
Critical Access Hospital CFO Toolkit: Financial Controls, AI, and Margin Strategy
When one person wears every hat, internal controls and smart technology aren't optional. They're survival tools.
The CFO of a critical access hospital is not a job description. It is a collection of fifteen job descriptions held together by institutional knowledge and sheer determination. The finance director who closes the books on Friday may also be fielding a vendor escalation on Saturday and presenting to the board on Monday. That is not a staffing gap. That is the operating model.
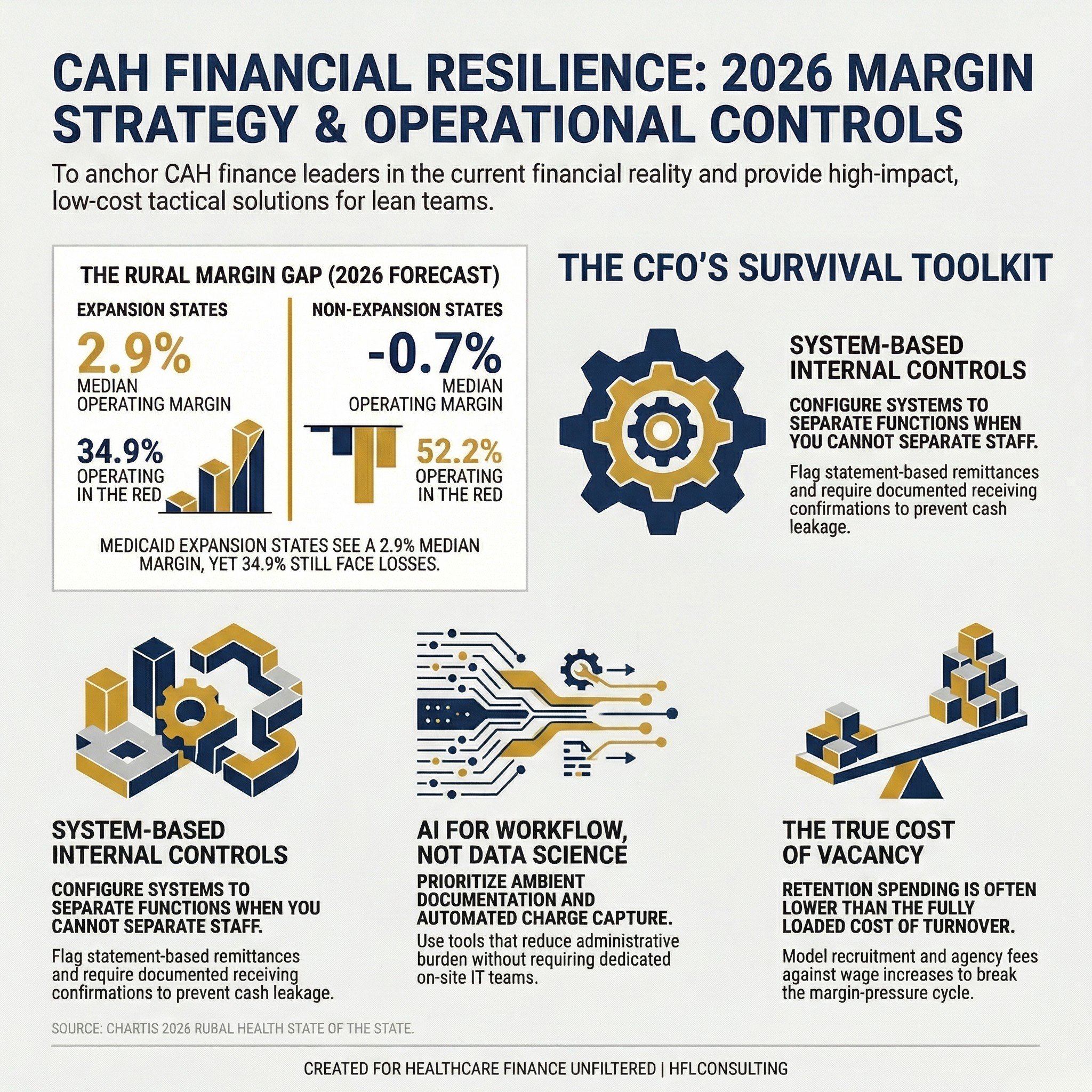
Split stat card comparing 2025 operating margins for rural hospitals in Medicaid expansion versus non-expansion states, showing -0.7% median margin in non-expansion states.
Running a critical access hospital's financial operations requires a particular kind of professional resilience. The structural constraints are real: thin margins, a Medicaid-heavy payer mix, aging facilities, workforce shortages, and a community that depends on the organization to remain viable. Against that backdrop, CFOs are also navigating a wave of regulatory and technology change that would challenge a health system ten times the size.
The data confirms what CAH finance leaders already know. According to Chartis's 2026 Rural Health State of the State report, rural hospitals in Medicaid non-expansion states carried a median operating margin of negative 0.7 percent in 2025, with 52.2 percent operating in the red. Expansion states fared better at a 2.9 percent median, though 34.9 percent still had negative margins. Improvement is real, but fragile.
This is the environment in which CAH CFOs are expected to build financial stability, deploy technology thoughtfully, and maintain the internal controls that protect the organization. This article is a practical toolkit for doing exactly that.
The Multi-Hat Reality and Why It Creates Financial Risk
The operational structure of a critical access hospital almost guarantees role overlap. A facility with 25 inpatient beds and 50 employees simply cannot staff every function the way a regional medical center can. The accounts payable function and the materials management function may sit with the same person. The CFO may also carry compliance responsibilities. The revenue cycle director may double as the billing supervisor.
This is not a criticism. It is a structural feature that finance leaders must design around rather than ignore.
When I worked as a Revenue Recovery Auditor for The Audit Group, we routinely reviewed CAH and small rural hospital operations as part of broader AP recovery engagements. One of the most consistent red flags we encountered was the combination of accounts payable and materials management under a single staff member with limited oversight. The vulnerabilities were specific and recurring: vendors being paid from statements rather than invoices, returned goods not generating credits against the account, and duplicate payments sitting in the system undetected because no one had cross-functional visibility to catch them.
These are not fraud scenarios. They are control failures that happen when good people are stretched beyond the scope of any reasonable job description. The financial exposure from AP leakage alone can be significant for an organization operating at negative margins. A $15 million facility paying on statements instead of invoices and missing 60 percent of its return credits is leaving real money on the table every month.
The answer is not to hire your way out of the problem. The answer is to build controls that work within the staffing model you actually have.
Internal Controls for Lean Operations
The core principle for CAH internal controls is separation of function, even when you cannot separate the people. That means using system configuration, workflow rules, and documented approval chains to create oversight checkpoints that do not require additional headcount.
For accounts payable specifically, the highest-priority controls are these. Require that all payments process against a purchase order or approved invoice, never against a statement. Configure your AP system to flag statement-based remittances before they reach the payment queue. Assign a second reviewer, even if that reviewer is the CFO or a department director outside finance, to approve any payment above a defined threshold. Run a monthly credit balance report against all vendor accounts and route that report to someone other than the person who processes the payments.
For materials management, implement a receiving confirmation step that is separate from the purchase approval. Even if the same person performs both functions, requiring a documented receiving confirmation creates a timestamped record that can be audited. Require return authorizations to generate a credit memo request as part of the workflow, not as an optional follow-up.
None of these controls requires new software. Most require only configuration changes and a documented policy. The investment is time. The protection is operational.
For payroll, which is often another area of risk in lean organizations, require dual approval on any new employee setup and any rate change. Segregate the payroll submission function from the payroll approval function, even if that means the CFO reviews and releases payroll rather than delegating it entirely.
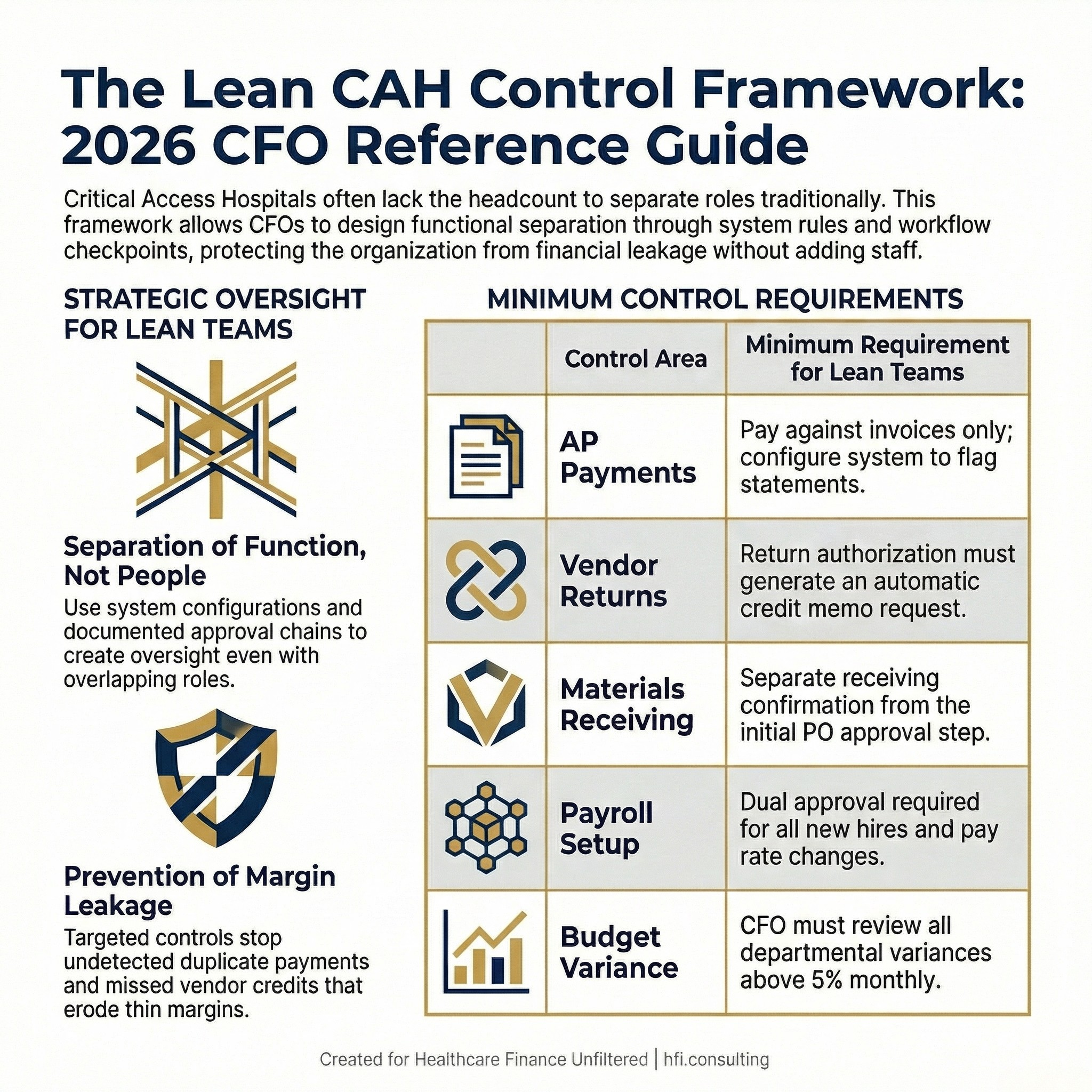
Five-row internal controls framework table for critical access hospitals operating with lean finance teams, showing minimum control requirements by functional area.
AI and Technology: What CAHs Can Actually Implement
The AHA's 2026 Knowledge Exchange on AI governance for rural hospitals makes a useful observation: rural hospitals are not behind on AI because they lack ambition. They are behind because they lack the patient volume, technical staff, and vendor infrastructure that larger systems use to justify and sustain AI investment.
That is a real constraint. It is also a narrower constraint than it appears, because the AI tools with the highest return in a CAH setting are not the complex clinical decision support systems that require data science teams to maintain. They are workflow tools that reduce administrative burden on staff who are already stretched.
Ambient clinical documentation is the clearest example. Multiple rural health system leaders cited in the AHA Knowledge Exchange reported that ambient scribing tools improved documentation accuracy and physician satisfaction without requiring a dedicated informatics team to manage. The physician-patient relationship improved because clinicians were no longer splitting attention between the patient and the EHR. Documentation compliance improved because the tool captured what was said rather than what the provider remembered after a long day.
For CAH finance operations, the equivalent entry points are AI-assisted denial management tools, automated charge capture review, and accounts payable automation that flags discrepancies before payment. These tools do not require your organization to build a data science capability. They require vendor selection, a documented implementation plan, and a realistic ROI threshold that accounts for your volume.
The governance framework matters as much as the tool selection. The AHA recommends starting with a risk-tiered approval process, clear vendor data-use expectations, and an annual revalidation requirement for every AI tool in use. For a CAH, that governance framework may be a one-page policy and a quarterly review with the CFO and the CEO. It does not need to be a standing committee. It needs to be documented and consistent.
A practical starting point: evaluate your three highest-volume administrative pain points and ask whether any of them have a software solution that does not require IT staff to implement and maintain. If the answer is yes, build the ROI case for that tool first before pursuing anything more complex.
Workforce and Wage Pressure
The labor constraint at critical access hospitals is not a staffing shortage in isolation. It is a wage gap problem layered on top of a pipeline problem, in markets where there is no backup workforce to draw from.
Chartis's 2026 data shows that rural hospitals with negative operating margins are not simply underfunded. Many are caught in a cycle where margin pressure limits wage competitiveness, which limits staff retention, which drives up agency and overtime costs, which further compresses margins. Breaking that cycle requires a financial strategy that is explicit about labor as a capital allocation decision, not just an operating expense.
For CFOs, that means modeling the fully loaded cost of turnover for key positions and comparing it to the incremental cost of a wage increase or a retention incentive program. The math on retention spending is often more favorable than CFOs expect, particularly for clinical and revenue cycle roles where replacement costs include travel nurse contracts and recruitment fees.
For healthcare workforce compensation strategy, the benchmark question is not just what the regional market rate is. It is what the cost of vacancy is for that specific role in your specific organization, and whether a targeted investment in retention changes that cost equation.
Rural health transformation funding, including the $50 billion Rural Health Transformation Fund that CMS recently began distributing to states, may create new flexibility for workforce investment. CAH CFOs should be tracking their state's application status and understanding what funding categories their state has proposed. Fifteen states have already submitted applications proposing alternative payment models for rural providers. The organizations that engage with their state Medicaid offices now will be positioned to access those funds faster when they become available.
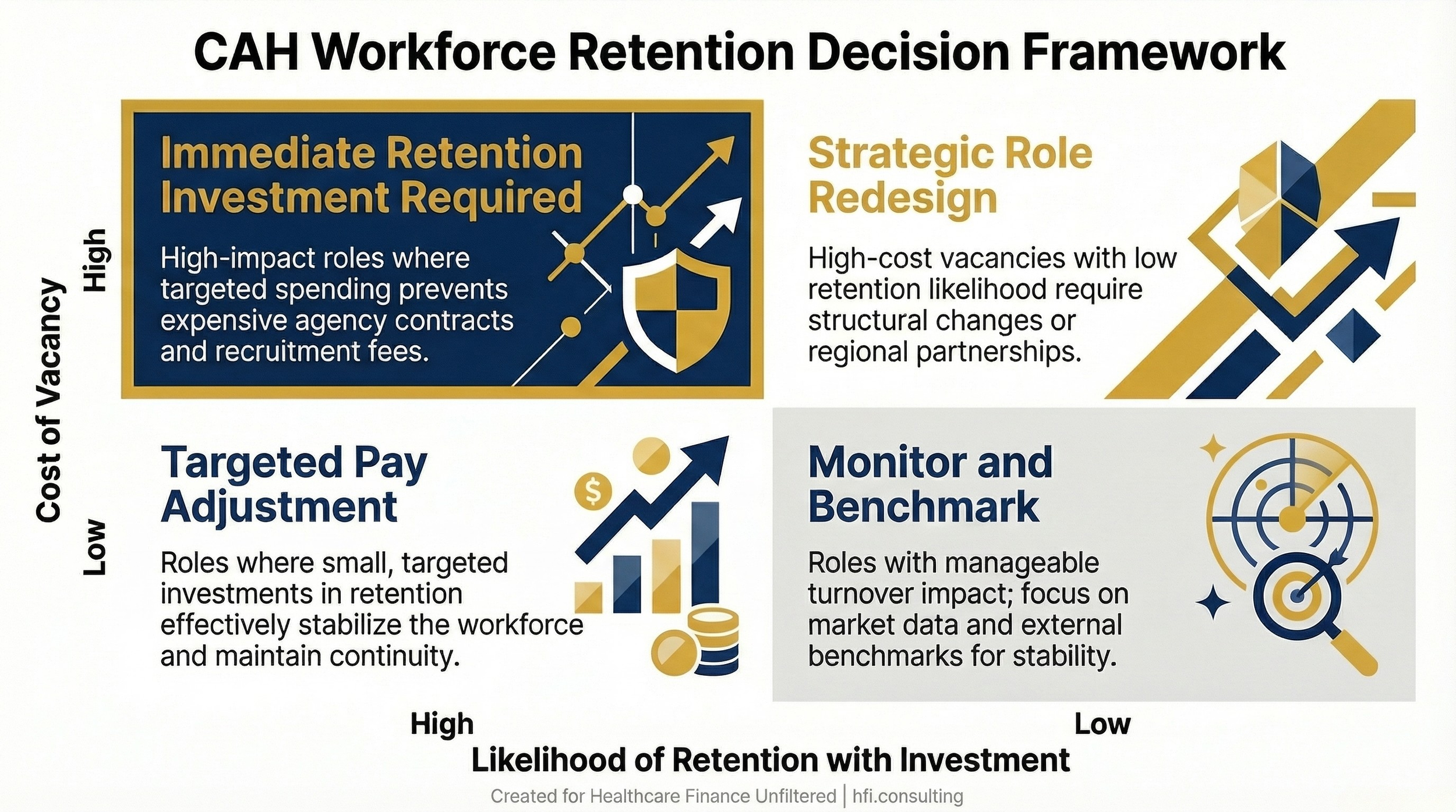
Two-by-two decision matrix titled CAH Workforce Retention Decision Framework, mapping cost of vacancy against retention likelihood to guide CFO investment decisions.
Community Outreach as a Financial Strategy
Community benefit reporting is a compliance requirement for nonprofit CAHs. It is also, when done well, a financial positioning tool. The organizations that can document community impact clearly are better positioned to access grant funding, engage local employers in direct contracting conversations, and build the kind of community trust that drives inpatient volume to their facility rather than to a regional competitor 90 miles away.
The finance function has a direct role in this. Accurate community benefit accounting, inclusive of the unreimbursed cost of Medicaid, charity care, community health education programs, and subsidized services, requires the same cost accounting discipline as any other financial analysis. If your cost accounting system is not allocating overhead to community benefit programs accurately, your reported community benefit figure understates the organization's true contribution.
That matters operationally. When local employers, county commissioners, or state legislators are evaluating whether to support funding for your organization, they are looking at your community benefit data. When your board is assessing the organization's strategic position, community benefit documentation is part of the evidence base.
Strategic Options: Knowing When to Restructure
For CAHs facing sustained negative margins, the strategic question is not whether to change but which change creates the best combination of financial stability and community access. The current environment offers more structured options than were available five years ago.
Rural Emergency Hospital conversion is the most discussed option and the most irreversible. Since January 2023, 44 rural hospitals have converted to REH status, gaining higher Medicare payments in exchange for eliminating inpatient services. The CFO of Mercy Hospital in Moundridge, Kansas, told HFMA that conversion turned around his organization's finances and allowed the addition of services the community actually needed. The tradeoff is real. Once inpatient capacity is eliminated, rebuilding it is not straightforward. Before pursuing REH conversion, model the financial impact across three scenarios: your current trajectory, REH conversion, and a regional partnership structure.
Critical Access Hospital status conversion, which 45 hospitals pursued over the past three years, offers higher Medicare cost-based reimbursement without the inpatient service elimination that REH requires. The constraint is the 25-bed limit and the 35-mile distance requirement from the nearest hospital. If your organization qualifies and has not pursued CAH designation, this is a conversation worth having with your reimbursement counsel.
Regional partnerships, whether for shared specialist services, back-office functions, or clinical integration, are gaining momentum as a middle path. The model of one hospital employing a specialist who provides services across multiple rural facilities reduces the cost of specialty access without requiring full consolidation.
The CFO's Role in Organizational Resilience
The stress of running a CAH finance function is real and worth naming directly. The margin for error is thin, the regulatory environment is shifting, the technology landscape is changing faster than most small organizations can absorb, and the personal accountability for every financial decision is concentrated in a very small leadership team.
That concentration of responsibility also means the CFO's contribution to the organization is outsized. The internal controls you build protect the organization from the leakage that quietly erodes margin. The workforce strategy you develop determines whether the nursing staff stays or leaves. The capital decisions you make shape whether the facility is viable in five years. Those are not small jobs.
What makes the role sustainable is a clear framework for prioritizing where to spend finite time and attention. Fix the controls that protect cash. Evaluate the technology that reduces administrative burden. Model the workforce scenarios that break the turnover cycle. Track the regulatory options that could change your reimbursement structure.
If you are navigating CAH finance operations and want a practical framework for internal controls, AI governance, or workforce retention modeling, I put frameworks like these into every issue of Healthcare Finance Unfiltered. Subscribe at hfi.consulting to get the next one directly in your inbox.
The Path Forward Is Incremental, Not Transformational
The rural hospital financial improvement that Chartis documented from 2023 to 2025 did not come from a single policy change or a single strategic pivot. It came from a combination of state-level Medicaid expansion, targeted funding programs, and operational decisions made by finance leaders who understood their specific market and their specific cost structure.
The CAH CFOs who are building sustainable organizations in 2026 are not waiting for a federal rescue. They are building the controls that protect cash, the technology foundation that reduces administrative burden, the workforce strategy that stabilizes staffing, and the community relationships that sustain volume. They are doing this with lean teams, limited capital, and deep institutional knowledge of markets that most consultants have never visited.
That is what this work looks like in practice. Incremental, disciplined, and grounded in the specific financial reality of the organization.
If you are a CAH finance leader dealing with a specific challenge in internal controls, AI implementation, or workforce strategy, I want to hear about it. Hit reply and tell me what you are working through. The most useful content I write comes directly from questions like yours.
P.S. What is the single biggest internal control gap you are aware of in your current CAH operation? Is it in AP, payroll, charge capture, or somewhere else? Hit reply and tell me. I am building a follow-up piece on CAH-specific control failures and want to include perspectives from finance leaders who are living this in real time.