
Revenue Cycle Leadership Transitions: The Payer Restructuring Moment That Reframes Your First 90 Days
Payers are restructuring prior auth and UM at the same moment health systems are filling RC leadership roles. That timing is not coincidental.
More than two dozen health systems have posted revenue cycle VP and director roles in the past two weeks. Boston Children's Hospital, RWJBarnabas Health, IU Health, Penn Medicine, Providence, and others are all actively recruiting. That volume of simultaneous openings does not happen because organizations suddenly got organized. It happens when finance and operational leadership have concluded that the current team is not positioned for what comes next.
What comes next is a payer landscape that is actively restructuring itself. Cigna announced last week it is exploring strategic alternatives for EviCore, its utilization management and prior authorization subsidiary. Payer executives from CVS Aetna, Blue Cross Blue Shield of Arizona, and BlueCross BlueShield of South Carolina named AI-driven UM modernization, IDR process abuse, and VBC investment lag as their top operational challenges. Cigna's own AI risk prediction model is now generating $2,000 in savings per participating member annually by identifying complex patients earlier and connecting them to clinical resources before they hit the emergency room.
These are not background news items. For incoming revenue cycle leaders, they are the operating environment you are walking into.
Infographic showing 22+ revenue cycle VP openings at health systems alongside simultaneous payer operational restructuring in prior auth and utilization management.
The Diagnostic Window Opens on Day One
Every leadership transition carries an implicit permission structure that expires quickly. In the first 60 to 90 days of a new RC role, your predecessor's decisions are still visible and the organization has not yet calcified around a narrative about why things are the way they are. That is your window to ask questions that would later read as criticism.
In my work at Ascension across seven hospitals, I watched this play out repeatedly. Incoming leaders who used the transition period to conduct a structured operational audit consistently identified issues that would have taken two to three years to surface under normal operating conditions. Leaders who skipped that audit spent the next 18 months reacting.
The audit is not a performance review of your predecessor. It is a current-state documentation exercise. And it matters more right now than it has in years because the payer landscape that shaped your department's current workflows is actively changing.
What Cigna's EviCore Review Actually Signals
When Cigna's incoming CEO Brian Evanko said the company is exploring strategic alternatives for EviCore, the headline coverage focused on the deal mechanics. The more important signal is in the framing: as prior authorization standardizes and automates at scale, a standalone UM business becomes harder to justify as a separate entity.
Cigna, along with other major insurers, recently agreed to standardize electronic prior authorizations for common services. The prior auth model built around manual clinical review, high FTE counts, and separate operational infrastructure is being compressed by technology and regulatory pressure simultaneously.
For incoming RC leaders, that has two direct implications. First, the prior auth workflows your new team built their processes around are going to change, possibly faster than your denial management protocols can adapt. Second, if your payer contracts still assume a manual prior auth environment, those terms may be generating more administrative friction than they should.
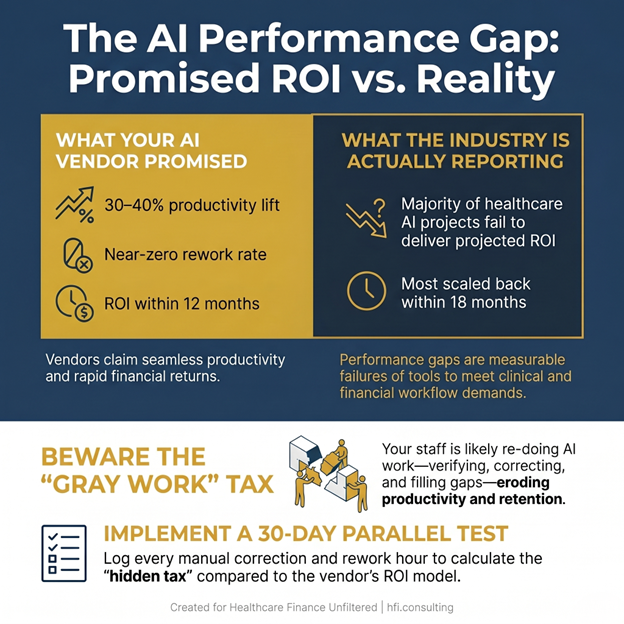
This is not an abstract operational concern. Prior auth denials represent a real and trackable component of your denial volume, and they are generated by a process that is actively being restructured on the payer side. You should know what percentage of your current denial write-offs are prior auth related before you agree to any budget targets.
The Payer AI Problem Your Predecessor Did Not Have to Solve
Cigna reported that its predictive high-cost claimants model is generating $2,000 in per-member savings annually by identifying complex patients before high-cost utilization events occur. That model works by connecting flagged members to clinical resources earlier. Inbound calls dropped 20% for digitally eligible employer business customers and 25% for pharmacy benefit members compared to two years ago.
The revenue cycle implication runs in the opposite direction from the payer's perspective. If payers are using AI to route complex members toward lower-cost care pathways before those members generate inpatient claims, your utilization mix is shifting. The cases that do generate inpatient and high-acuity outpatient claims are, by design, the ones the payer's model failed to divert. Those cases skew toward clinical complexity and documentation intensity.
Your documentation and coding team is working a harder caseload than the aggregate stats suggest. If your case mix index has drifted upward in the past 18 months without a corresponding review of your coding documentation protocols, that is a finding worth surfacing in your first operational review.
The payer also now has real-time access to risk data that your clinical and finance teams do not. That asymmetry is not new, but the sophistication gap is widening. The question for incoming RC leaders is whether your team has the data infrastructure to identify your own high-cost utilization trends before they become prior auth denials or retrospective audits.
For more on the prior authorization timeline and what compliance deadlines are approaching, the CMS Interoperability and Prior Authorization analysis is worth reviewing before your first payer contract meeting.
What the Talent Flow Is Telling You
The former SVP of Revenue Cycle at Beth Israel Lahey Health just left to become CEO of a medical billing company backed by an AI-focused holding company. In his LinkedIn announcement, he described three years spent designing a shared services operating model, reorganizing 1,500 team members, and integrating vendor services before deploying Epic across 12 facilities. He left the system to lead what he describes as a company driving transformational change in revenue cycle.
The most experienced RC operators in the country are moving toward AI-enabled billing infrastructure. They are not moving away from healthcare. They are moving toward the part of the ecosystem that has the capital and the architectural flexibility to rebuild RCM from the workflow up rather than layering AI onto a billing team that has not fundamentally changed its operating model in a decade.
That tells you something about where the leverage in this field is moving. It also tells you what the organizations recruiting right now are likely looking for. They are not hiring revenue cycle VPs to maintain the current state. They are hiring leaders who can bridge from where the department is to where the payer and technology environment is heading.
The 22-plus active postings include roles titled Vice President of Revenue Strategy and Operations (Frederick Health), Vice President of Revenue Analytics (RWJBarnabas Health), and Assistant Vice President of Revenue Cycle Systems (University of Miami Health System). Those titles are not traditional RCM titles. They signal an expectation that the next generation of RC leadership is analytically oriented, systems-focused, and capable of operating as a strategic partner to the CFO rather than as a billing department head.
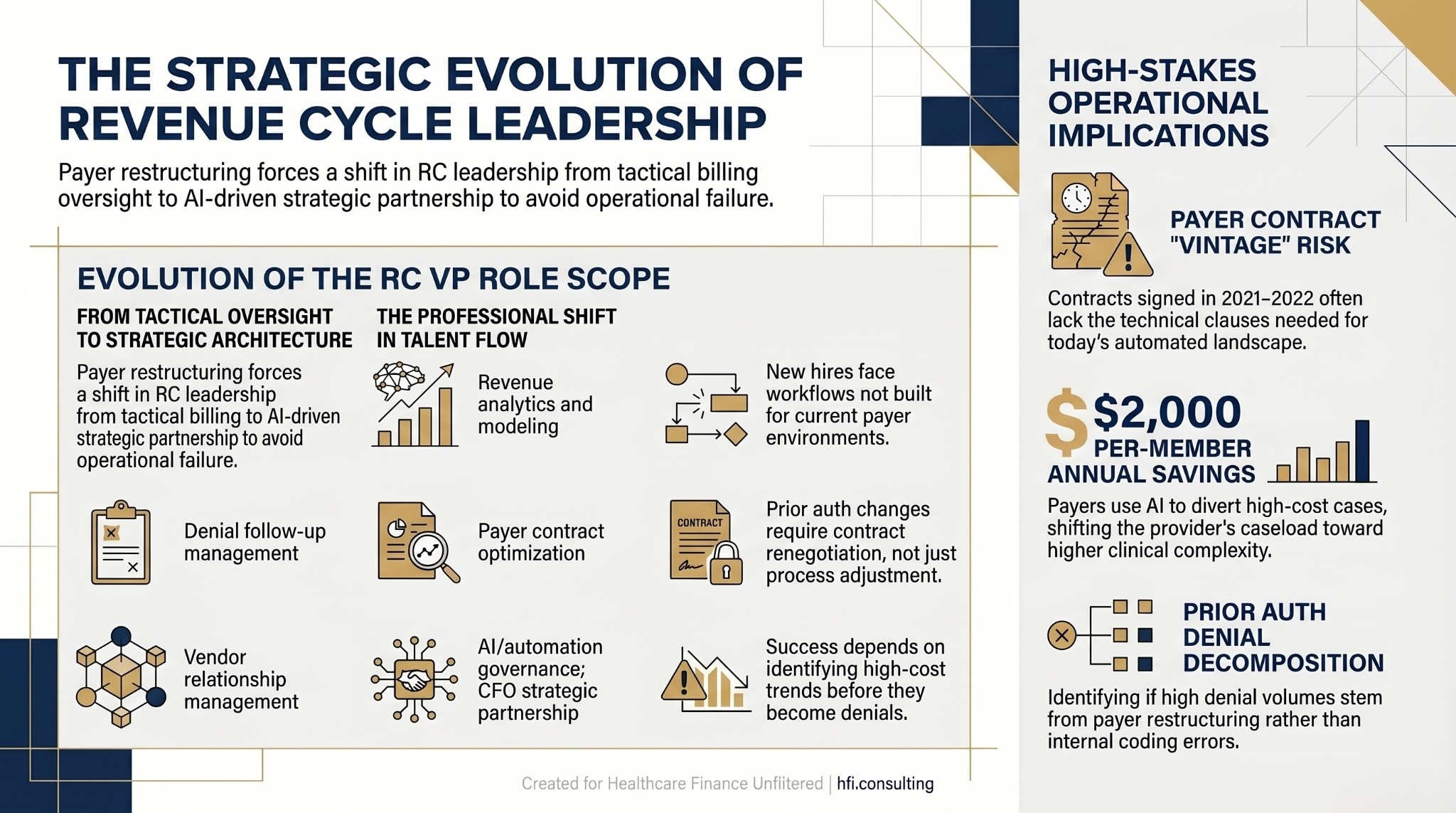
Comparison table showing traditional vs. emerging revenue cycle VP role scope and the strategic gap new leaders must bridge in the current payer environment.
Your First 90-Day Audit: What to Prioritize Given the Current Payer Environment
The standard new-leader operational review hits the basics: days in A/R, clean claim rate, denial rate, collections per encounter. Those metrics matter. They are not sufficient for the current moment.
Given simultaneous payer restructuring around prior auth, AI-driven utilization management, and electronic standardization, the audit needs to include several layers that are not on a standard RCM dashboard.
Prior auth denial decomposition. Your overall denial rate tells you where you are. Decomposing it by denial reason, payer, and service line tells you where the payer contract risk is concentrated. If 40% of your denial volume traces to prior auth, and your largest commercial payer is actively restructuring its UM subsidiary, that is a contract conversation, not a coding conversation.
Payer contract vintage review. Contracts signed in 2021 or 2022 were negotiated in a different administrative environment. The manual prior auth assumptions baked into those terms no longer match the technology trajectory on the payer side. An incoming RC leader who inherits contracts without reviewing vintage and administrative load clauses will spend two years absorbing friction that a renegotiation could have addressed.
Workflow bottlenecks that predate your predecessor. Many RC operational problems were identified, documented, and deprioritized long before your predecessor arrived. The transition period is the right time to surface those legacy issues because the organizational politics around them are briefly suspended. Ask your team: what problem has been on the list for more than two years and why has it not moved?
Vendor contract audit for technology currency. The RC vendor market is consolidating. Platforms that were competitive in 2021 may not have kept pace with what payer-side AI can now generate in denial volume. A vendor audit is not about switching vendors in your first 90 days. It is about knowing what your current stack can and cannot do before you commit to budget targets.
The Denial Loop analysis from April is a useful framing document for understanding the bilateral cost structure of the payer-provider fight.
What Payer Finance Leaders Are Actually Worried About
The Becker's Payer Issues survey of 11 payer executives published last week named several challenges that have direct revenue cycle implications on the provider side.
CVS Health Aetna's lead director for VBC provider engagement named the lag between investment and return in value-based care as the dominant challenge. That lag is a cash flow problem for providers and a contract terms problem for RC leaders. If your organization has signed value-based agreements with upside-only structure, your RC team's work on documentation quality directly affects whether savings materialize.
BlueCross BlueShield of South Carolina's VP named IDR process misuse, specifically high volumes of questionable filings and strategic batching, as a growing concern. IDR abuse by some providers increases administrative friction across the board and creates pressure for payers to tighten administrative processes that affect every provider equally.
Blue Cross Blue Shield of Arizona's VP named modernizing utilization management as the core challenge, specifically moving from transaction-heavy UM to a data-driven, clinically nuanced model. That is a direct description of what EviCore was built for and what Cigna is now reconsidering. The UM infrastructure your revenue cycle team interacts with daily is being redesigned, not just updated.
Understanding the payer side of these operational pressures is not a courtesy exercise. It is a negotiating prerequisite. RC leaders who know what their payer counterparts are managing internally have a better starting position in contract conversations than those who treat payers as an external variable rather than an organization with its own operational constraints.
If you are stepping into a new revenue cycle role or advising one, the 90-day diagnostic framework is the right starting point. A structured current-state assessment that includes payer contract vintage, prior auth denial decomposition, and vendor technology currency will give you the operational grounding you need before the next budget cycle locks in assumptions that may not match where the payer landscape is heading.
The team at hfi.consulting works with health system and health plan finance leaders on exactly this kind of revenue cycle diagnostic. If you are navigating a leadership transition or a department restructure, reach out at hfi.consulting.
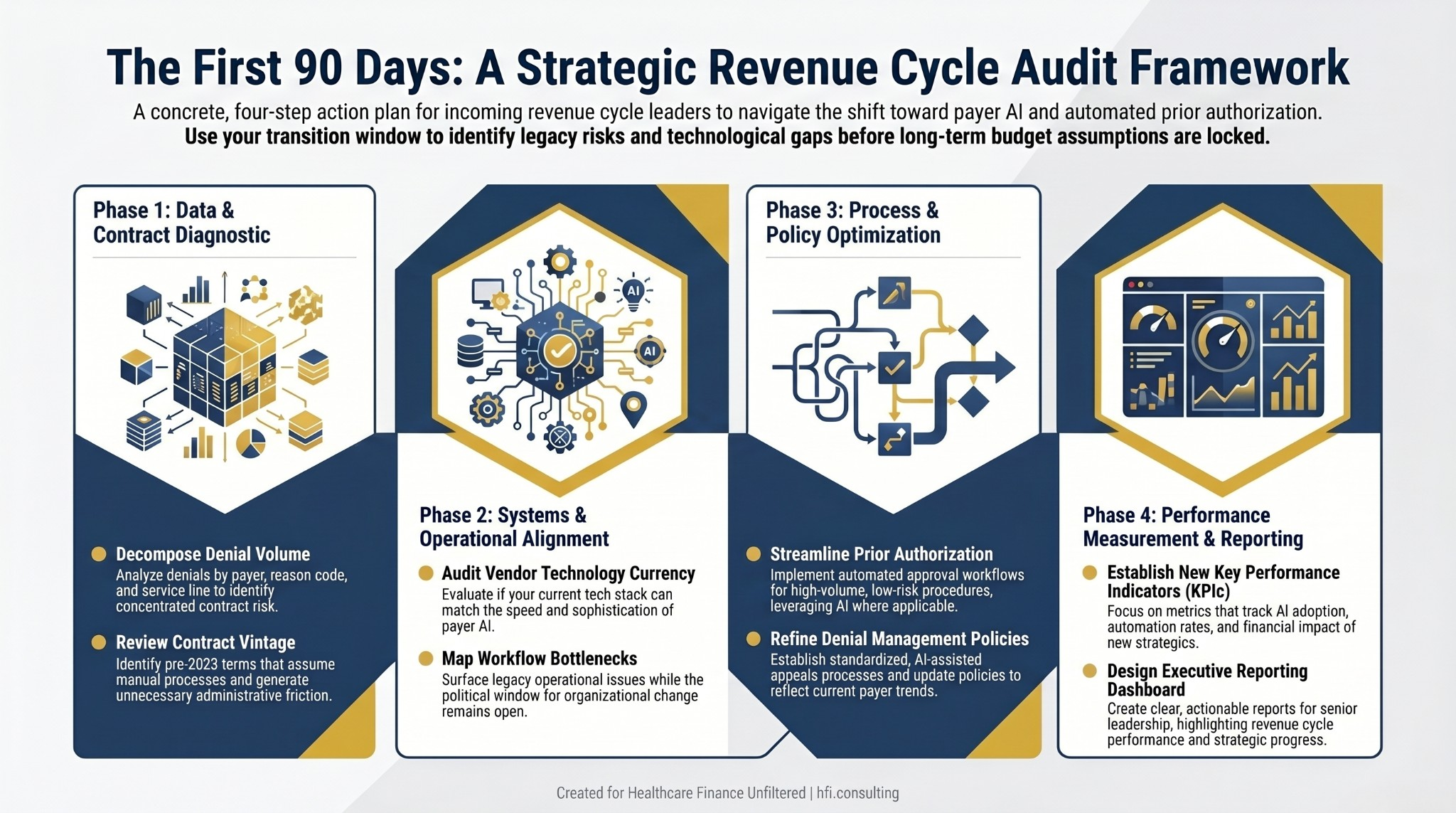
Four-step revenue cycle leadership transition audit framework showing denial decomposition, contract vintage review, vendor technology assessment, and workflow bottleneck mapping.
The Longer Play
The health systems recruiting right now are not hiring into a stable operating environment. They are hiring people to lead a function that is being restructured from both the inside and the outside simultaneously.
From inside, the expectation is analytical capability, CFO partnership, and AI governance. From outside, the payer landscape is automating prior auth, restructuring UM infrastructure, and deploying predictive models that change the composition of the cases that generate inpatient claims.
The RC leaders who do well in this environment will be the ones who treat the transition period as an intelligence-gathering exercise rather than a relationship tour. The operational map you draw in the first 90 days is the one you will navigate from for the next two years. Drawing it with the payer restructuring context in view is not optional. It is the difference between a current-state map and an already-outdated one.
For the AI in revenue cycle analysis that covers payer take-backs and what AI tools are producing at the hospital level.
For the medical group revenue cycle framing on high-deductible patient dynamics and why self-pay A/R is also part of the leadership transition picture.
The organizations that will navigate the next 24 months well are the ones whose revenue cycle leadership understands the payer side as well as the provider side. That is a harder profile to find than the job postings suggest. It is also the reason this many roles are open at once.
Are you moving into a new revenue cycle leadership role, or are you a CFO building the transition plan for one? The 90-day diagnostic framework applies whether you are the incoming leader or the executive sponsor. Reach out at hfi.consulting if you want to talk through the current-state assessment structure.
P.S. For those of you who have been through a revenue cycle leadership transition: what was the one thing you wish you had audited in the first 60 days that you did not? Hit reply. I read every response and the patterns are usually worth a follow-up piece.