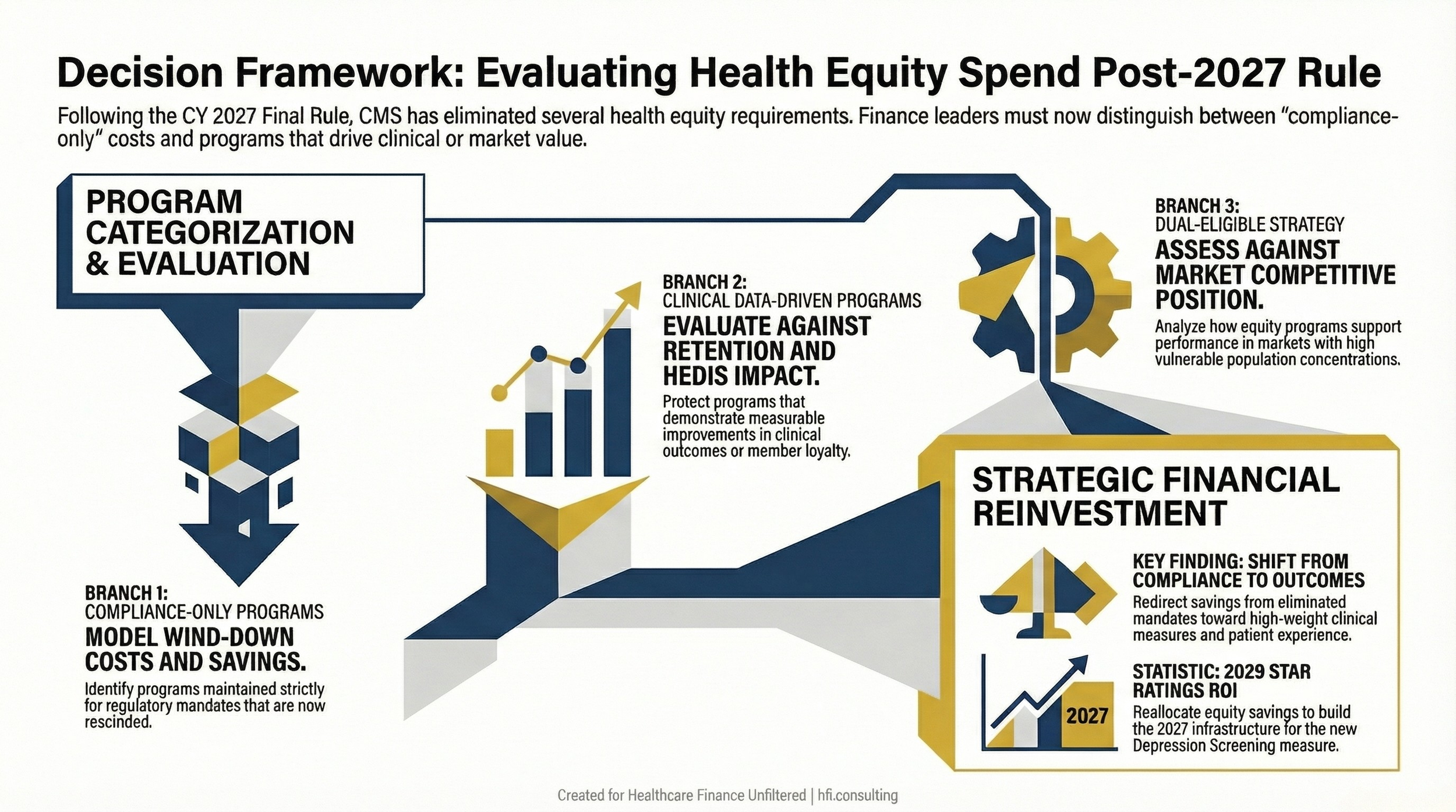
Decision flowchart for MA plan finance leaders evaluating health equity program investments following CMS 2027 rule changes removing mandatory health equity requirements
Depression Screening: The New Measure Coming in 2029 Star Ratings
CMS is adding a Part C Depression Screening and Follow-Up measure, with the measurement year beginning in 2027 and the measure impacting 2029 Star Ratings.
The two-year runway sounds long. It is not. Plans that wait until 2028 to build clinical workflows, provider network agreements, and member outreach programs around depression screening will be behind when the measure starts counting.
From a finance planning perspective, this is a capital allocation question. Behavioral health network development, member engagement programs, and data infrastructure for tracking screening completion and follow-up rates all require upfront investment. The return is in 2029 Star Ratings performance, which drives quality bonus payments and rebates.
Build a preliminary business case now. Estimate the per-star-point value of bonus payments for your contract, model the investment required to move from your current behavioral health screening baseline to the performance level needed to score at the three-star threshold on this measure, and present it as a 2026-2027 investment for a 2029 return.
That is the kind of forward-looking analysis that finance leaders can offer QI and clinical leadership that no other function will bring to the table.
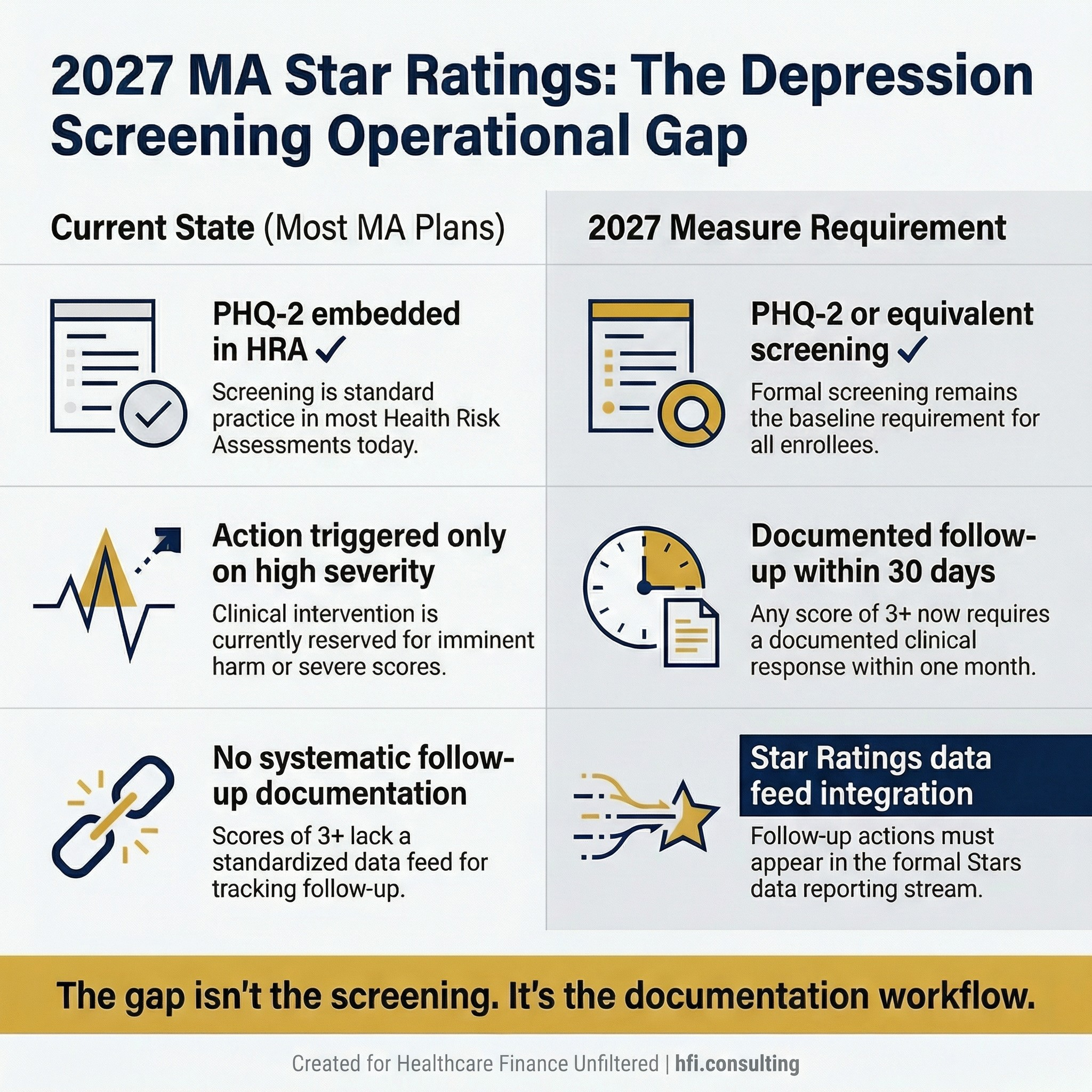
Side-by-side comparison infographic showing the gap between current MA plan PHQ-2 HRA workflows and CY 2029 Depression Screening Star Ratings measure requirements
From the Payer Side: The Follow-Up Gap Most Plans Won't See Coming
Many MA plans already have depression screening built into their Health Risk Assessment. PHQ-2 questions are embedded, members are completing them, and care management teams are reviewing the responses. On paper, the infrastructure for this measure already exists.
The problem is what happens next.
In a typical MA HRA workflow, follow-up action on PHQ-2 responses is triggered by clinical severity. A score suggesting significant depression or imminent risk gets routed to care management. A score of 3 on a 0-to-6 scale, the lowest threshold that counts as a positive screen under the HEDIS measure framework, often receives no documented action at all. A clinician may review it and make a judgment call. That judgment call may never appear in a system that feeds Star Ratings reporting.
That is a measure failure. Not a clinical one. A documentation one.
Plans that discover this gap in 2028 will not have time to fix it before the measurement year closes. The work to map the data flow from PHQ-2 response to follow-up action to Star Ratings data feed needs to happen now, in 2026, while there is still runway to build and pilot a revised protocol.
The follow-up itself does not have to be a psychiatric referral. A documented outreach call from a qualified care management staff member, a scheduled appointment, or a step-up to a PHQ-9 administration can all qualify. Plans with strong care management teams are likely already making these contacts. The question is whether those contacts are being documented in a way that creates a measureable numerator event.
For finance leaders, this is the business case framing: the investment required is not in building new clinical programs. It is in closing the loop between clinical activity that is already happening and the documentation infrastructure that translates that activity into Star Ratings performance.
That is a workflow and data integration project. It has a cost. It also has a 2029 quality bonus payment return that can be modeled now.
Part D: IRA Changes Are Now Codified
The Inflation Reduction Act restructured Medicare Part D significantly, and CMS has been implementing those changes through program instructions since 2023. With that program instruction authority expiring, CMS is codifying the changes in regulation for 2027 and beyond.
The codified elements include elimination of the coverage gap phase, the reduced annual out-of-pocket threshold, removal of cost sharing in the catastrophic phase, the Manufacturer Discount Program that replaced the Coverage Gap Discount Program, and updates to True Out-Of-Pocket cost calculations, specialty-tier rules, and reinsurance payment methodologies.
For MA-PD plans, the primary finance implication is certainty. These provisions are no longer subject to year-by-year program instruction updates. Your actuarial models for Part D liability can be built on a stable regulatory foundation for 2027 and beyond.
If your plan has been carrying the assumption risk around whether IRA provisions would continue, that uncertainty is now resolved. Update your long-range financial models accordingly.
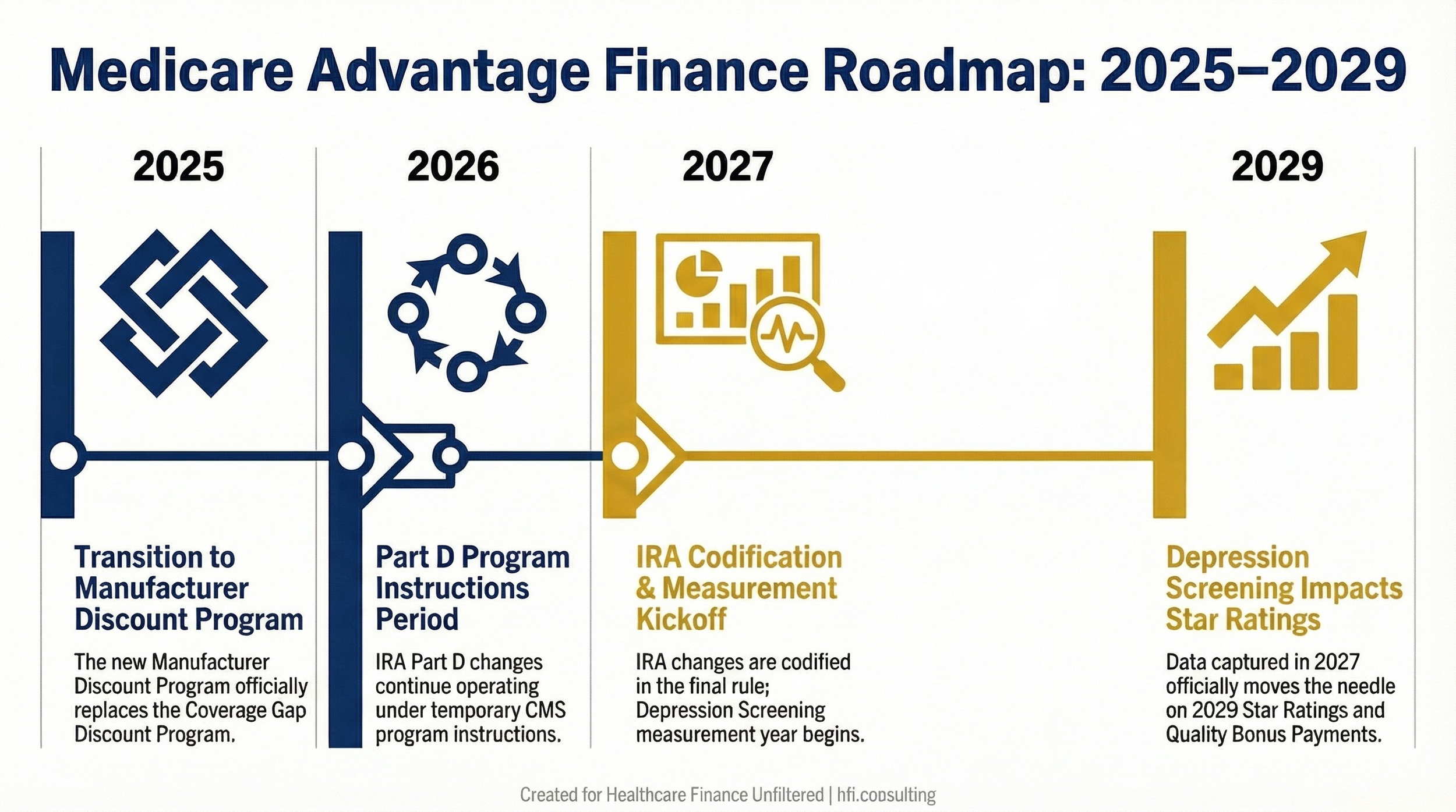
Timeline showing Medicare Advantage and Part D regulatory changes from 2025 through 2029, including IRA codification in 2027 and Depression Screening measure impact in 2029 Star Ratings
Supplemental Benefits: Debit Card Compliance and Reduced Notices
CMS is finalizing two supplemental benefit provisions that carry operational cost implications.
For debit card administration, plans must now electronically link debit cards to covered items and services through a real-time identification mechanism that verifies benefit eligibility at the point of sale. Cards must also be limited to the specific plan year. If your plan uses debit cards for supplemental benefit delivery and you have not already implemented real-time eligibility verification at point of sale, this is a technology and vendor contract project, not just a policy update.
On the notice side, CMS is rescinding the requirement for plans to send mid-year notices about unused supplemental benefits. This is a straightforward administrative cost reduction. Model the savings on print, postage, and staff time associated with mid-year notice production and distribution.
The cannabis SSBCI clarification is worth noting for any plans that have been exploring or already offering cannabis-related supplemental benefits. CMS has clarified that cannabis products illegal under applicable state or federal law are not allowable as SSBCI. This is a reminder to audit your supplemental benefit offerings against current state and federal law before finalizing your 2027 benefit design.
What Your Finance Team Should Do Before Q3
The CY 2027 final rule creates a clear set of planning actions. The plans that move on these now will have a material advantage in 2027 bonus payments and 2029 Star Ratings performance.
Star Ratings recalibration. Pull your current measure-by-measure Star Ratings performance and identify which of the 11 removed measures contributed to your scores. Remodel your projected Star Ratings without those measures and identify the gap measures where investment will have the greatest impact on your bonus payment tier.
Health equity budget review. Separate compliance-mandated equity activities from programs with demonstrated clinical or member retention value. Build a budget scenario that models the savings from winding down compliance-only programs against any reputational or market risks.
Depression Screening investment case. Build a 2026-2027 capital request for behavioral health network and data infrastructure investments tied to the new Depression Screening measure. Frame it as a 2029 Star Ratings and quality bonus payment return on investment.
Part D model update. Update your long-range actuarial models to reflect codified IRA provisions. Remove assumption risk carryovers from prior years.
Debit card vendor audit. Confirm that your supplemental benefit debit card vendor can meet the real-time eligibility verification requirement. If not, this is a 2027 procurement and implementation project that needs to start now.
If you want a structured framework for working through these five planning priorities with your team, HFI readers can access the MA Finance Planning Checklist at hfi.consulting. It includes the budget modeling questions, the Star Ratings recalibration worksheet inputs, and the Depression Screening business case template.
The MA Finance Planning Checklist for CY 2027 is available at hfi.consulting. It covers all five planning priorities from this article in a format you can take directly into your next finance-QI leadership meeting.
The Bigger Picture: What This Rule Signals
CMS is explicitly reducing regulatory burden under Executive Order 14192. That framing matters for how MA finance leaders interpret not just this rule but the direction of future rulemaking.
The removal of health equity mandates, the elimination of duplicative reporting requirements, and the rescission of mid-year notices all reflect a deliberate pivot away from administrative compliance as a proxy for plan quality. CMS is betting that a leaner, clinically focused measure set will better serve beneficiaries and create more meaningful competition among plans.
For plans that exited MA markets in recent years citing unsustainable administrative and compliance costs, this rule removes some of the friction that contributed to those decisions. Whether it is enough to reverse market exits at scale remains to be seen. But the trajectory is clear.
For finance leaders still in the market, the question is whether your organization is positioned to compete on clinical outcomes and patient experience rather than administrative process compliance. That is a capital allocation question as much as a clinical one.
The plans that will win in 2027 and 2029 are the ones whose finance leaders are building business cases for clinical quality investments today.
What This Means for Your 2027 Budget
The CY 2027 final rule is not a dramatic overhaul. It is a targeted recalibration that reduces administrative compliance costs while raising the bar on clinical quality performance.
For MA finance leaders, that is a net positive in terms of operational burden. But it requires active management. The savings from eliminated health equity mandates and mid-year notices do not automatically flow to the bottom line. They need to be redirected toward the investments that will drive performance on the measures that remain.
Start the recalibration now. Your 2027 budget cycle is closer than it looks.
If you lead finance for an MA plan or work alongside plan leadership on quality strategy, I want to hear what you're seeing in your market. What's the biggest budget pressure you're navigating heading into 2027 planning? Hit reply and tell me. These conversations shape what I write next.
Healthcare Finance Unfiltered publishes analysis like this every week. If a colleague would find this useful, forward it directly.
P.S. The Depression Screening measure doesn't hit Star Ratings until 2029, but the measurement year starts in 2027. What's your plan's current baseline for behavioral health screening completion rates? That number will determine whether this is a crisis or an opportunity in your 2029 bonus payment calculations. Hit reply and let me know where you're starting from.