
Rural Health Transformation Program 2026: CFO and CIO Guide to Winning EHR/ERP Grant Funding
The OBBBA's $50B rural health fund is your window to fix long-deferred EHR problems. Here's how to build a winning bid before the 2028 redistribution clock starts.
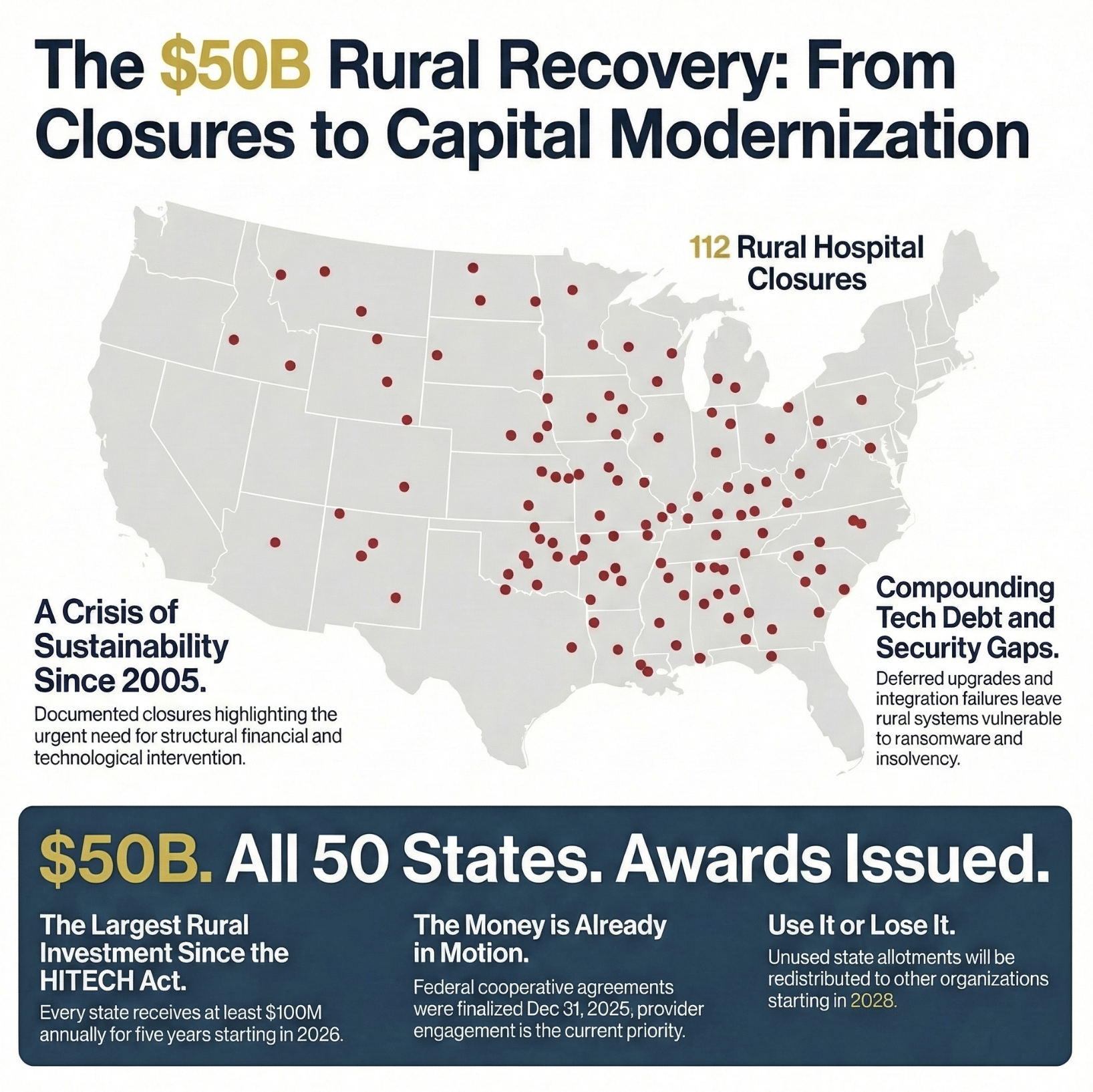
The Rural Health Transformation Program just handed rural CFOs and CIOs the largest technology funding opportunity since the HITECH Act. Fifty billion dollars. Five years. No state match required. And unlike HITECH's scramble a decade ago, this program gives rural health systems the flexibility to fix the right problems instead of just racing to check a compliance box.
Here's what changed at year-end: CMS already awarded all 50 states their RHT Program cooperative agreements by December 31, 2025. The state application window is closed. The funding is allocated. What hasn't happened yet is the provider-level engagement that determines which rural hospitals actually receive those funds and for what purposes.
Beginning in 2028, unused state allotments get redistributed. If your system isn't engaged in your state's implementation planning right now, you could watch this funding flow to better-positioned organizations while your aging EHR limps through another budget cycle.
The state money is in the door. The question is whether you're at the table when your state decides how to deploy it.
Why the RHTP Is Different From Every Rural Funding Program That Came Before
Rural hospitals have been promised federal lifelines before. The Medicare Modernization Act created Critical Access Hospital designations. The Flex Program provided operational support. HRSA grants funded specific initiatives. Most of that funding addressed symptoms rather than root causes, and very little of it touched the technology infrastructure that determines whether a rural hospital can actually operate efficiently.
The Rural Health Transformation Program, embedded in the One Big Beautiful Bill Act, operates differently in three ways that matter to finance leaders.
First, the funding is substantial. Each state receives at least $100 million annually for five years. Half of the $50 billion was divided equally among all 50 participating states. The other half flows through a formula that weights rural population, proportion of healthcare facilities in rural areas, and hospitals serving high proportions of low-income patients. States with large rural populations and heavy safety-net burdens received significantly more than $100 million annually.
Second, the allowable uses explicitly include technology infrastructure. The legislation authorizes spending on training and technical assistance for technology-enabled solutions, including remote monitoring, robotics, and artificial intelligence. It authorizes software and hardware for significant information technology advances. It explicitly names cybersecurity capability development. States must deploy funds across three or more of the approved use categories, which means every state implementation plan includes at least some technology component alongside clinical and workforce priorities.
Third, states design their own implementation plans. The federal government does not mandate specific technology choices or vendor relationships. CMS has published state project abstracts — summaries of what each state committed to when applying — so rural hospitals can actually look up what their state prioritized before walking into any conversation with state officials. That is a significant advantage most rural CFOs and CIOs haven't yet used.
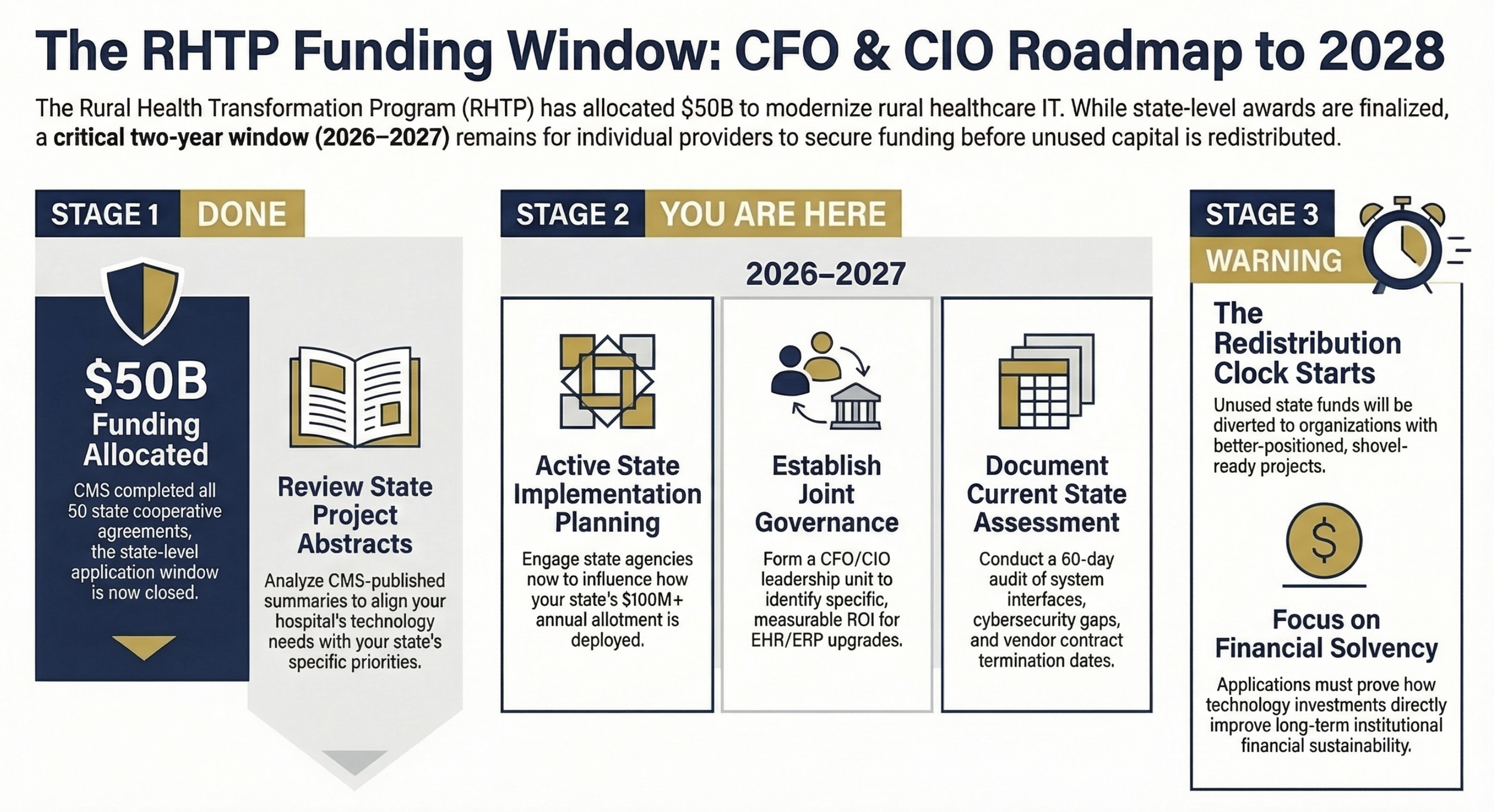
Key CFO/CIO action steps under each stage. Purpose: Reorient readers to the actual current moment — state awards are finished, provider-level engagement is the active window before 2028 redistribution
The EHR Problem Rural Hospitals Have Actually Been Living With
Before building a grant strategy, finance and technology leaders need an honest assessment of what they're actually trying to fix. Rural hospital EHR and ERP challenges are not the same as the problems large health systems face, and conflating them leads to grant applications that sound generic and lose to more specific proposals.
In my experience reviewing technology operations across multi-hospital systems, the most consistent rural technology failures cluster around three problems.
Deferred upgrades that compound over time. A Critical Access Hospital that implemented an EHR in 2012 using HITECH funding may be running a version that the vendor no longer actively supports. Patches get applied. Workarounds get built. Clinical staff develop shadow systems in spreadsheets because the EHR can't do what they need it to do. The cost of the deferred upgrade feels prohibitive every budget cycle, so it gets deferred again.
Integration failures between clinical and financial systems. Many rural hospitals operate their EHR and their ERP as parallel, largely disconnected systems. Charge capture flows from clinical documentation to billing, but cost accounting, productivity tracking, and supply chain management operate in separate platforms with manual reconciliation. Finance teams spend hours weekly moving data between systems that should talk to each other automatically. This isn't an inefficiency. It's a structural barrier to the kind of financial visibility that allows a rural CFO to make sound strategic decisions.
Cybersecurity vulnerabilities from outdated infrastructure. Rural hospitals are among the most targeted healthcare organizations for ransomware attacks precisely because aging systems lack modern security architecture. The RHTP explicitly identifies cybersecurity capability development as an allowable use. This framing matters: cybersecurity isn't just an IT problem. A ransomware attack at a sole-community provider creates a patient care crisis that directly translates into financial and liability exposure for the organization.
If you want to read more about how EHR vendor relationships create structural financial risk, I covered the Epic interoperability and contract leverage problem in depth here: Epic's Interoperability Crisis: What Healthcare Finance Leaders Need to Know About Contract Leverage and Strategic Risk. The dynamics that apply to large systems also play out, often more severely, at smaller rural organizations with less negotiating leverage.
Start Here: Governance Before Technology
The instinct when new funding becomes available is to call the EHR vendor, request a proposal, and start budgeting. That instinct leads to failed implementations.
Every successful EHR upgrade at a resource-constrained organization starts with governance, not technology selection. Governance means establishing who makes decisions, what problems those decisions are solving, and how success will be measured. Without governance, you will purchase an upgraded system and discover 18 months into implementation that clinical staff, finance staff, and IT staff each had a different vision of what the new system was supposed to do.
A rural CFO and CIO building a grant-eligible technology improvement plan need to answer these questions before any vendor conversation happens.
Who owns the project? At rural hospitals, the CFO and CIO frequently operate as the same person, or as two people with overlapping responsibilities and limited staff. For a technology project funded by a state RHTP grant, you need a named executive sponsor with authority to make decisions, a clinical champion who represents provider and nursing workflow needs, and a finance champion who owns the ROI framework and budget accountability. These can be the same two or three people. They cannot be undefined.
What problems are you solving? "Our EHR is old" is not a problem statement. "We lose 90 minutes per provider per day to documentation because our EHR doesn't support ambient capture" is a problem statement. "Our charge capture failure rate is 3.2% because the EHR and billing system don't integrate" is a problem statement. Specific, measurable problem statements make grant applications credible and make vendor contracts enforceable.
What does success look like in three years? Grant applications that win include measurable outcome commitments. Not "improve efficiency" but "reduce average length of stay by 0.4 days through better discharge planning workflow." Not "enhance cybersecurity" but "achieve SOC 2 Type II certification and eliminate the three legacy systems currently excluded from our security monitoring platform." Specificity wins funding. Vagueness loses it.
Current State Documentation: The Work Nobody Wants to Do
Once governance is established, the next step is the one most organizations skip: rigorous current state documentation. You cannot write a compelling grant application, select the right vendor, or negotiate an enforceable contract without an honest picture of where you are today.
Current state documentation for an EHR/ERP upgrade should capture: every system currently in production, who built each interface between systems, what data moves through each interface and how often, where manual reconciliation replaces automated data flow, what your total annual IT spend is by system, and what your current support contract terms are including termination clauses and renewal dates.
That last item matters more than most CFOs realize. A rural hospital with an EHR contract that auto-renews in 90 days on unfavorable terms cannot negotiate effectively with the incumbent vendor or credibly threaten to switch. Before engaging any vendor in technology upgrade conversations, know your contractual position.
For the ERP side of the equation, document your current chart of accounts structure, what cost accounting methodology you're using, whether your productivity reporting integrates with clinical data or operates separately, and what financial reporting you cannot currently produce because your systems don't support it. This last item often generates the clearest picture of what a new system needs to deliver.
Future State Vision: What the Grant Application Actually Needs to Say
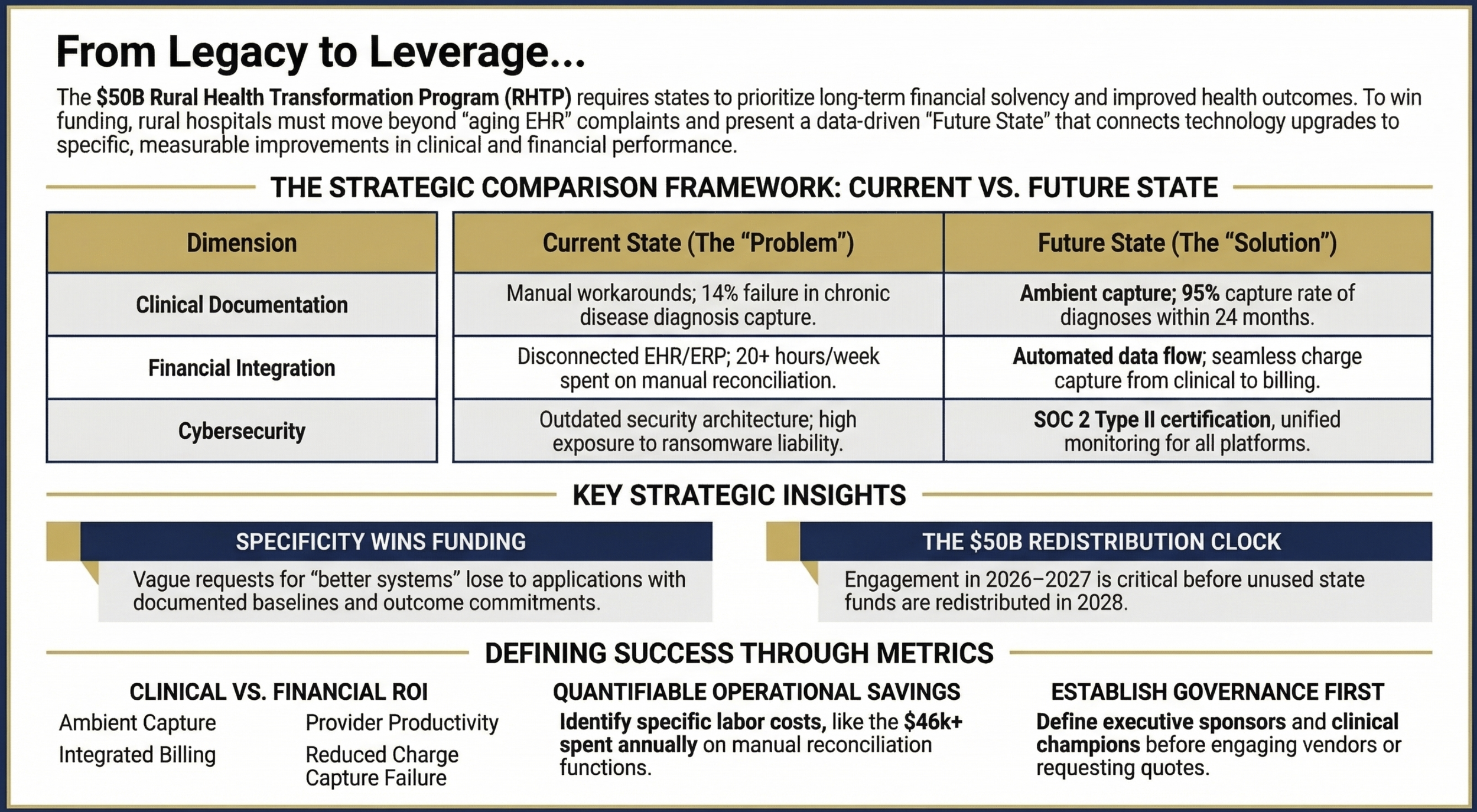
Type: Side-by-side comparison table Content: Current State vs. Future State across five dimensions — Clinical Documentation, Charge Capture Integration, Financial Reporting, Cybersecurity, and Workforce Productivity — with specific metrics in each cell Purpose: Show CFOs/CIOs the framework structure that makes grant applications concrete and evaluable
State RHTP plans must describe how funds will improve access, improve health outcomes, prioritize technology that supports prevention and chronic disease management, and outline strategies for long-term financial solvency. Your technology upgrade proposal needs to connect directly to these required plan elements.
The connection that wins grant funding is not "we need a better EHR." It is: "Our current clinical documentation system fails to capture 14% of diagnoses relevant to chronic disease management in our patient population. We cannot measure care gaps, generate quality reports required for value-based care arrangements, or identify patients due for preventive screenings. A modernized EHR with embedded clinical decision support and care gap identification will allow us to document, report, and act on 95% of chronic disease diagnoses within 24 months of implementation."
That framing connects a technology investment to a patient outcome. It gives the state a measurable commitment to hold you accountable to. And it positions your organization as a serious steward of public funds rather than a hospital using grant money to solve a vendor relationship problem.
I covered the broader framework for evaluating healthcare technology ROI in AI Medical Scribes: The ROI Case Healthcare Finance Leaders Need Before Budget Season. The ROI framework structure translates directly to EHR upgrade proposals: define the baseline problem with measurable data, project the specific improvement with reasonable assumptions, and identify the monitoring metrics that will confirm whether the investment delivered.
The CFO/CIO Collaboration Framework for Grant Execution
Rural hospitals where the CFO and CIO work in silos lose to rural hospitals where they work as a unit. Grant applications that separate the financial case from the technology case signal to state evaluators that the organization doesn't have integrated leadership.
Here is what effective CFO/CIO collaboration looks like for an RHTP technology grant application.
The CFO owns the financial model. This includes the total cost of ownership for the proposed technology solution, the projected operational savings from reduced manual processes and better charge capture, the return on investment timeline, and the budget framework that demonstrates the organization can absorb implementation costs not covered by grant funding. The RHTP does not require state matching funds, but implementation always costs more than the software. Staff training time, workflow disruption, temporary productivity loss, and third-party implementation support all represent real costs that need to be in the financial model.
The CIO owns the technical architecture. This includes the current state infrastructure assessment, the proposed future state architecture, the implementation timeline and milestones, the vendor evaluation framework, and the security and data governance requirements that any proposed solution must meet. For rural hospitals without a dedicated CIO, this role often falls to an IT director or a contracted technology advisor. If your organization doesn't have internal technology leadership with implementation experience, budget for external project management before you talk to any vendor.
Both leaders own the vendor selection process jointly. Vendor demos that only involve IT staff produce technology that finance can't use. Vendor demos that only involve finance staff produce contracts that IT can't implement. Every vendor evaluation should include: a structured demonstration of financial reporting capabilities, a review of the implementation methodology and timeline, reference calls with comparable rural organizations that have completed implementation, and a detailed review of the contract terms including data ownership, termination rights, and price escalation provisions.
The three major EHR vendors serving rural markets each have distinct positioning. Epic dominates the large health system market and has made meaningful rural investments, but implementations at small rural hospitals require expensive consulting support and long timelines. Cerner (now Oracle Health) has historically had broader rural presence and more flexible deployment models, but has faced integration challenges post-Oracle acquisition. Mid-market vendors like athenahealth, MEDITECH, and TruBridge are purpose-built for smaller organizations and often deliver faster implementation timelines at lower total cost.
For a detailed look at the financial risk embedded in vendor relationships with the major EHR players, The Real Cost of Healthcare IT: Who's Getting Rich While Patients Get Broke walks through how large technology relationships extract value from health systems that don't negotiate from informed positions.
Building a Winning Grant Bid: What the State Evaluators Are Looking For
State RHTP plans need to address rural financial solvency as one of their required elements. Technology proposals that demonstrate a direct connection between the investment and the hospital's long-term financial viability will rank above generic technology improvement proposals.
Your grant application should include three components beyond the basic project description.
A financial sustainability narrative that quantifies the problem. If your current system costs $400,000 annually in maintenance and produces reports that require 20 hours weekly of manual reconciliation at a blended cost of $45 per hour, that's $46,800 annually in manual labor for one function. If a modern integrated system eliminates that manual reconciliation, that's a documented operational saving that contributes to your financial sustainability case.
A workforce plan that addresses the implementation reality. Grant applications that acknowledge rural workforce constraints earn more credibility than those that assume implementation will proceed smoothly. Your application should describe who will manage the implementation internally, what staff training timeline looks like, whether you're partnering with a regional health system or cooperative for implementation support, and how you'll maintain operations during the transition period.
A technology partnership strategy that shows you've done your homework. State evaluators are looking for organizations that understand the vendor landscape, not organizations that accepted the first proposal they received. Documenting that you evaluated three vendors, conducted reference calls, and selected the solution based on specific criteria demonstrates the financial stewardship that justifies public investment.
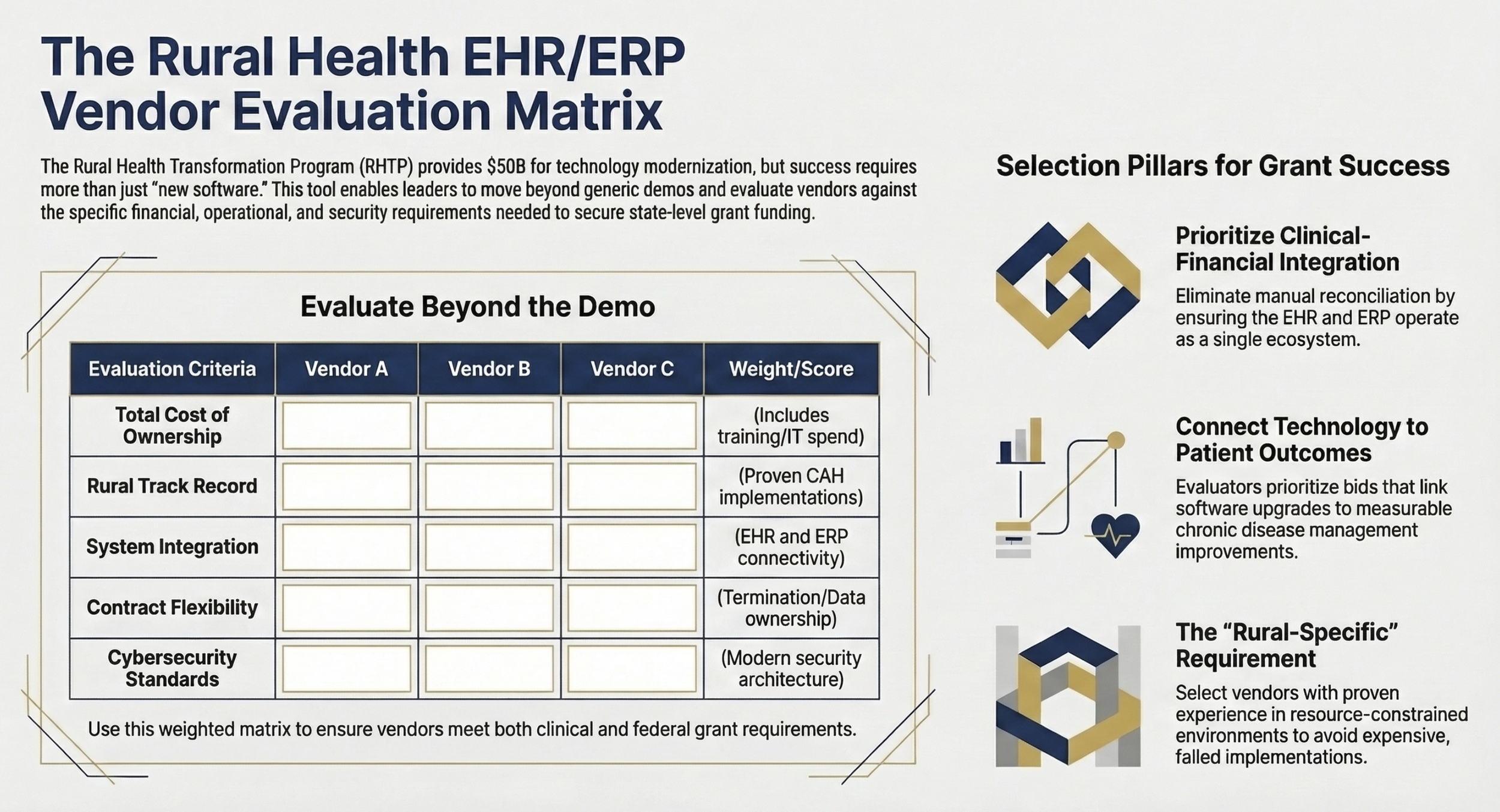
Decision framework / checklist matrix Content: Five-column scoring matrix with rows for Vendor A/B/C evaluation against criteria: Total Cost of Ownership, Rural Implementation Track Record, Integration with Existing Systems, Contract Terms and Flexibility, Cybersecurity Standards Purpose: Provide a reusable CFO/CIO vendor evaluation tool readers can adapt for their own RFP process
Your Next 90 Days: What Finance Leaders Should Do Right Now
The state award process is complete. Every state has been funded. What happens next is determined at the provider level, and the organizations that engage first will have the most influence over how state implementation plans take shape.
Look up your state's RHT Program project abstract this week. CMS published abstracts for all 50 states as part of the award announcement. Your state's abstract describes the priorities it committed to when applying — technology, workforce, access, or some combination. If your state's abstract doesn't explicitly mention EHR infrastructure or technology modernization, that doesn't mean it's excluded. States must deploy funds across at least three approved use categories, and technology is on every state's eligible list. But knowing your state's stated priorities tells you how to frame your organization's case.
Contact your state hospital association and your state Medicaid agency within the next 30 days. Ask specifically how rural providers will be engaged in implementation planning and whether there is an advisory process or provider input mechanism. If your state is moving quickly toward implementation, you want a seat in that conversation before the framework is set.
Complete a current state technology assessment within 60 days. If you don't have internal capacity, contact your Regional Extension Center or your state Primary Care Association for assessment resources. Organizations that arrive at state planning conversations with documented needs and specific project proposals will have far more influence than those arriving with general requests.
Begin your CFO/CIO governance structure now, before funding flows to providers. Organizations that have governance in place execute faster and with fewer missteps than organizations that try to build governance and run an implementation simultaneously.
For rural finance leaders who want to understand the full financial picture of what Critical Access Hospital designation means for your technology investment decisions, the financial mechanics are covered in depth here: Critical Access Hospitals: The Financial Reality of Keeping Rural Healthcare Alive.
The RHTP is not a rescue program. It's a bridge. Rural hospitals that use this funding to build genuinely modern, integrated, secure technology infrastructure will emerge from the five-year program in a fundamentally different competitive position. Rural hospitals that use it to patch aging systems without addressing the underlying governance and integration problems will be back in the same position in 2031.
The difference between those two outcomes is the work you do in the next 90 days.
If you're currently planning an RHTP technology bid or working through an EHR evaluation, hit reply and tell me where you're stuck. The most common implementation failure points are rarely the ones vendors warn you about.
P.S. What's the single biggest obstacle your rural health system faces in pursuing RHTP technology funding: governance, vendor selection, state access, or internal capacity? Reply and let me know — I'm tracking the most common answers to write a follow-up on the top three barriers.