
Florida Outpatient Diagnostic Center Acquisitions 2026: CFO Guide to Due Diligence, Hidden Pitfalls, and ROI Maximization
What every finance leader must evaluate before signing on a diagnostic imaging deal in Florida's booming $6.7B market.
Florida’s outpatient diagnostic market is on fire right now. With the state’s lab market projected to hit $6.7 billion in 2026 and over 4,200 diagnostic businesses actively operating, buyers are circling deals on BizBuySell and Synergy Business Brokers at a pace not seen since pre-pandemic. Multi-modality imaging centers in Palm Beach, Miami-Dade, and Central Florida are listing with gross revenues exceeding $3.6 million and EBITDA margins that make hospital CFOs envious.
But deals that look clean on a broker spreadsheet often carry financial landmines that don’t surface until after close. Reimbursement dependencies, equipment lifecycle surprises, physician referral concentration risk, and payer contract gaps can turn a profitable center into a cash drain within 18 months.
Florida Diagnostic Roadmap
This article walks through the most common pitfalls finance leaders encounter in Florida diagnostic center acquisitions, and the ROI levers that separate high-performers from average ones after the deal closes.
Why Florida Diagnostic Centers Are Attracting Serious Acquisition Interest
The demographics tell a compelling story. Florida’s 65-and-older population is growing faster than any other large state, and this cohort drives 70% of diagnostic imaging volume nationally. The shift from inpatient to outpatient care settings has accelerated post-pandemic, with commercial payers and CMS both incentivizing lower-cost site-of-service alternatives to hospital outpatient departments.
Established multi-modality centers in high-demand Florida markets regularly report net cash flows above $750,000 annually. When you factor in physician-owner retirement trends and private equity consolidation appetite, the pipeline of available deals is unusually strong right now.
Plan networks actively steered members toward freestanding diagnostic centers because the cost differential versus hospital outpatient imaging is substantial. A standard MRI that bills $2,200 at a hospital outpatient department often costs a plan $400-$600 at a freestanding center. That economics gap is not going away, which means patient volume at high-quality independent centers will continue to grow.
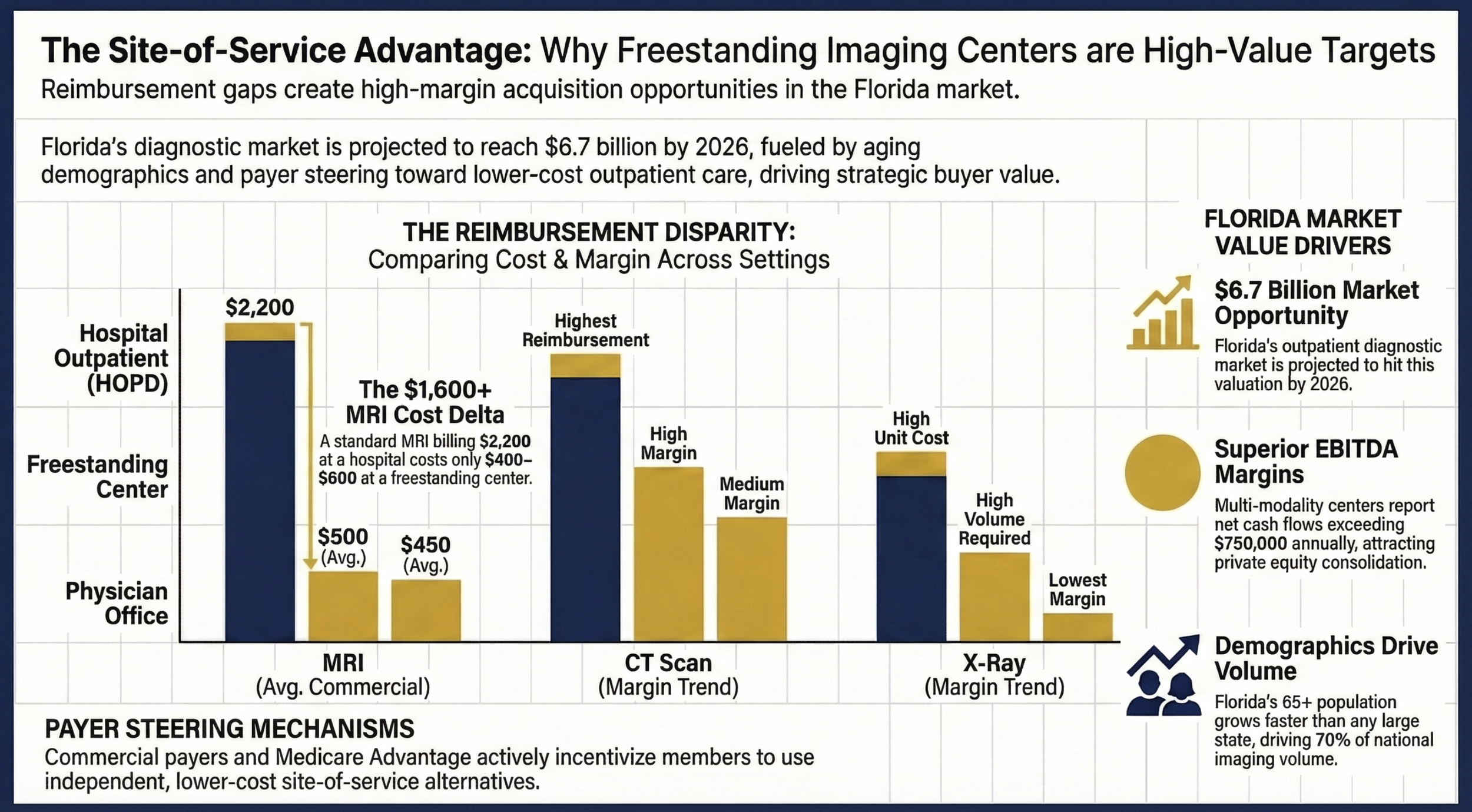
Site of Service Advantage: Why Freestanding Imaging Centers are High-Value Targets
Five Due Diligence Pitfalls That Can Sink Your ROI
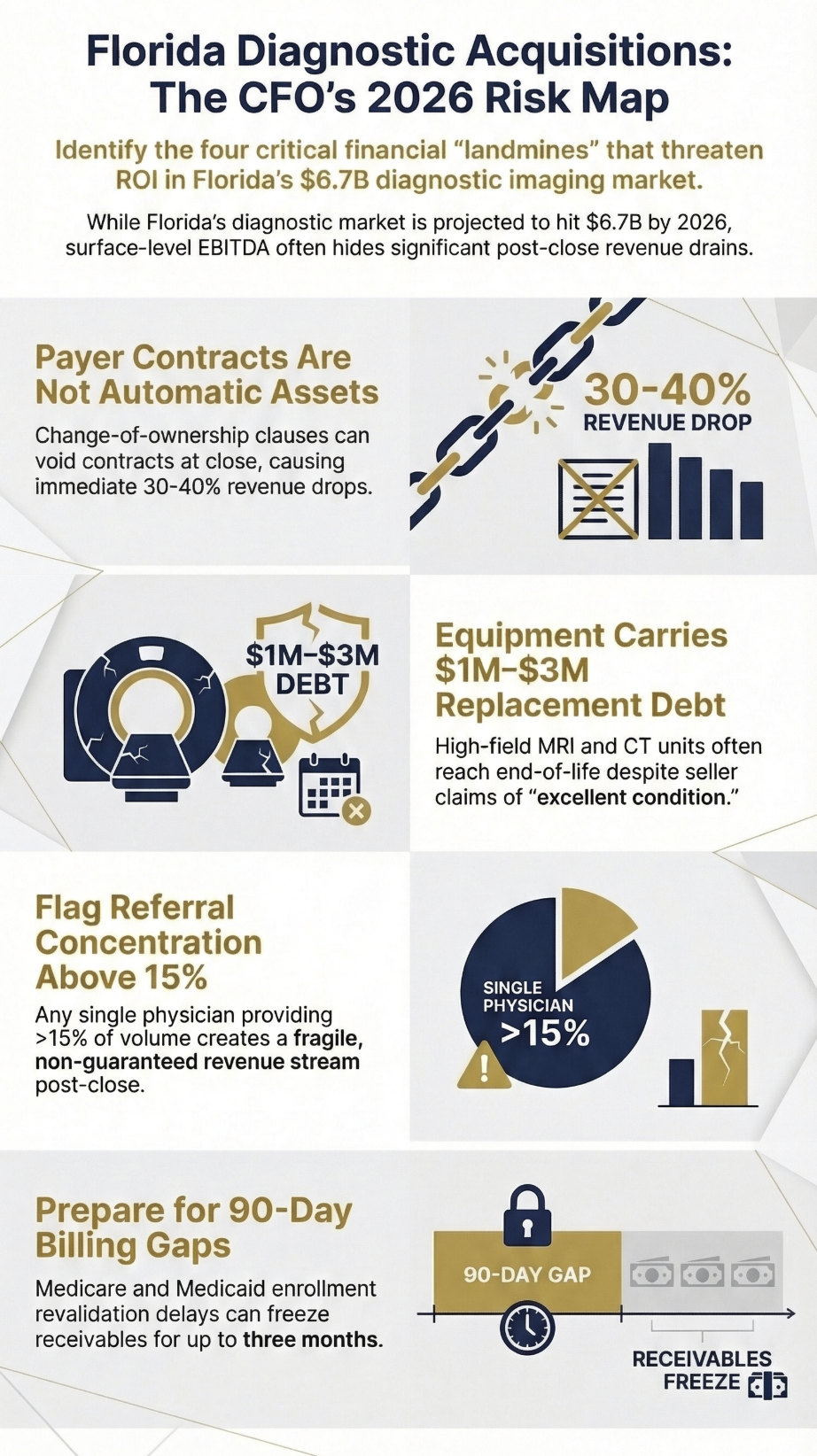
1. Payer Contract Transferability Is Not Guaranteed
This is the most overlooked risk in diagnostic center acquisitions, and it regularly blindsides buyers. When you acquire a practice, existing payer contracts do not automatically transfer to the new entity. Most insurance contracts include change-of-ownership clauses that require written payer approval, which can take 60 to 120 days and may result in modified reimbursement terms.
The risk: You close the deal in January, begin operating under the seller’s legacy contracts, and discover in March that two of your commercial payers have notified you that the old contracts are voided and you are now billing out-of-network. Revenue drops 30-40% overnight on those lives.
Before signing any letter of intent, request a contract-by-contract transfer analysis from legal counsel. Identify which payers represent more than 10% of revenue and begin informal outreach to those networks before close. Build a 90-day revenue protection buffer into your deal financing assumptions.
2. Equipment Condition and Replacement Timelines Are Frequently Misrepresented
High-field MRI equipment, CT scanners, and PET/CT systems carry replacement costs of $1 million to $3 million per unit, and the useful life claims on broker marketing materials often do not align with manufacturer maintenance records. A 1.5T MRI with 400,000 scans logged is functionally at end of useful life regardless of what the seller’s asset schedule says.
The standard seller pitch: “Equipment is in excellent condition, well-maintained, with several years of remaining life.”
What finance leaders actually face: Service contract costs increasing 15-20% annually, helium refill expenses that were deferred, and pending FDA software updates that require hardware upgrades.
Build an independent biomedical engineering assessment into your due diligence. Require the last three years of manufacturer service records. Then build a capital replacement reserve into your pro forma; at minimum, budget 5-8% of equipment replacement value annually.
3. Physician Referral Concentration Creates Fragile Revenue
Many freestanding diagnostic centers in Florida derive 40-60% of their volume from a small number of referring physician relationships. If those physicians are also part-owners who are selling, their post-close referral behavior is not contractually guaranteed. Restrictive covenant law in Florida is complex, and non-compete agreements in healthcare are subject to significant legal scrutiny.
Review 24 months of referral data by the ordering physician before you finalize valuation. Any single referral source representing more than 15% of revenue is a concentration risk that should either reduce purchase price or trigger a referral continuity agreement with holdback provisions tied to post-close volume performance.
4. Medicare and Medicaid Enrollment Gaps Delay Revenue
Revalidation and reassignment of Medicare billing privileges to a new legal entity is a step many buyers underestimate. CMS processing timelines for provider enrollment changes run 60-90 days on average, and during that window, Medicare claims cannot be submitted under the new entity’s billing information. Medicaid enrollment timelines in Florida vary by program but add additional complexity.
A center doing $1.5 million annually in Medicare revenue running a 90-day enrollment delay loses $375,000 in receivables timing. That is not a deal-killer, but it absolutely needs to be in your working capital calculation and your day-one cash flow model.
5. Stark Law and Anti-Kickback Compliance Exposure
Diagnostic imaging is one of the higher-risk Stark Law compliance areas because of the self-referral dynamics. Florida has a meaningful number of physician-owned diagnostic centers where the ownership structure has evolved organically and the compliance documentation has not kept pace. Any arrangement where referring physicians are also investors requires careful review under the in-office ancillary services exception or applicable Stark exceptions.
The red flag to look for: Sellers who are reluctant to produce complete physician ownership documentation, billing compliance audit histories, or Medicare cost reports. Undisclosed OIG investigations or prior settlements are material liabilities that should be uncovered in due diligence, not post-close.
Require a healthcare regulatory attorney review of all physician arrangements, managed care contracts, and any prior self-disclosure history before finalizing your deal structure.
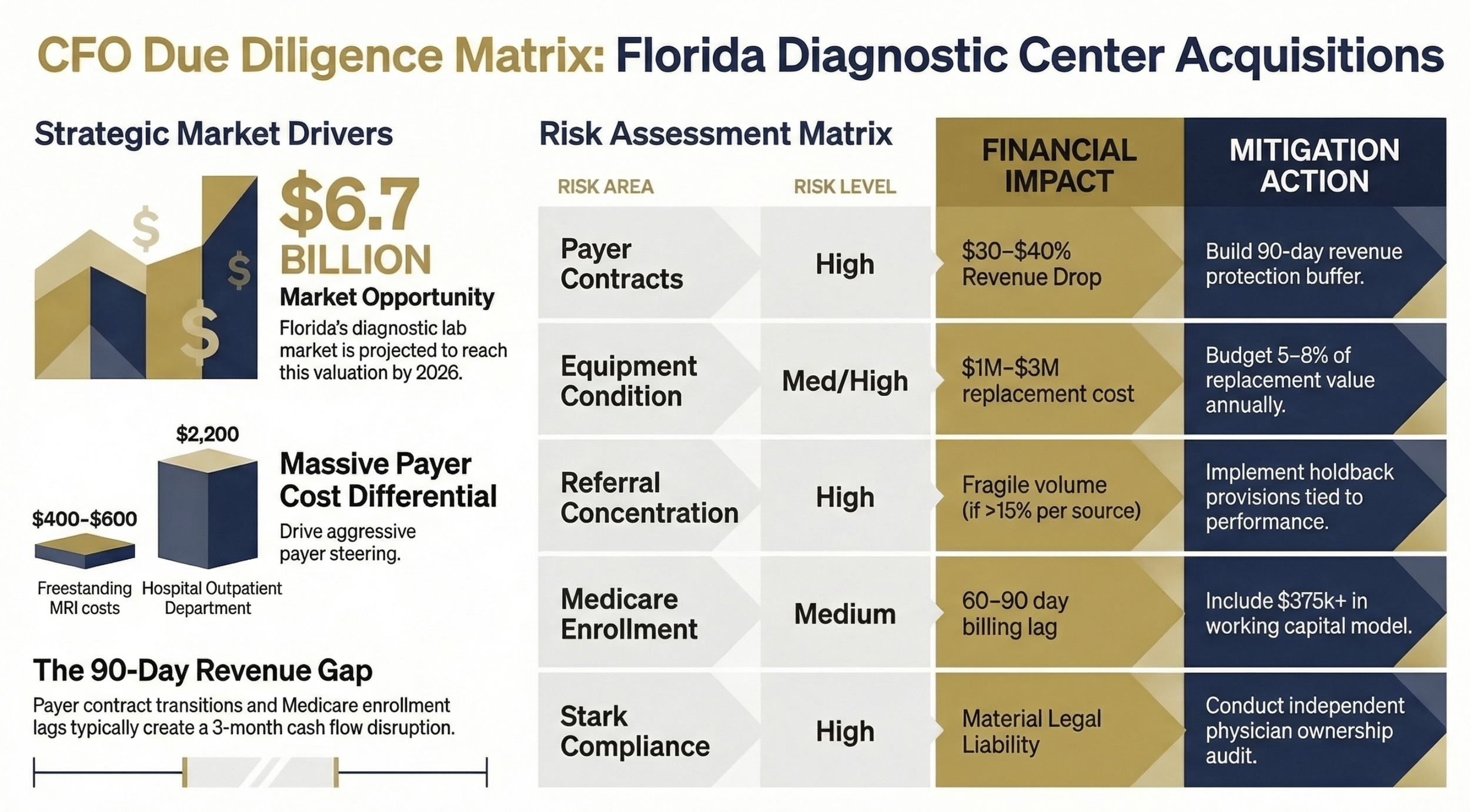
CFO Due Diligence Matrix: Florida Diagnostic Center Acquistions
Post-Acquisition ROI Levers That Actually Move the Needle
Payer Contract Renegotiation: Your First 90-Day Priority
Most acquired diagnostic centers have not renegotiated commercial payer rates in three to five years. The previous owner was either too busy, not financially sophisticated enough, or lacked the volume leverage that a new, potentially multi-location buyer can bring to the table.
Begin payer contract analysis on day one. Identify contracts where rates are 10% or more below Medicare comparable rates for high-volume codes (CPT 70553, 71250, 74178). A single payer renegotiation in Florida commercial markets can add $150,000 to $400,000 in annual net revenue for a mid-size center without adding a single patient.
Modality Mix Optimization
Not all imaging modalities are created equal from a margin perspective. MRI and PET/CT carry the highest reimbursement rates relative to technical cost. Plain film X-ray and low-complexity ultrasound have thin margins and high volume requirements to break even.
Review your modality utilization and scheduling data within the first 60 days. If you have MRI capacity running at 60% utilization and X-ray at 110%, you have a scheduling optimization opportunity. In my work at Ascension across seven hospitals, we found that rebalancing modality scheduling with predictive analytics tools consistently recovered 15-25% of revenue per imaging suite through throughput improvements alone.
Staffing Model: The Labor Cost Arbitrage Opportunity
Florida diagnostic centers often carry legacy staffing models built around the previous owner’s preferences rather than operational data. High overtime, underutilization of radiology technologist scope, and redundant administrative layers are common in owner-operated centers that have not been professionally managed.
A rigorous productivity analysis using industry benchmarks such as those published by MGMA and HFMA typically identifies 10-15% labor cost reduction opportunity in acquired centers within the first year without sacrificing quality metrics. Benchmark against 45-55 RVUs per technologist per day as a starting target for multi-modality environments.
The Multi-Location Synergy Play
Single-site diagnostic centers in Florida trade at 3-5x EBITDA. Multi-site platforms command 6-8x multiples from PE buyers. The acquisition math changes dramatically if you are building toward a platform play rather than a single asset hold.
If your strategy includes adding two or more locations, the ROI equation changes across every cost category. Shared payer contracting, consolidated billing operations, group purchasing for supplies and service contracts, and centralized interpretation services all contribute to margin improvement that a single-site analysis would never capture.
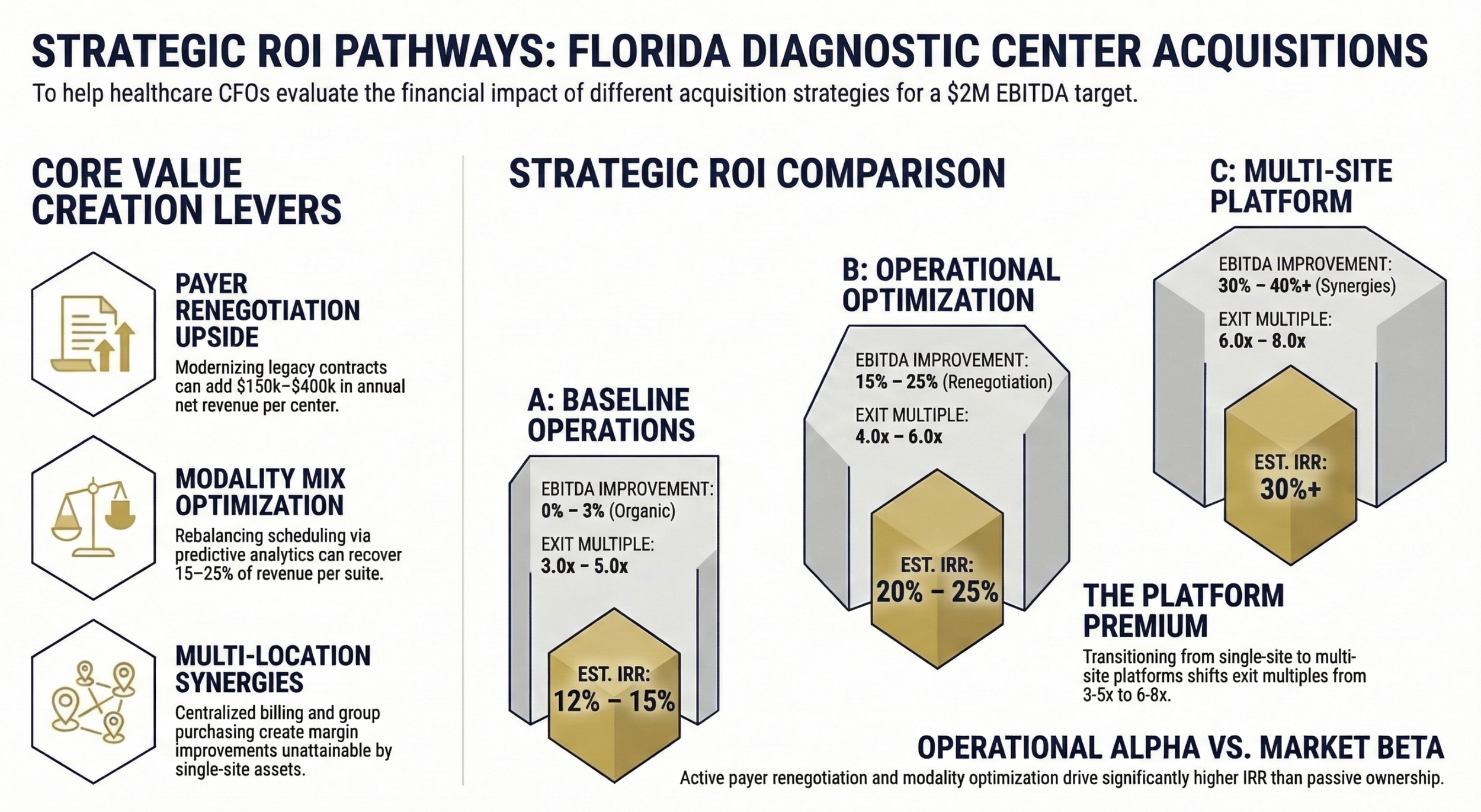
Strategic ROI Pathways: Operational vs Market
Building Your Acquisition Pro Forma: Key Assumptions to Stress-Test
A realistic acquisition model for a Florida diagnostic center should include scenario planning across at least three revenue assumptions.
Base case: Current revenue maintained with 3% annual growth, payer contracts unchanged for 12 months
Downside case: 15% revenue decline in year one from payer contract transition issues and referral disruption
Upside case: 10% volume growth from payer renegotiation, referring physician expansion, and modality optimization
Your working capital buffer should cover at a minimum 90 days of operating expenses, accounting for the Medicare enrollment gap and the lag between new payer contract effective dates and first payment receipt. Centers with heavy Medicare Advantage volume face additional complexity because MA plan contracts are separate from traditional Medicare billing relationships and require individual renegotiation.
Break-even analysis should be calculated at the payer contract level, not just the aggregate. If your three largest commercial payers represent 60% of revenue and all require contract renegotiation post-close, your revenue vulnerability window is substantially larger than your blended average would suggest.
"The difference between a good diagnostic center acquisition and a great one is almost always found in how thoroughly the finance team stress-tested payer contract continuity before the deal closed."
The Diagnostic Center Acquisition Due Diligence Checklist
Before signing any letter of intent, verify the following:
Payer Contracts:
Obtain all current payer contracts with effective dates and rate schedules
Confirm change-of-ownership notification requirements for each payer
Identify contracts representing more than 10% of revenue as critical path items
Begin informal network participation discussions with the top 3 payers pre-LOI
Equipment:
Commission an independent biomedical engineering assessment for all major equipment
Request manufacturer service records for the last 36 months
Calculate capital replacement reserve requirement (minimum 5-8% of replacement value annually)
Verify helium supply contracts and cryogen costs for MRI equipment
Revenue Integrity:
Review 24 months of referral data by ordering physician and practice group
Flag any single referral source above 15% of total volume
Request the last three years of billing audits and compliance review documentation
Verify all Medicare and Medicaid provider numbers are active and unrestricted
Compliance:
Obtain complete physician ownership documentation and investment arrangement history
Require healthcare regulatory counsel review of all Stark and Anti-Kickback exposure
Confirm no pending OIG investigations, prior settlements, or Medicare audits
Review all HIPAA compliance documentation and any prior breach notification history
Download the Diagnostic Center Acquisition Financial Model Template. I'm building this for Healthcare Finance Unfiltered subscribers. Reply to this email to get early access when it launches.
The Bottom Line for Finance Leaders
Florida outpatient diagnostic centers represent a genuine opportunity for health systems, physician groups, and independent finance-savvy buyers looking for high-margin, high-demand assets in a growing market. But the acquisition landscape in 2026 requires more diligence than it did three years ago.
Payer contract transferability, equipment capital requirements, referral concentration, and compliance exposure are not secondary concerns you address post-close. They are the deal-defining variables that determine whether you are buying a cash flow engine or an operational turnaround.
The finance leaders who win in this space are the ones who stress-test revenue at the payer contract level, build realistic working capital buffers, and enter negotiations with a clear post-close value creation roadmap rather than just a purchase price rationale.
P.S. If you are actively evaluating a diagnostic center acquisition in Florida, I want to hear about it. What is the single biggest financial concern you are navigating right now? Hit reply and tell me. I read every response and your questions directly inform future articles.