
AI in the Revenue Cycle: How Hospitals Are Fighting Back Against Payer Take-Backs
Recoupments cost providers $1.6B a month. Here is the CFO framework for using AI to surface, challenge, and recover what payers are taking back.
Payers recouped more than $1.6 billion from healthcare providers last month. And the month before that. And the month before that.
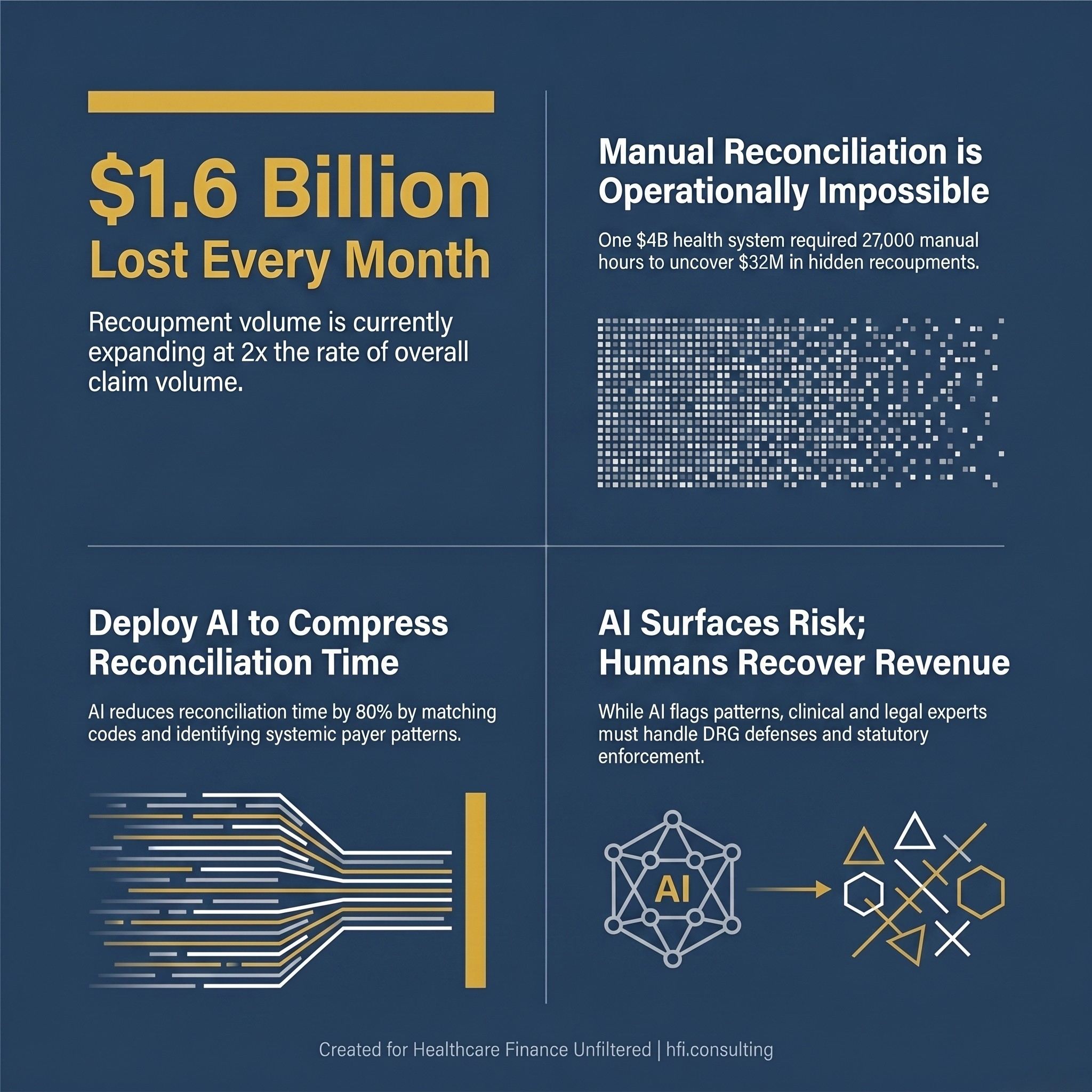
Infographic showing payer recoupments cost healthcare providers $1.6 billion per month, with recoupment volume growing at twice the rate of overall claims
Most of that money left provider bank accounts quietly, buried inside remittance adjustments that revenue cycle teams often lack the staff, the tools, or the time to scrutinize line by line. In the same period, providers lost an additional $48 billion in net revenue to final denials and uncollected patient responsibilities in 2025 alone.
The financial pressure is real. And now the battlefield is shifting.
The Mechanics of What Payers Are Doing
Understanding take-backs starts with separating them from traditional denials. A denial stops a claim before payment. A recoupment, also called a take-back, happens after payment has already been received and recorded as revenue.
Payers execute recoupments by offsetting future payments, quietly deducting amounts owed from subsequent checks. For revenue cycle teams without robust ERA reconciliation workflows, these deductions often surface as unexplained variances in expected cash.
Take-backs generally fall into two categories.
Administrative recoupments are triggered by data mismatches: duplicate payments, retroactive eligibility terminations, coordination of benefits errors where another payer is identified as primary after the fact. These are often valid, but they are also frequently applied without adequate notice to providers.
Clinical and DRG recoupments are more complex and more contentious. They result from post-payment audits where the payer argues that clinical documentation does not support the billed Diagnosis Related Group. A Sepsis-3 claim gets downgraded to a simple infection. A high-complexity DRG gets reclassified to a lower-weighted code. These disputes require a different response strategy entirely.
What makes both categories operationally dangerous is that they are growing. According to Waystar, recoupments have expanded at twice the rate of overall claim volume over the past three years. Payers facing rising medical loss ratios and higher utilization are using take-backs as a lever to manage their own financial position.
Why Finance Leaders Have Been Flying Blind
For most hospital finance teams, the recoupment process has been a black box. The Electronic Remittance Advice arrives with adjustment codes. Someone on the revenue cycle team has to match those codes to originating claims, determine whether the deduction is justified, calculate the financial exposure, and decide whether to initiate an appeal.
That process is not automated at most organizations. It requires dedicated staff, institutional knowledge of payer behavior, and access to historical claims data spanning months or years. The Waystar data makes the scale concrete: one health system with roughly $4 billion in annual revenue was found to have $32 million in hidden recoupments that would have required the equivalent of 27,000 hours of manual reconciliation annually. That is approximately 13 full-time employees, working year-round, doing nothing else.
Most organizations do not have 13 people assigned exclusively to recoupment research. So the adjustments get written off. The revenue disappears. The payer wins by default.
What AI Can Actually Do Here
The "set it and forget it" framing around AI in revenue cycle has set unrealistic expectations across the industry. As Paul LePage, VP of Revenue Cycle at UC Davis Health, noted in recent Becker's reporting, AI in RCM augments human expertise. It surfaces patterns in denials, prioritizes work queues, and automates lower-complexity tasks. It does not replace payer strategy, contract interpretation, or escalation judgment.
That framing matters for how finance leaders structure their AI investments.
For recoupments specifically, AI is genuinely useful in three areas.
Pattern identification at scale. AI can scan remittance datasets and claims history simultaneously, matching adjustment codes to originating claims and flagging systematic patterns that indicate payer behavior rather than isolated billing errors. When a payer begins consistently downgrading a specific DRG across multiple admissions, an AI system can surface that pattern within days. A manual review team might not catch it for quarters.
Prioritization of appeal opportunities. Not every recoupment is worth challenging. AI can evaluate the dollar value of each adjustment, the strength of the underlying documentation, the payer's historical appeal reversal rate for similar adjustments, and the deadline window, then rank the appeal queue accordingly. That moves finance leaders from reactive triage to strategic prioritization.
Reconciliation time compression. Waystar reports that its AI capability reduces reconciliation time by more than 80%, providing full visibility into payer recoupments so providers can identify and respond to take-backs they would previously have written off. For one early adopter health system, that meant recovering $32 million from adjustments that had been invisible.
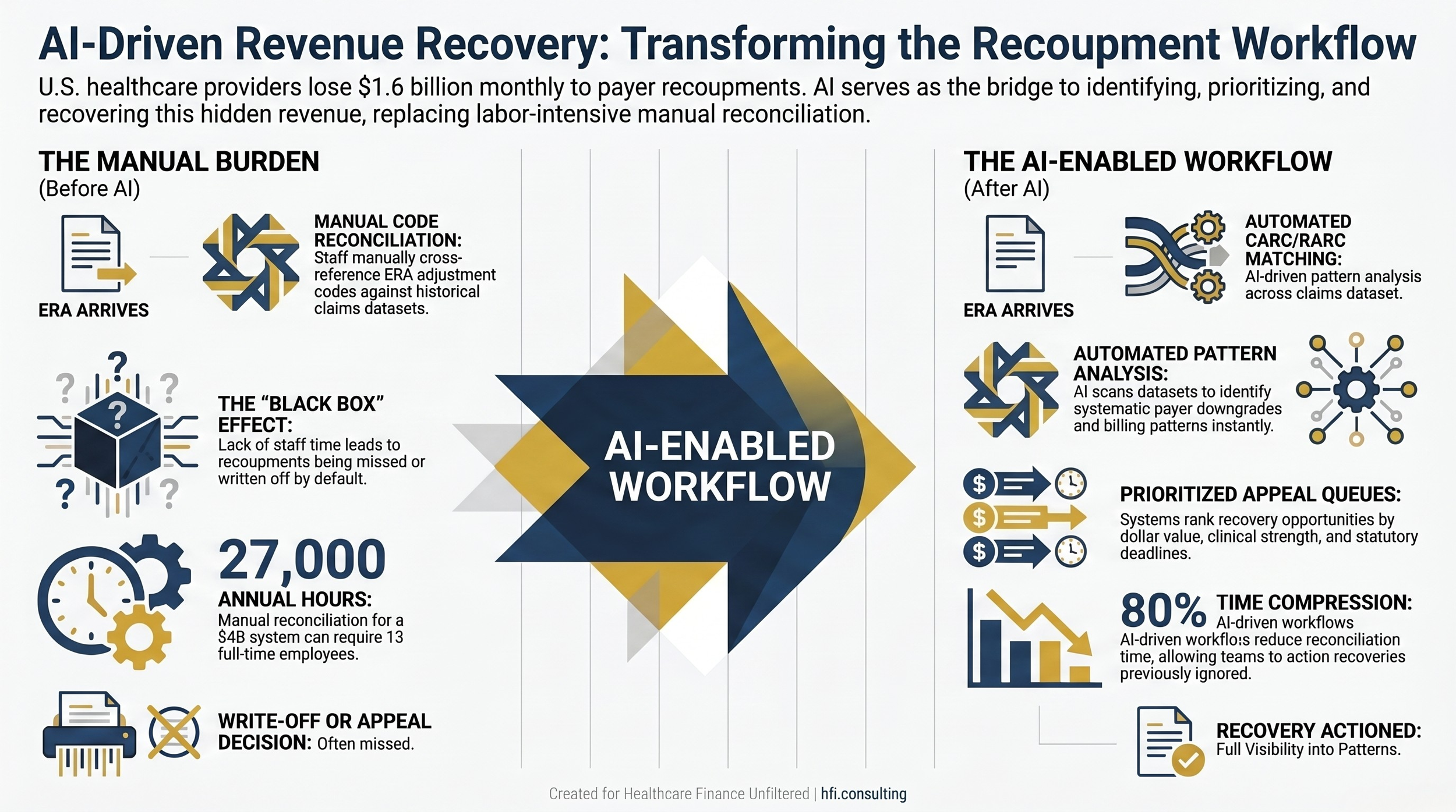
Side-by-side process flow comparing manual recoupment reconciliation to AI-enabled reconciliation workflow in hospital revenue cycle management
What AI Cannot Do: The Governance Problem
This is where the operational reality diverges sharply from the vendor pitch.
AI can surface a $32 million recoupment problem. It cannot write the clinical narrative for the appeal. It cannot interpret the specific contract language in your payer agreements. And it cannot fix the documentation gaps that led to the DRG downgrade in the first place.
Laura Elliott, VP of Revenue Cycle at Brooks Rehabilitation in Jacksonville, put it plainly in recent industry commentary: AI can identify patterns, predict risk, and prioritize work, but it cannot fix broken processes, unclear accountability, poor data integrity, or weak payer strategy.
That is not a critique of the technology. It is a definition of what governance must provide.
Finance leaders deploying AI in their recoupment workflows need to build three operational layers around the technology.
Clinical validation capability. When a payer challenges a DRG on clinical grounds, the response is not a coding defense. It is a clinical defense. The hospital needs a clinician who can document that the treating physician's judgment and the patient's specific clinical indicators supported the billed diagnosis. AI can flag the dispute. A physician advisor or clinical documentation specialist has to resolve it.
Contract modeler integration. Take-backs coded with CO-45 (charge exceeds fee schedule) often reflect payer system calculation errors, not provider billing errors. The proof is in the contract. Finance teams need a contract modeler who can demonstrate, rate by rate, that the payer's system is calculating the allowed amount incorrectly. That is a human function with AI support, not the reverse.
Statutory protection awareness. In many states, there are legal limits on how far back payers can reach for recoupments and specific notice requirements before offsets can be applied. Florida, for example, limits look-back windows for commercial payers and Medicare Advantage plans under statutes 627.6131 and 641.3155. If a payer attempts a take-back outside the statutory window, or applies an offset without providing the required 30 to 45 days' notice and appeal opportunity, the recoupment can be challenged on procedural grounds alone, regardless of the underlying clinical question.
AI is not reading your state statutes. Your revenue cycle counsel is.
The Payer Take-Back Response Framework
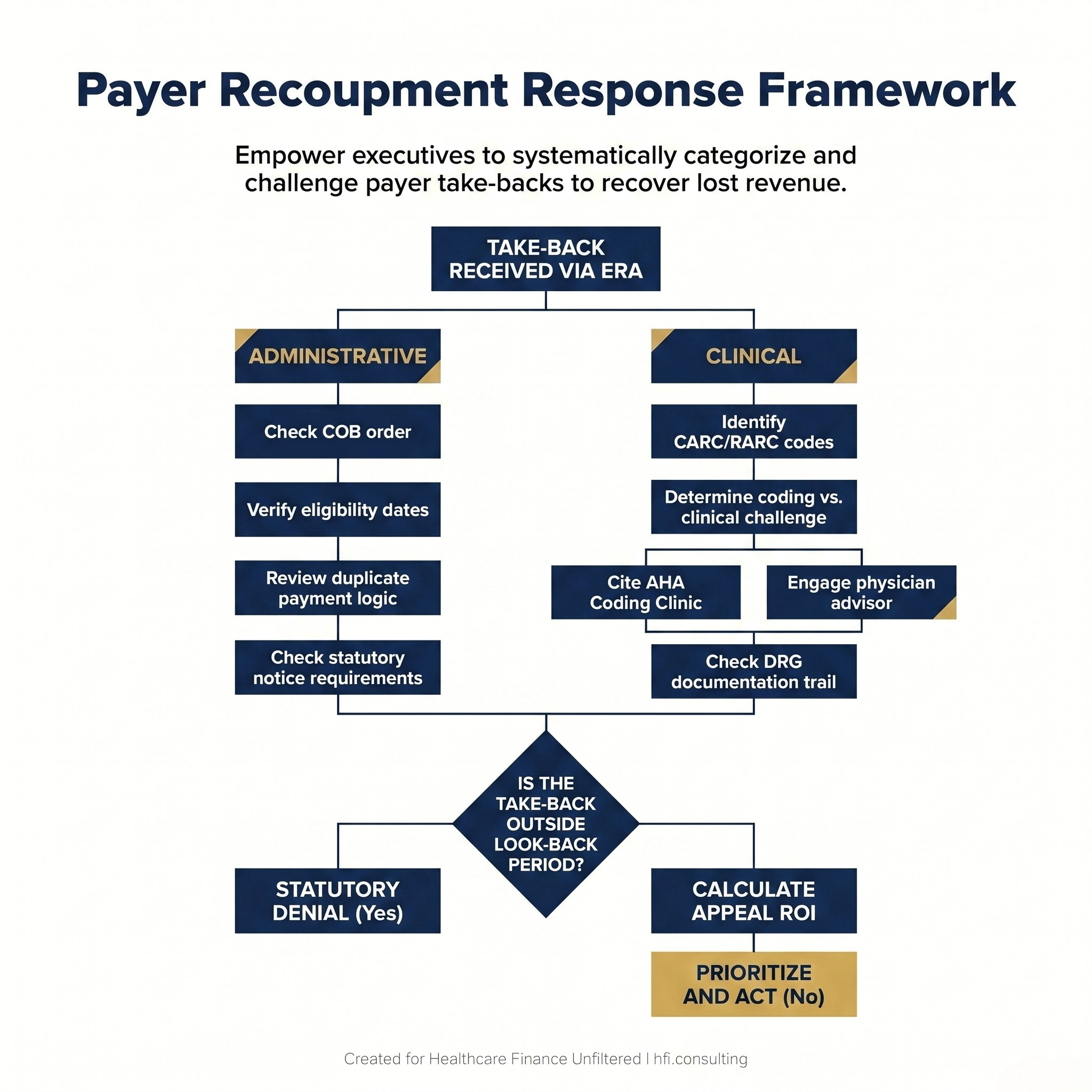
Decision tree flowchart showing hospital revenue cycle team steps for responding to payer recoupments, from ERA receipt through clinical or administrative appeal pathways
The practical framework for responding to take-backs has four components.
Identify the adjustment type before beginning the appeal. CARC and RARC codes on the ERA are your starting point. CO-45 is a rate dispute. CO-50 is a medical necessity challenge. PI codes are payer-initiated reductions that require immediate scrutiny of the underlying contract's right-of-recovery language. Coding the response correctly before beginning the appeal prevents wasted effort.
Separate coding accuracy from clinical validity. Payers frequently conflate these two challenges, and hospitals often respond to clinical challenges with coding defenses. If a payer is arguing that the diagnosis itself is invalid, citing an ICD-10 guideline will not resolve the dispute. The hospital needs a clinician to demonstrate that the patient's lab values, treatment response, and clinical course supported the billed diagnosis.
Build a device and implant documentation trail. High-cost implants are a frequent target for post-payment audits. The defense requires implant logs, serial numbers linked to the specific patient and operative report, invoice reconciliation that ties acquisition cost to the contracted carve-out rate, and warranty credit documentation if a manufacturer return is involved. In my work at UF Health Jacksonville, managing cost accounting for a Trauma I and Level 3 NICU, the gap between what was billed and what was documented for high-cost implants was a recurring source of exposure. The documentation burden is significant and must be built proactively, not assembled after a payer challenge arrives.
Document the statutory timeline. If a take-back arrives without proper notice, or falls outside the applicable look-back window, that procedural failure is its own grounds for challenge. Revenue cycle teams should log the date of payer notice for every recoupment and compare it against both the contractual and statutory requirements in the relevant state.
"AI is most powerful when it is paired with governance, cross-functional alignment, KPI discipline, and leadership accountability." — Laura Elliott, VP of Revenue Cycle, Brooks Rehabilitation
Healthcare finance leaders reading this are already managing compressed margins and resource-constrained teams. The invitation from vendors to "implement AI" in the revenue cycle is real and, in the right context, well-founded. But the organizations that will see measurable improvement are the ones that treat AI as infrastructure, not a solution.
That means investing in the governance, the clinical validation workflow, the contract management capability, and the statutory knowledge that transforms AI-generated insights into recovered revenue.
If you are evaluating AI tools for your revenue cycle or building the internal case for investment, I have put together a companion resource that may help. Check out the AI-Powered Revenue Leakage Prevention guide here.
If your finance team is navigating a specific recoupment challenge or evaluating your take-back exposure for the first time, hit reply and tell me what you are seeing. I read every response.
The Payer Dynamic That Finance Leaders Cannot Ignore
There is a larger strategic context shaping this problem.
Payers are deploying AI on their side of the equation. Algorithms are flagging claims for post-payment review, identifying coding patterns that may indicate upcoding, and initiating recoupments based on statistical modeling rather than individual case review. The clinical accuracy of those models varies. The volume of take-backs they generate does not.
The ACA enhanced subsidy expiration at the end of 2025 has compounded the financial pressure on both sides. With roughly 5 million people expected to lose coverage in 2026, providers face rising uncompensated care. Payers face adverse selection and higher utilization from remaining enrollees. Recoupments, for payers, are one pressure valve.
Finance leaders cannot solve the macroeconomic dynamic. They can build the infrastructure that ensures their organizations are not absorbing unjustified losses quietly.
The organizations that are seeing meaningful results share a common pattern. They are not simply licensing AI tools. They are redesigning their revenue cycle workflows around what the technology can surface, building clinical and legal response capacity, and training their teams to operate at a higher level of analytical precision.
That is not a vendor conversation. It is a strategic finance conversation.
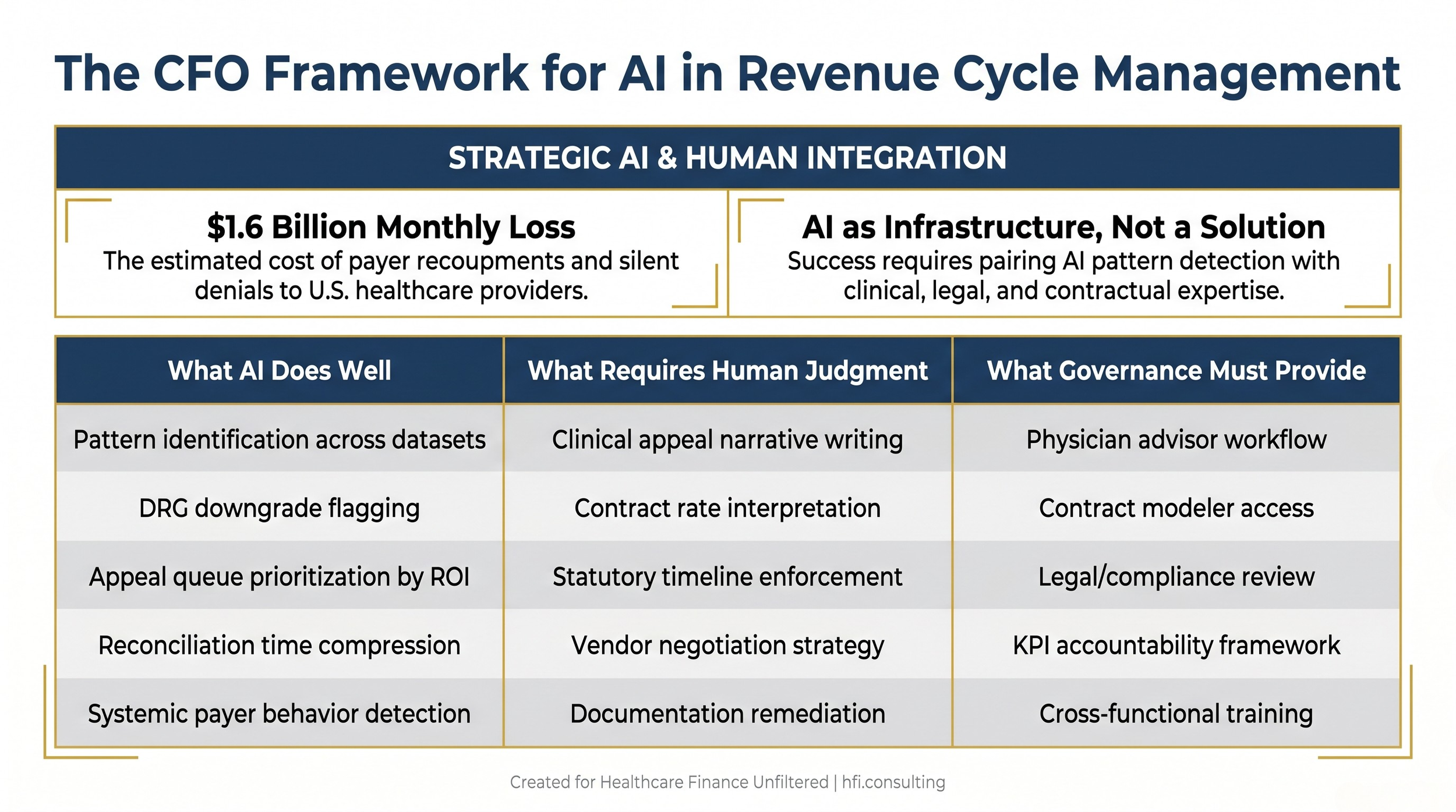
Three-column comparison table showing what AI does well, what requires human judgment, and what governance must provide in hospital revenue cycle management
The revenue cycle has always been a game of information asymmetry. Payers have historically held more data, more processing capacity, and more speed than provider billing teams. That gap is narrowing.
Finance leaders who understand what AI can surface, what their clinical and legal teams must still do, and how to build governance around both are better positioned than those waiting for a turnkey solution that does not exist.
The $1.6 billion monthly problem is not going to be solved by technology alone. But it is increasingly being solved by finance leaders who know how to deploy it.
Want help thinking through your recoupment exposure or building the internal case for AI investment in your revenue cycle? Connect with me at hfi.consulting
P.S. If you are a VP of Revenue Cycle or CFO, I am curious: where is your organization's biggest gap right now, surfacing recoupments you do not know about, challenging ones you have already identified, or building the governance to make appeals stick? Hit reply and let me know.