
AI in Revenue Cycle Management: The Enterprise Implementation Framework Healthcare CFOs Need in 2026
82% of organizations now call AI integral to RCM. The ones building lasting ROI treat it as an operating model investment, not a software purchase.
Healthcare organizations spent 2024 and early 2025 piloting AI in revenue cycle. The results looked promising in controlled settings. Now the bill is coming due, and finance leaders are discovering that the gap between a successful pilot and enterprise-scale ROI is wider than any vendor projected.
The differentiator is not the technology. It is whether your organization redesigned how work flows before deploying the technology to accelerate it.
Why AI-Powered RCM Is No Longer Optional
Eighty-two percent of healthcare leaders now report that AI is an integral part of their revenue cycle operations, with 70% categorizing it as a high or critical organizational priority. Prior authorization automation alone is expected to have the biggest operational impact of any AI application in 2026, according to survey data from revenue cycle leaders across the country.
These numbers matter for a specific reason. Your competitors are already deploying this infrastructure. The question is no longer whether to invest in AI-powered RCM. It is whether your investment will generate the returns you need to justify the capital allocation.
The finance leaders who are getting this right share one characteristic: they stopped treating AI as a technology implementation and started treating it as an enterprise operating model redesign.
CFO’s Enterprise AI in RCM framework design
The Framing That Changes Everything
Leaders from Mayo Clinic and Jefferson Health offered the clearest articulation of this shift at the ViVE digital health conference in early March 2026. Their organizations are among the early health systems that have moved AI from pilot to enterprise scale, and the lesson they drew is not about which AI platform to select.
Patricia Henwood, MD, Chief Clinical Officer at Jefferson Health, described it this way: revenue cycle leaders need to map how work actually moves across the enterprise, from scheduling and authorization through coding, billing and payment, and then align decision rights and performance metrics accordingly. The technology comes after the workflow redesign, not before.
"If you think only AI technology is going to be the solution, you're wrong," she said.
Mayo Clinic's COO Maneesh Goyal reinforced this point from a governance perspective. Revenue cycle processes are interconnected in ways that most organizations treat as separate workstreams. The way AI implementations get deployed in individual departments without coordinated enterprise logic creates exactly the fragmentation that prevents ROI from materializing.
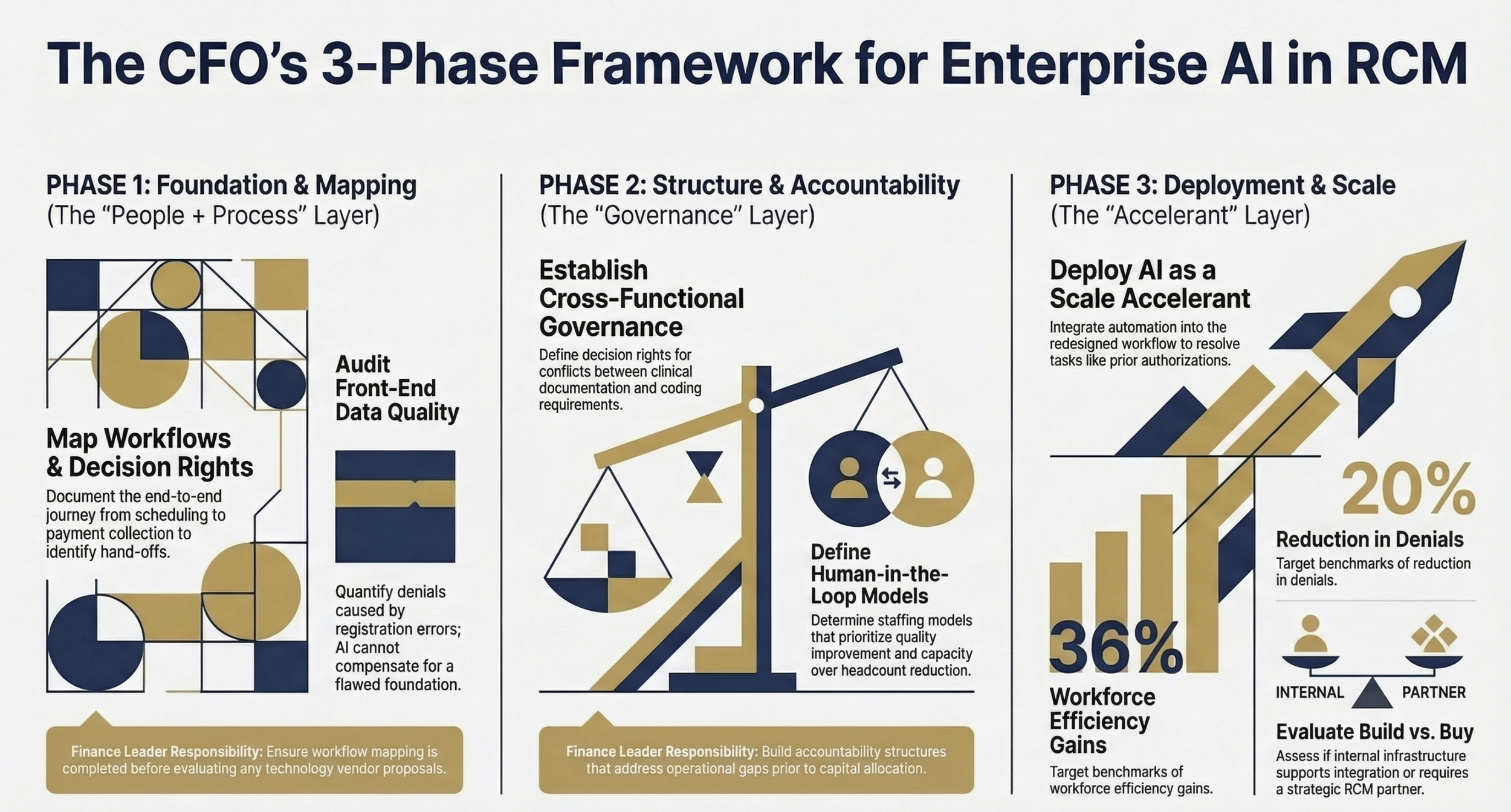
CFO’s Framework for Enterprise AI in RCM includes People & Process Layer, Governance, and Accelerant layers
What the ROI Data Actually Shows
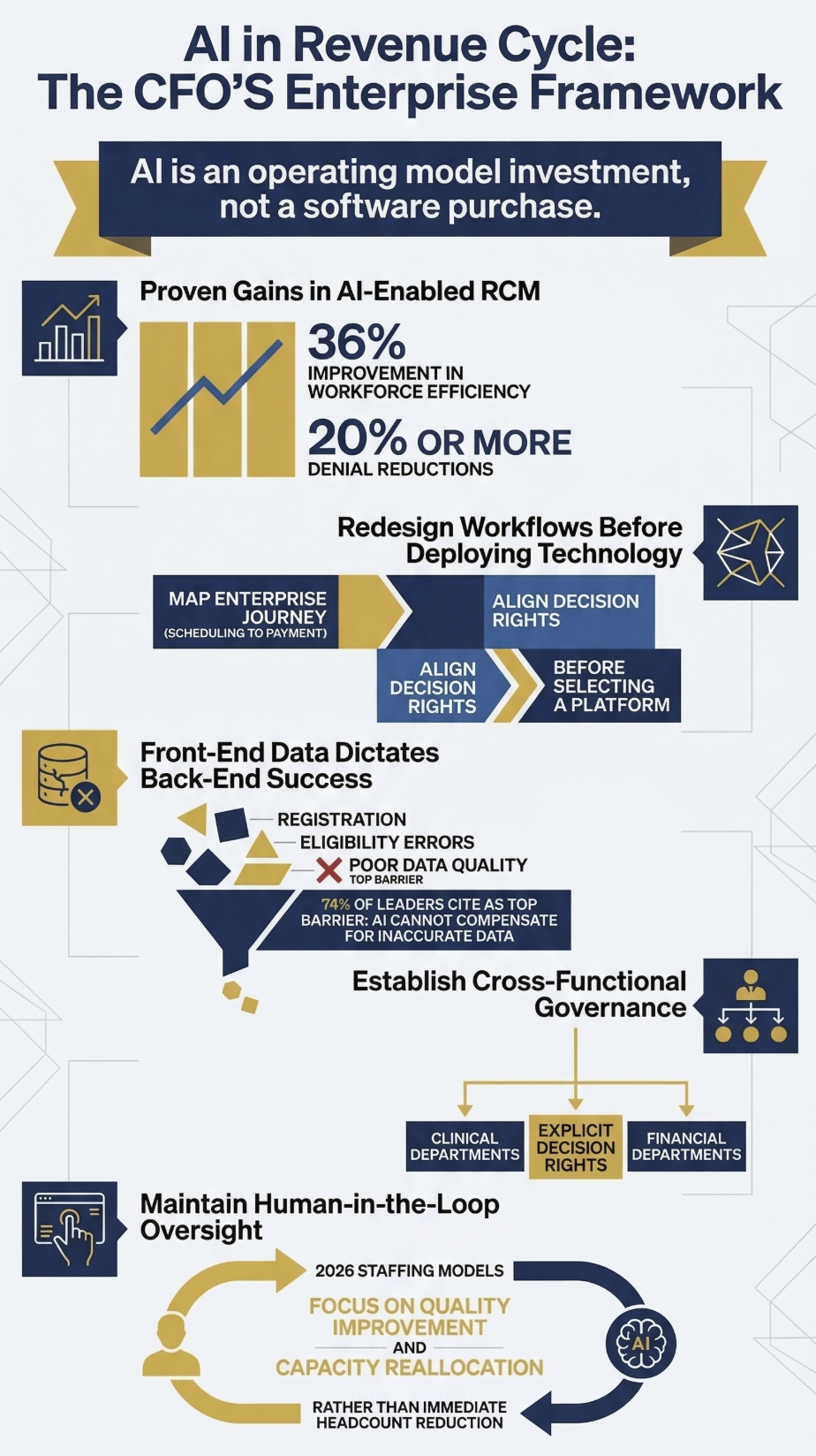
The benefit data for AI in RCM is real. Organizations that have deployed AI-powered tools at scale report a 36% improvement in workforce efficiency, a 37% improvement in patient experience and collections outcomes, and denial reductions of 20% or more. Prior authorization automation, autonomous coding, and predictive denial management are delivering measurable returns in organizations with the operational infrastructure to support them.
The problem is that most organizations deploy AI into existing workflows without addressing the structural conditions that determine whether the technology can deliver. This produces a frustrating pattern: the pilot works because a small team with dedicated focus executes it well. The enterprise rollout underperforms because the underlying workflow fragmentation and governance gaps that the pilot bypassed now limit scale.
From my work at Ascension tracking productivity metrics across seven hospitals, I watched this dynamic play out repeatedly with technology implementations that were not AI-related but followed the identical pattern. The technology was sound. The operational conditions were not designed to sustain it at scale.
The finance leader's job is to assess both dimensions before approving capital, and to build accountability structures that ensure operational conditions are addressed before technology deployment begins.
The Three Barriers Finance Leaders Must Address First
The data on AI implementation barriers is telling. Fifty-one percent of organizations cite limited IT infrastructure as the biggest obstacle. Forty-four percent cite budget constraints. Forty-three percent cite integration challenges. These are technology and capital barriers that finance leaders are accustomed to evaluating.
The barrier that gets underweighted: 74% of revenue cycle leaders say poor data quality is a critical barrier to AI success. This is not an IT problem. It is an operational discipline problem that finance leaders must drive.
Front-end data quality is the foundation. The current trend in AI-enabled RCM is a significant shift toward front-end investment, specifically patient registration, insurance verification, and eligibility confirmation. Organizations are discovering that back-end claims scrubbing powered by AI cannot compensate for front-end data errors. When insurance verification is incomplete or registration data is inaccurate, AI-powered coding and billing tools are working from a flawed foundation.
This has a direct financial implication. If your organization is evaluating AI for denial management or autonomous coding, the single best predictor of whether that investment will generate projected returns is the quality of your front-end data capture. Finance leaders who evaluate AI vendors without auditing their front-end data quality are approving capital based on projections that will not materialize.
Governance architecture determines enterprise performance. Mayo Clinic's emphasis on governance reflects a structural reality. Revenue cycle decisions cascade into individual departments and subspecialties across the organization. When AI tools are deployed in billing without alignment to changes in coding workflows, or when prior authorization automation is implemented without corresponding adjustments to clinical documentation expectations, the technology creates new fragmentation rather than resolving existing fragmentation.
Finance leaders need to ensure that AI implementation plans include cross-functional governance with explicit decision rights, not just a project management structure that coordinates timelines.
Human oversight remains non-negotiable in 2026. Agentic AI, tools that do not just recommend actions but actively resolve tasks including payer website searches, coding decisions, and prior authorization submissions, is expanding rapidly. Seventy-three percent of organizations believe prior authorization automation will have the largest impact of any AI application in the near term.
But 2026 strategy across leading organizations still emphasizes human-in-the-loop oversight for AI-generated outputs. The finance implication is that staffing models for AI-enabled RCM should not assume headcount reduction as the primary return driver in years one and two. The near-term return is quality improvement and capacity reallocation, not elimination.
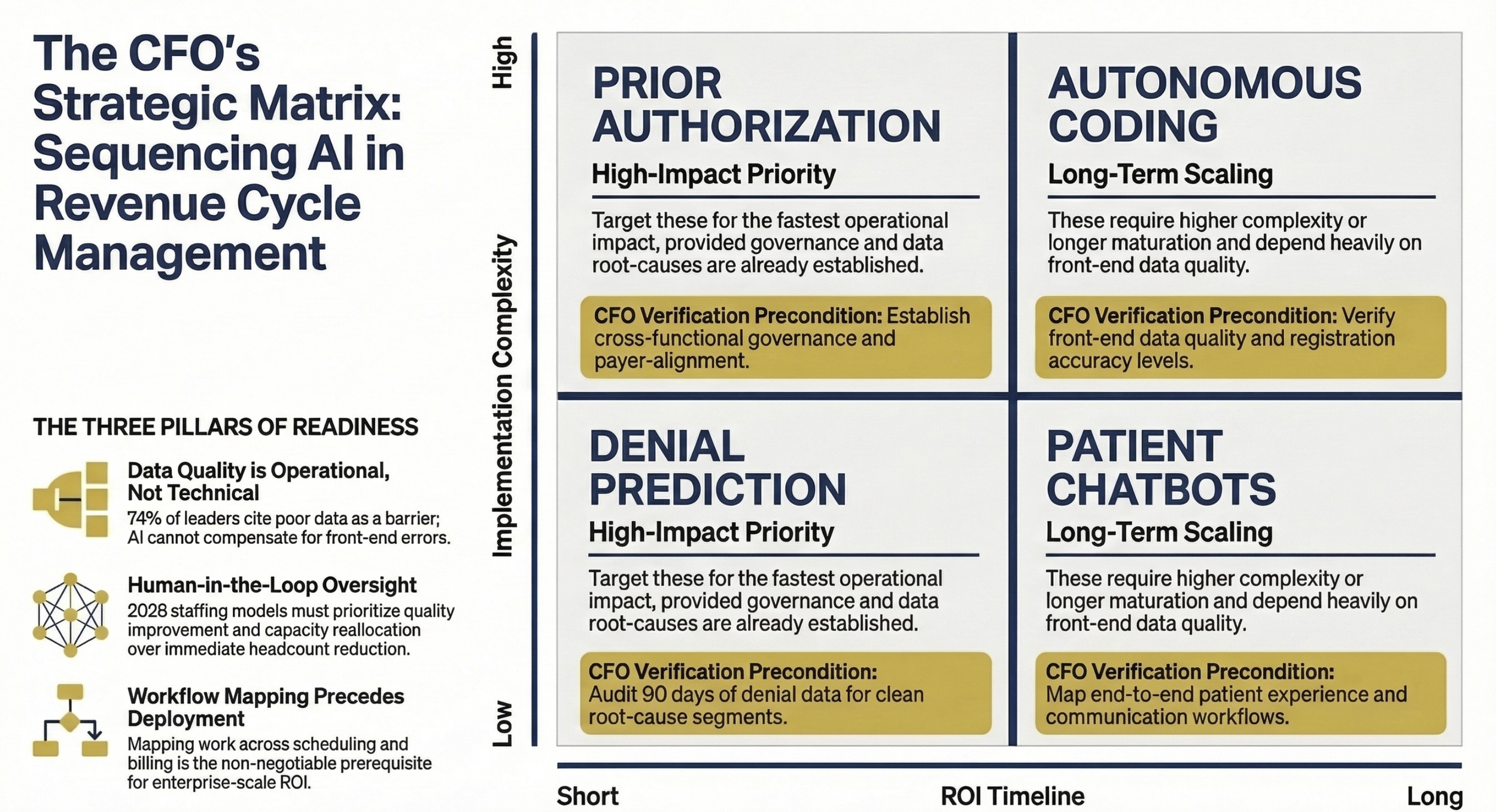
Four-quadrant matrix plotting AI application types (prior authorization, autonomous coding, denial prediction, patient financial chatbots) against two axes: implementation complexity (low to high) and ROI timeline (short to long).
Building the Long-Term Investment Case
The shift happening in 2025-2026 is toward AI becoming standard, unnamed infrastructure in revenue cycle operations. Experts predict that by 2026, leading organizations will no longer discuss AI as a separate initiative. It will be built into how revenue cycle operates, similar to how electronic claims submission is no longer a technology investment discussion.
This trajectory has two implications for long-term financial planning.
First, the question is not whether to invest but how to sequence investment to build cumulative capability rather than disconnected point solutions. The organizations currently generating the strongest AI-enabled RCM returns are those that built foundational data infrastructure first, deployed AI in highest-impact areas second, and have a multi-year roadmap that adds capability incrementally as operational maturity increases.
From my perspective working in Medicare Advantage operations at Florida Blue Medicare, the payer side of this equation is equally relevant for provider finance leaders to understand. Payers are deploying AI in prior authorization and utilization management at scale. The WISeR model CMS launched in early 2026 is the federal government's version of AI-driven utilization management. Provider organizations that have not built AI-enabled RCM capability to respond to AI-enabled denial generation are entering an asymmetric operational environment.
Second, strategic outsourcing is becoming a viable long-term option for organizations that cannot build enterprise AI capability internally. The market is consolidating around AI-enabled RCM platforms, including the recent formation of Smarter Technologies combining SmarterDx, Thoughtful.ai, and Access Healthcare into a comprehensive platform. For health systems with limited IT infrastructure, partnering with an AI-capable RCM vendor may generate better returns than internal implementation. Finance leaders need to evaluate build versus buy with the same rigor applied to any major capital decision.
If you are currently working through an AI vendor evaluation or building the internal business case for AI-enabled RCM investment, I want to hear what you are running into. Hit reply and tell me where the process is stalling.
The CFO Decision Framework
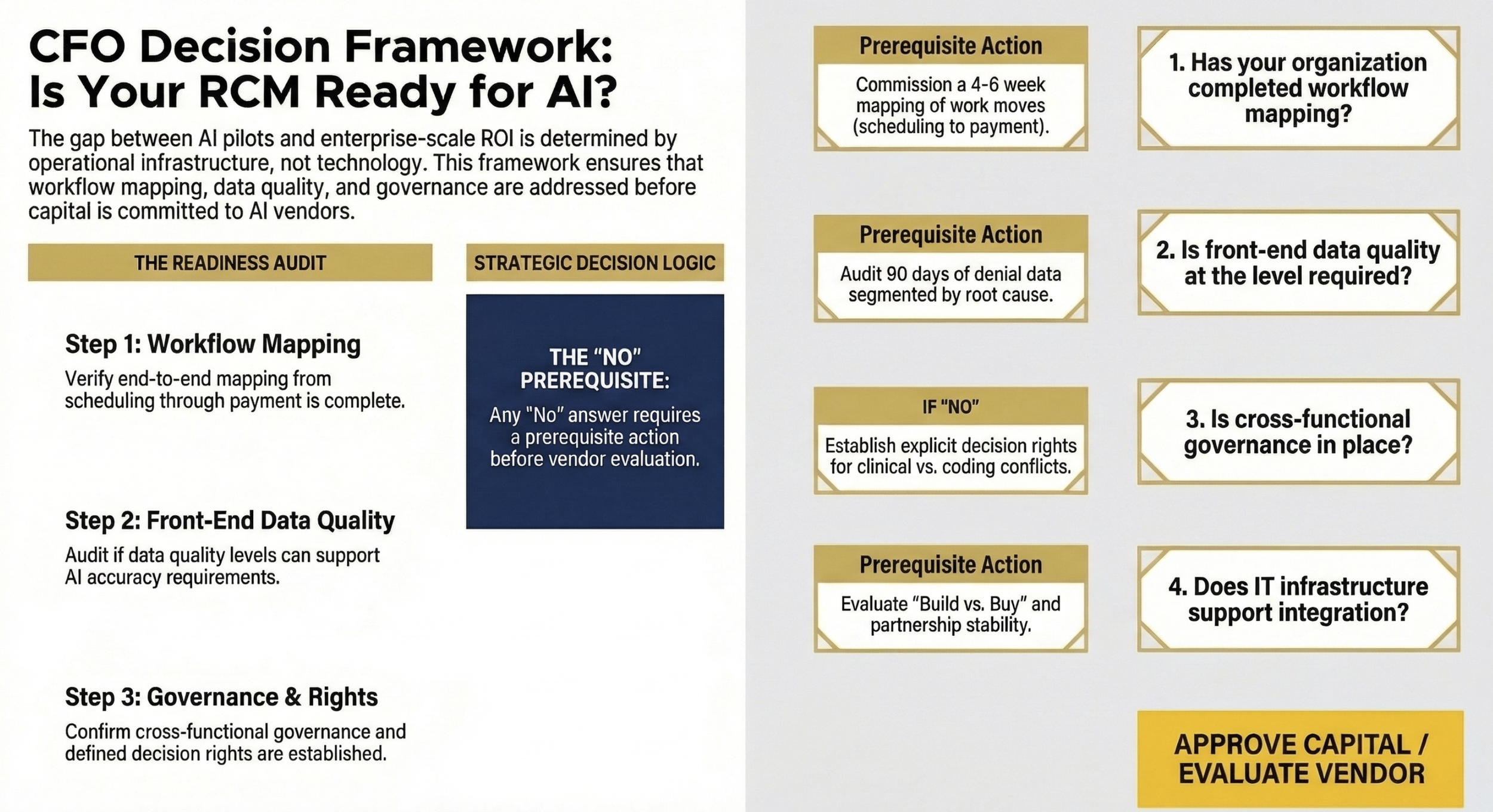
CFO AI-in-RCM decision framework with four sequential questions. (1) Has your organization completed workflow mapping from scheduling through payment? (2) Is front-end data quality at the level required to support AI accuracy? (3) Is cross-functional governance in place with defined decision rights? (4) Does your IT infrastructure support integration requirements? Each "No" answer leads to a prerequisite action before proceeding to vendor evaluation.
Before approving capital for AI-enabled RCM, finance leaders should require answers to four specific questions.
What is the current state of front-end data quality? Request denial data segmented by root cause. If a significant percentage traces to front-end registration errors, start there before investing in back-end AI.
What workflow redesign is planned before deployment? Any vendor proposal that does not include a workflow mapping and redesign phase should be treated as a point solution, not an enterprise investment. Understand what that distinction means for projected returns.
What governance structure will manage cross-functional alignment? Identify who has decision rights when clinical documentation expectations conflict with coding requirements, or when scheduling workflow changes affect authorization outcomes. If there is no clear answer, the governance infrastructure is insufficient.
What is the human oversight model? Understand what percentage of AI-generated outputs will be reviewed by staff, what the escalation path is when AI recommendations conflict with clinical judgment, and how accuracy will be measured and reported to finance leadership.
The organizations generating 20% denial reductions and 36% efficiency improvements did not achieve those outcomes by purchasing better software. They achieved them by treating AI deployment as the final step in an enterprise redesign, not the first.
As we covered in Revenue Cycle Management in 2026 the deeper problem in most revenue cycle operations is not process efficiency. It is that reimbursement assumptions and operational models have not kept pace with market changes. AI does not solve that problem. But when the underlying operational model is sound, AI is the most powerful tool available to scale it.
What to Do in the Next 90 Days
If your organization has not yet moved AI from pilot to enterprise planning, the sequencing below reflects how leading organizations have approached it.
Audit front-end data quality first. Pull 90 days of denial data and segment by root cause. Quantify what percentage of denials trace to front-end data errors versus back-end coding or billing issues. This tells you where AI investment will have the highest return.
Commission a workflow mapping exercise. Map how work actually moves from scheduling through payment collection, including where hand-offs occur, who has decision authority at each step, and where the current process creates rework. This takes four to six weeks and is the prerequisite for any enterprise AI implementation.
Evaluate build versus buy with long-term criteria. Assess whether your internal IT infrastructure and governance can support enterprise AI implementation, or whether an AI-enabled outsourcing partner is the better strategic option. Consider the consolidation happening in the RCM vendor market and what it means for partnership stability.
For related context on how to structure ROI analysis for technology investments in revenue cycle, see Why Your Revenue Cycle ROI Calculations Are Probably Wrong. For the broader technology spending accountability framework, see The Real Cost of Healthcare IT.
The Bottom Line
AI in revenue cycle has crossed from experimental to essential. The organizations generating real returns are not the ones that bought the most sophisticated tools. They are the ones that did the organizational work first.
The finance leader's role in this transformation is not to evaluate software. It is to ensure the operational preconditions are in place before capital is committed, and to build governance infrastructure that holds the enterprise accountable for delivering projected returns.
If your organization is deploying AI in RCM or preparing to, subscribe to Healthcare Finance Unfiltered for the frameworks and analysis your team needs to build the business case and manage the implementation. The next 12 months will determine which organizations have built sustainable AI-enabled revenue cycle operations and which ones have expensive software running in fragmented processes.