
Value-Based Payment Models 2026: Health System CFO Strategy Guide for TEAM and CJR-X
Mandatory bundled payments are expanding faster than most executives planned. Here is how to build a financial infrastructure that protects margin.
The TEAM model launched in January 2026 across 740 hospitals, and six days before a major industry conference in April, CMS announced CJR-X, expanding mandatory bundles to every U.S. hospital for joint replacement starting in September 2027. If your organization is still treating value-based care as a future planning item, the window for reactive preparation is almost closed.
The language around value-based care has been aspirational for a long time. Better outcomes. Lower costs. Improved patient experience. Those goals have existed on strategy slides since the Affordable Care Act passed in 2010. What is different now is the enforcement mechanism. CMS is no longer offering runway. It is setting deadlines.
For health system CFOs, the question has shifted from "should we participate in value-based models" to "how do we build the financial and operational infrastructure to survive mandatory participation at scale." That is a different problem, and it requires a different kind of planning. CMS compliance and financial exposure have been intensifying on multiple fronts simultaneously, and the mandatory bundled payment expansion is part of the same directional shift.
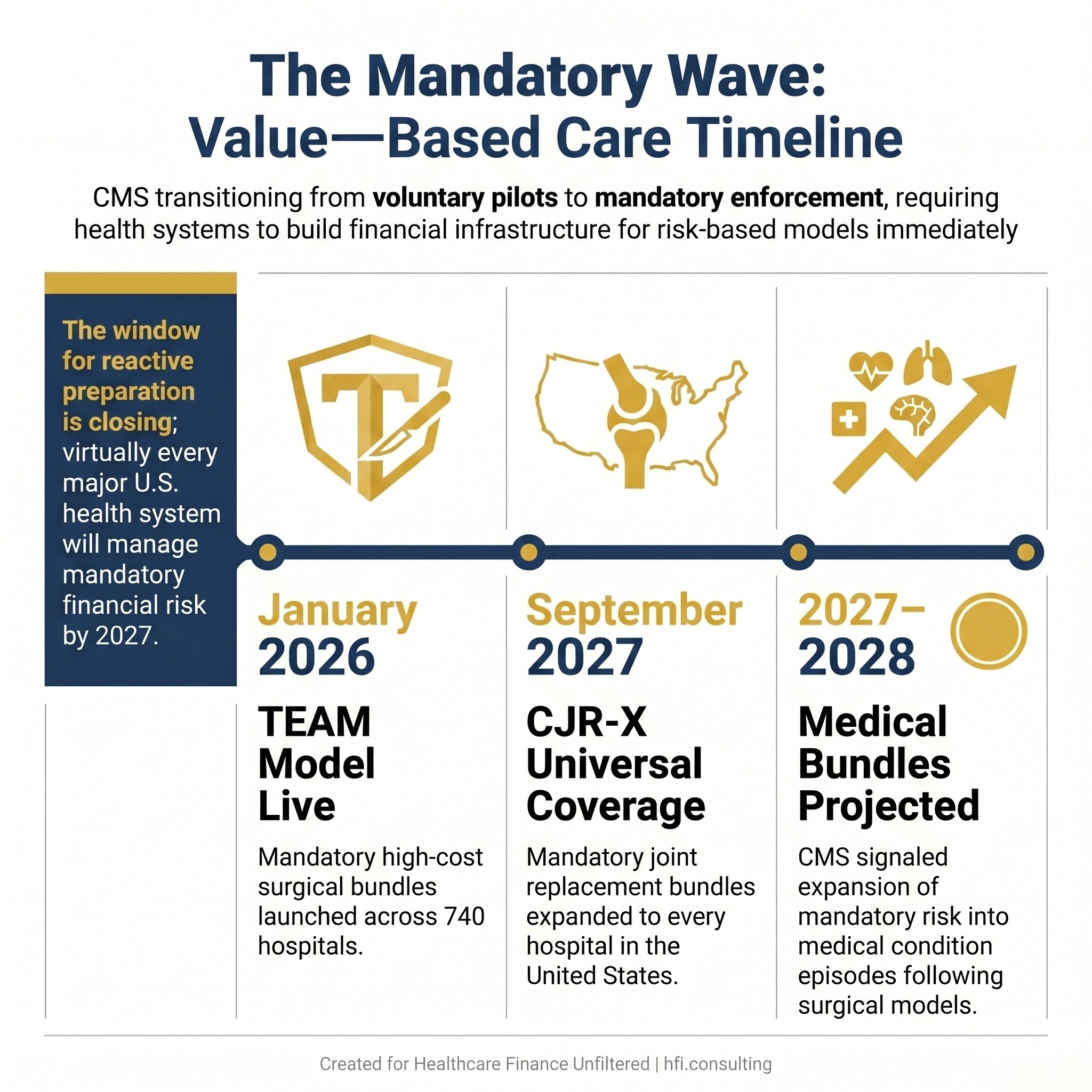
Timeline graphic showing three mandatory value-based payment milestones from 2026 to 2028 for U.S. health systems
Why the Timeline Just Changed
The Transforming Episode Accountability Model went live in January 2026, marking a decisive break from the voluntary bundled payment experiments that defined the past 15 years. TEAM is not a pilot. It is a mandatory program covering specific high-cost surgical episodes at participating hospitals.
CJR-X extends mandatory bundles to the full U.S. hospital population for joint replacement beginning in September 2027. CMS has signaled that further mandatory bundles covering medical conditions are expected by the end of 2027 and into 2028.
Read that sequence again: one year from now, virtually every major health system in the country will be managing mandatory financial risk for at least one episode category. Within two to three years, medical condition bundles will follow. Organizations that treat this moment as the starting gun, rather than the final warning, will be far better positioned than those still in "explore and evaluate" mode.
The lesson from organizations that navigated the voluntary BPCI Advanced program is instructive. Sound Physicians, which managed more than 300,000 episodes over nearly seven years as the largest initiator under that program, has been explicit about what separates performing systems from struggling ones: success is not achieved through education campaigns. It requires redesigned workflows, embedded care planning, and physician incentives that are structurally tied to total cost of care.
What the Financial Model Actually Requires
Value-based payment models exist on a spectrum of financial risk. CMS categorizes them from pay-for-reporting at the low end through shared savings, shared risk, and full capitation at the high end. The AHA framework maps this as a continuum where organizations can phase into risk rather than flip a switch.
In practice, most health systems have been living somewhere in the middle, carrying fee-for-service volume while building limited ACO or bundled payment capability. That middle position becomes harder to sustain as mandatory participation eliminates the option to stay on the sidelines.
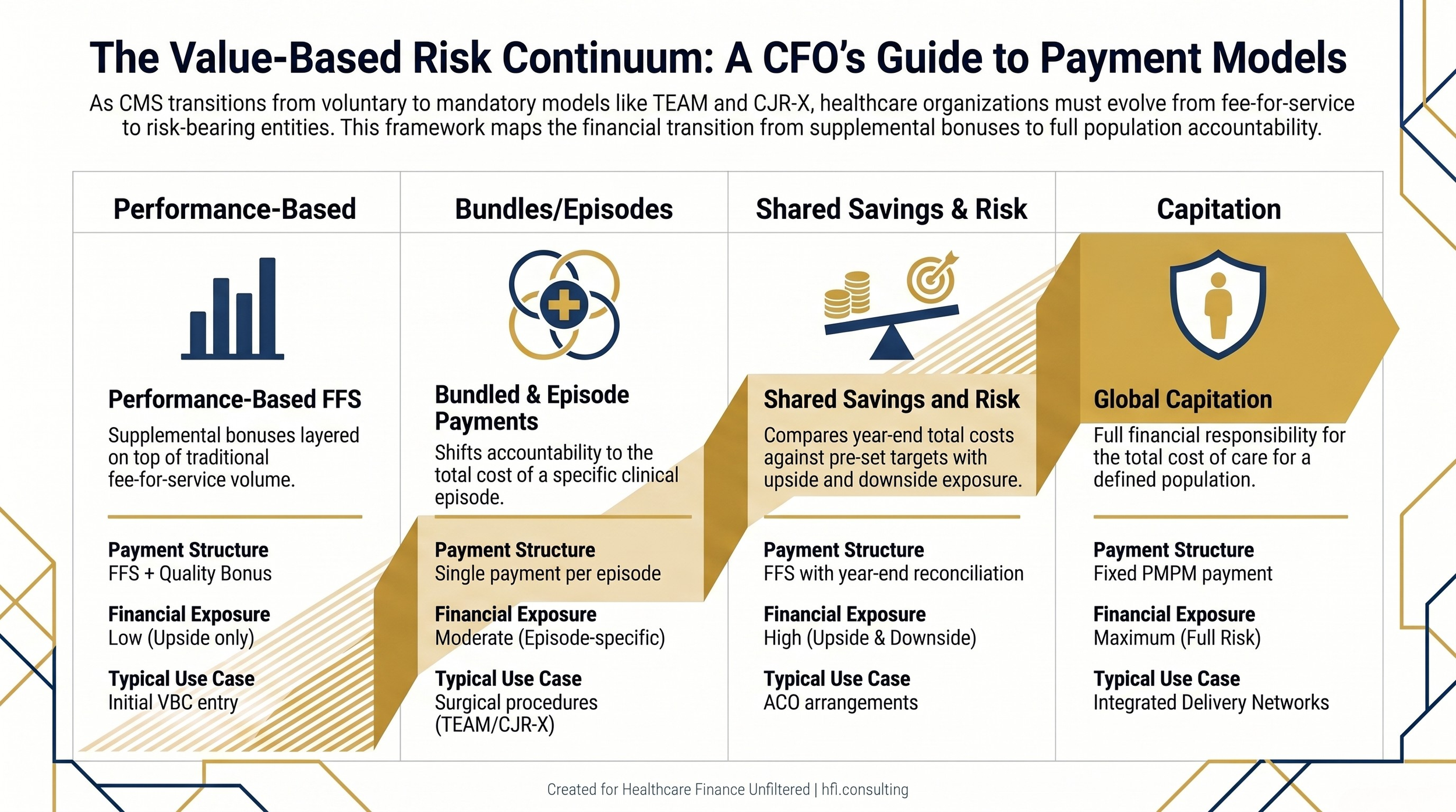
Four-column comparison table of value-based payment models from performance-based payment to full capitation showing risk level and financial exposure
Understanding where each service line sits on the risk spectrum is the starting point for CFO planning. A hospital managing 600 total joint replacement cases annually under CJR-X needs to know its contribution margin per episode, post-acute spending by discharge disposition, and readmission costs broken out by payer. If those data sets are not readily accessible today, they need to be built.
Deloitte's framework for value-based payment adoption identifies four models that define the landscape: performance-based payment layered on top of FFS, bundled and episode-based payments, shared savings and shared risk arrangements, and global capitation. Most hospital systems will operate across two or three of these simultaneously for different service lines, different payers, and different patient populations.
The Three Operational Levers That Move the Needle
Organizations that have generated strong financial results under value-based arrangements consistently cite the same operational building blocks. They are not complicated. But they require sustained investment and cross-functional commitment that cannot be assembled reactively.
Post-Acute Care Redesign
Post-acute spending is the most variable and the most improvable cost category within an episode bundle. For a total joint replacement, the difference between a patient discharged to a skilled nursing facility versus home with physical therapy can represent $8,000 to $12,000 in episode cost. Multiply that across hundreds of cases and the financial impact is material.
Redesigning post-acute workflows means building real-time visibility into where patients are going, why, and what it costs. It means investing in care coordination staff who manage transitions actively, not retrospectively. And it means building preferred partner relationships with post-acute providers who share data and align on quality metrics.
Sound's purpose-built Medicare Shared Savings Program ACO for long-term care residents illustrates what targeted post-acute redesign can produce at scale. In its inaugural year, the ACO saved Medicare $23 million. In 2024, that figure grew to $114 million. The model worked because it treated high-cost, high-complexity patients as a distinct subpopulation requiring dedicated infrastructure, not a workaround tacked onto existing community ACO operations.
Physician Incentive Alignment
This is where most health system value-based care strategies stall. Physician compensation that rewards visit volume and procedure throughput is structurally incompatible with total cost of care accountability. Closing that gap requires redesigning incentive structures, which is politically difficult even when the financial logic is clear.
In my work at Ascension across seven hospitals, the organizations that made the most meaningful progress on value-based care metrics were the ones that embedded quality and efficiency metrics directly into physician compensation models rather than treating them as aspirational overlays. Physicians need to understand not just the financial mechanics of a bundled payment but why reducing avoidable readmissions and optimizing post-acute placement actually aligns with the outcomes they trained to deliver.
The message from Providence Health is worth internalizing here. The system holds over 1.9 million covered lives in value-based arrangements across 51 hospitals in seven states and generated more than $177 million in Medicare savings in 2025, with shared savings awards exceeding $127 million. That performance did not come from a single initiative. It came from sustained cultural investment in physician engagement and a governance structure that made care variation visible across the full continuum.
Data Infrastructure for Episode Tracking
CFOs cannot manage what they cannot measure. For bundled payment programs, that means building the ability to track episode costs in real time, not 60 days after the quarter closes.
An effective episode cost tracking framework includes claims-based spending by episode category, post-acute utilization breakdowns, readmission rates and costs by physician and discharge disposition, and benchmark comparisons against CMS targets. Most organizations have some of these data points. Few have them integrated into a dashboard that is operationally useful for care teams and financially actionable for finance leaders. The same real-time cost tracking and analytics infrastructure that drives revenue leakage prevention applies directly here: the data architecture is nearly identical, and organizations that have built it for one purpose have a meaningful head start on the other.
Investment in this infrastructure is not optional under mandatory programs. The organizations that built data capability voluntarily during the BPCI Advanced era had a significant advantage when mandatory participation arrived. Those building it reactively under TEAM are starting behind. In our work with health systems at HFI Consulting, the contribution margin gaps we most consistently find are in implant-intensive service lines where vendor contract variation makes per-episode cost unpredictable well before post-acute spending enters the picture.
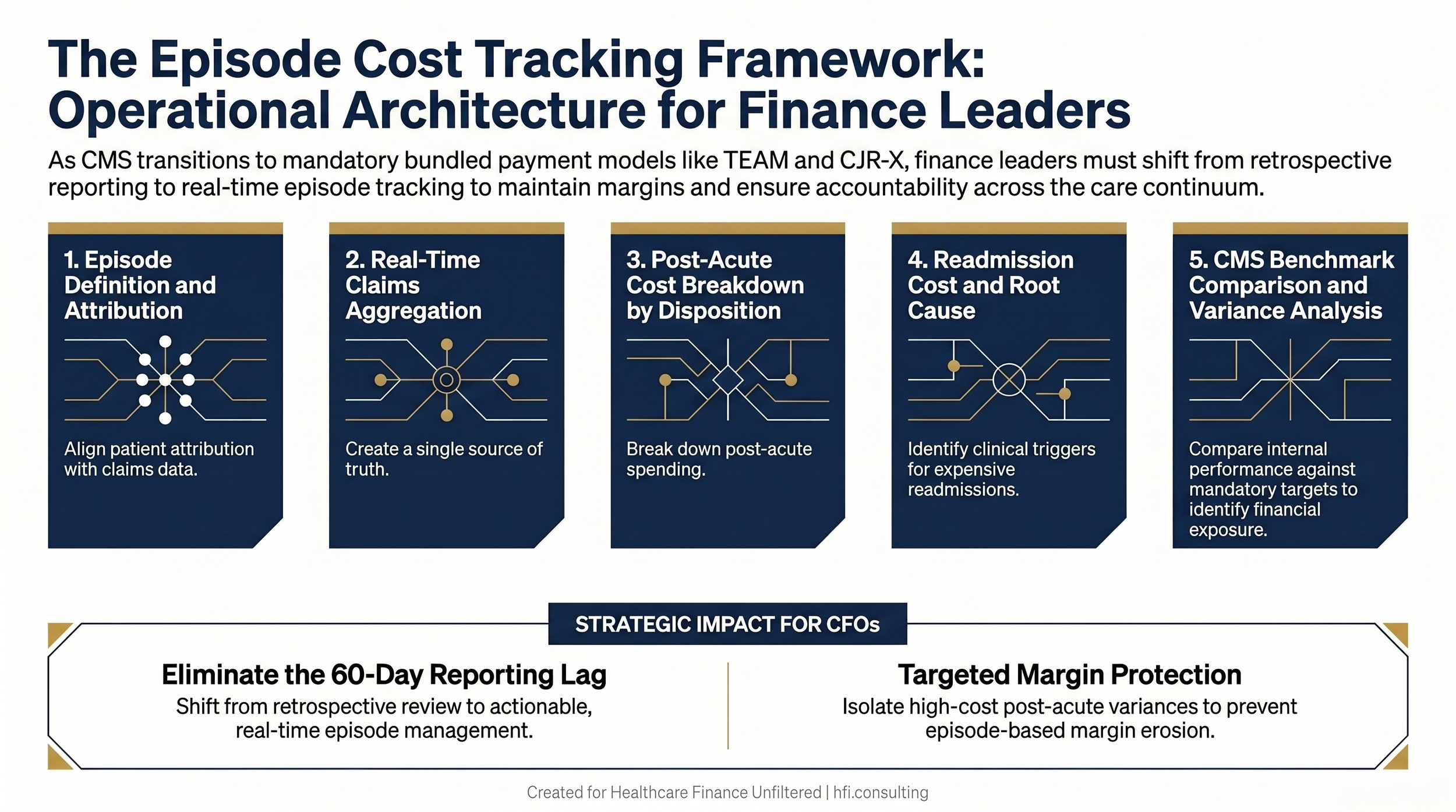
Five-step episode cost tracking framework diagram for hospital CFOs managing bundled payment programs
Managing the High-Cost Subpopulation Problem
One of the most underestimated challenges in value-based care is the concentration of spending in a small patient subset. Approximately 10% of Medicare beneficiaries account for roughly 60% of annual Medicare spend. Long-term care residents represent a disproportionate share of that group, with average annual spend of $40,000 to $50,000 compared with $12,000 to $13,000 for community Medicare ACO beneficiaries.
Standard ACO programs designed for community Medicare beneficiaries do not effectively serve this population. The care coordination model, the data integration requirements, and the post-acute partnerships needed for long-term care residents are fundamentally different from what works for a relatively healthy 68-year-old managing two chronic conditions.
For health system CFOs, the financial implication is straightforward: if your value-based care strategy does not account for this subpopulation differently, you are likely leaving savings on the table while carrying unmanaged downside risk. Purpose-built care models for high-complexity patients are an investment with measurable ROI, not a cost center.
Ready to assess your health system's value-based care financial readiness? The framework for building episode cost infrastructure, post-acute redesign, and physician incentive alignment is exactly the kind of operational finance work that determines whether mandatory participation becomes a margin opportunity or a margin threat. Visit hfi.consulting to explore how targeted financial analysis can position your organization for what is coming.
The Health Equity Dimension CFOs Cannot Ignore
CMS is increasingly incorporating social risk factors into value-based payment benchmarks. This matters financially, not just operationally.
Health systems serving higher-proportion safety-net populations face structurally different risk profiles under episode-based programs. A patient with unstable housing discharged after a total joint replacement faces a materially higher readmission risk than a patient with robust home support. If your benchmarks do not account for that difference, your financial performance metrics will systematically understate the challenge your care teams are actually managing.
CFOs should be actively assessing whether their current value-based contracts include appropriate risk adjustment for social determinants of health. Where they do not, that is a negotiation point in payer contract discussions, not something to accept as a fixed parameter.
The Payer Perspective: Succeeding on the Other Side of the Table
Approximately one quarter of the value-based care story belongs to payers, and it is a meaningfully different operational challenge.
For Medicare Advantage plans and commercial insurers, value-based contracting with providers is both a cost management tool and a member experience lever. Plans that structure value-based arrangements effectively can drive better outcomes for members, reduce total cost of care, and differentiate their network in competitive markets. The Medicare Advantage rate pressures heading into 2027 make cost-efficient provider partnerships even more strategically important for plan CFOs managing tightening margins.
From my time managing Medicare Advantage operations at Florida Blue Medicare, including HRA program oversight and MA plan financials, the payer-side challenge is not lack of interest in value-based contracting. It is execution complexity. The practical barriers include:
Clinical data integration: Claims data exists. Clinical data from provider EHR systems is far harder to access and normalize. Without it, plans cannot generate the population health insights that make value-based partnership genuinely useful to providers.
Benchmark design: How a plan sets its total cost of care targets has enormous implications for provider willingness to participate. Benchmarks that feel arbitrary or that do not reflect regional cost variation will drive providers back to transactional fee-for-service relationships.
Attribution accuracy: Getting the right patients attributed to the right providers under the right value-based contracts sounds administrative. In practice, attribution errors can create millions of dollars of financial exposure and undermine the trust between payer and provider that makes the model work.
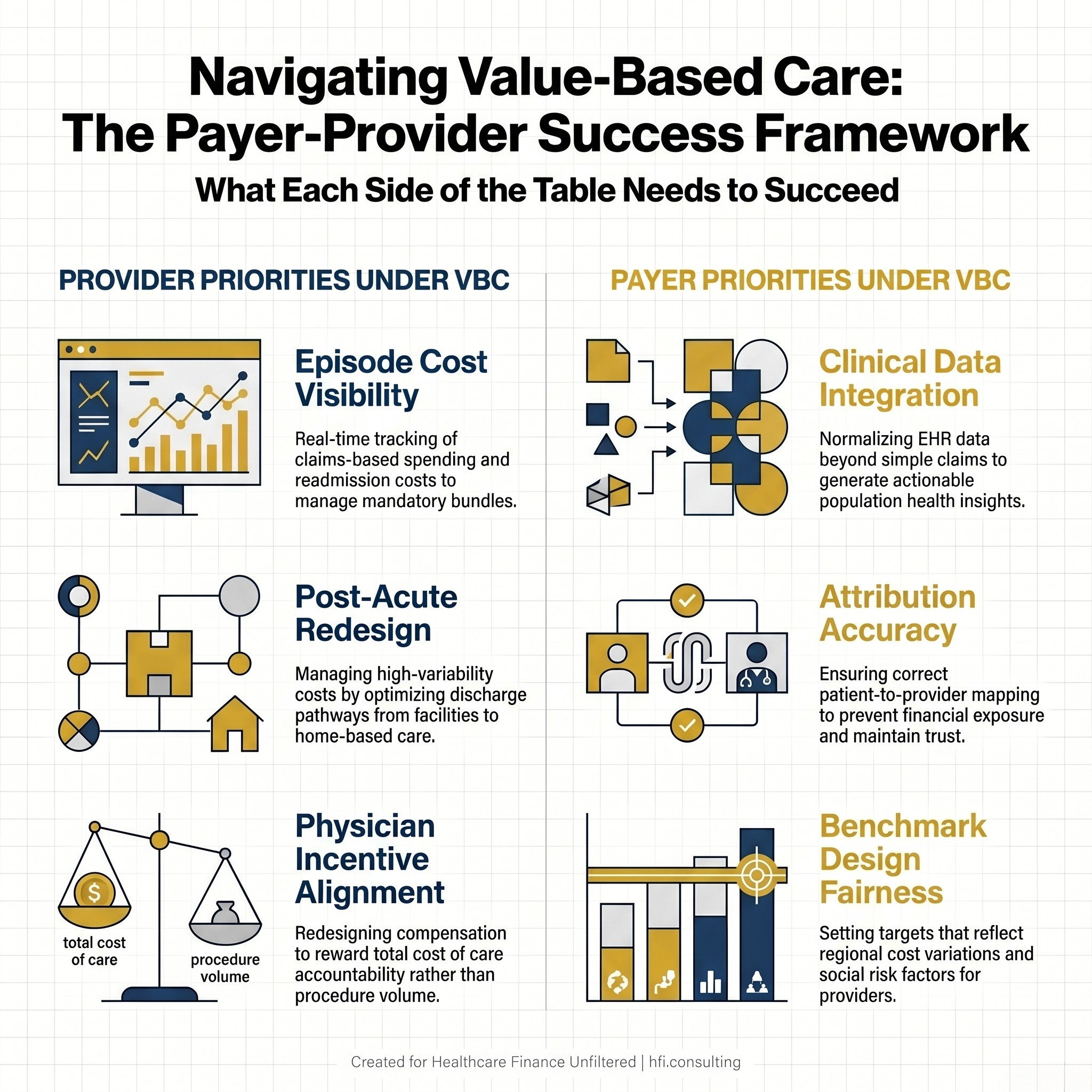
Side-by-side comparison of provider and payer strategic priorities in value-based care arrangements
For payer CFOs specifically, the strategic priority is building the data infrastructure to be a genuinely useful partner to provider organizations rather than simply a contract counterparty. Plans that can offer providers real-time claims data, attribution rosters, risk score transparency, and actionable quality measure performance reports are far more likely to recruit and retain high-quality provider partners in value-based arrangements. The contracting dynamics around alternative care delivery models like Hospital at Home are a useful illustration of how this plays out in practice: payer-side contract strategy for alternative care delivery requires the same data fluency and benchmark transparency that value-based bundled contracts demand.
The Deloitte framework for payer capabilities in value-based care identifies data analytics, network design, and contract administration sophistication as the core differentiators. Plans that invest in these areas are better positioned to structure arrangements that work financially for both parties, rather than designs that look good in a board presentation and collapse in year two when providers discover the downside risk is not manageable.
What CFOs on Both Sides Should Be Doing Right Now
The mandatory expansion of bundled payments is not happening to organizations that are already deeply invested in value-based infrastructure. It is happening to organizations still in planning mode.
For provider CFOs, the immediate priorities are: completing an episode cost baseline for TEAM-covered service lines, assessing post-acute partner performance against quality and cost metrics, reviewing physician compensation models for structural alignment with total cost accountability, and identifying which high-complexity subpopulations require dedicated care management investment.
For payer CFOs, the priorities are: auditing data-sharing capabilities to ensure they can be a useful partner rather than a passive contract counterparty, reviewing attribution methodology for accuracy and fairness, and assessing whether current value-based contract designs actually create aligned incentives or just shift risk without creating shared accountability.
The organizations that win under mandatory value-based care will not be the ones that respond fastest when the rules change. They will be the ones that built the infrastructure before it was required and treated the current regulatory environment as confirmation of a strategic direction, not a disruption to it.
For more on the financial modeling frameworks, physician incentive design, and episode cost tracking tools that support value-based readiness, visit hfi.consulting
P.S. Is your organization treating the TEAM model and CJR-X expansion as a clinical program or as a finance problem? I want to know how CFOs are thinking about the episode cost infrastructure required. Hit reply and tell me where your organization is in the readiness process.