
Offshore Medical Billing and AI: Who Is Actually Touching Your Revenue Cycle?
Most physicians and practice leaders never find out their billing has been sent overseas. Here is what to ask before you sign.
More than half of all U.S. medical billing is now handled by third parties. A significant portion of that work is performed offshore, often without the physician or practice leader ever knowing. If your billing company is charging under 7 to 8 percent of collections depending on specialty, the question worth asking is not whether they are good at their job. The question is how they are making the economics work.
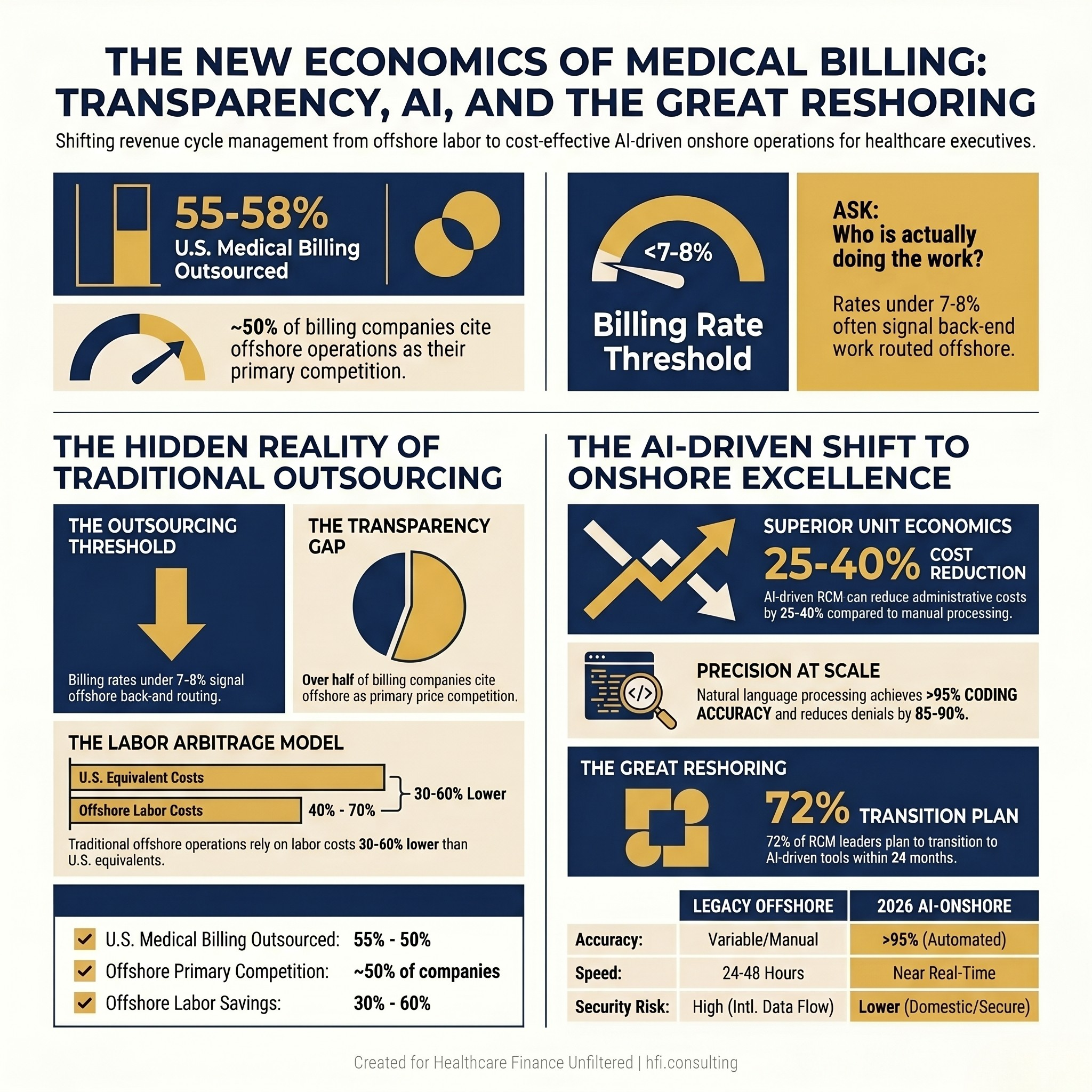
Two-column stat card showing U.S. medical billing outsourcing rates and rate thresholds that signal offshore operations.
The Offshore Billing Reality Most Practices Never See
The U.S. medical billing outsourcing market has become enormous. Industry estimates put the outsourced share of billing at approximately 55 to 58 percent of total market revenue, with that share growing steadily as administrative complexity increases and margins shrink. Within that outsourced segment, offshore operations in India, the Philippines, and nearshore locations like Colombia and Costa Rica handle a substantial portion of back-end work including coding, payment posting, and accounts receivable follow-up.
The business case for offshore operations has always been straightforward. Offshore labor costs 30 to 60 percent less than comparable U.S.-based staff. For billing companies competing on price, routing back-end tasks offshore is a standard operating model, not an anomaly.
The problem is not that offshore work happens. The problem is that it often happens without the client's knowledge or consent, and without a clear understanding of who has access to protected health information.
Low Rates Are Not Automatically a Red Flag. They Are a Prompt to Ask Questions.
A billing rate under seven or eight percent is not proof that something is wrong. Some companies operate efficiently, use technology well, and run lean domestic teams at competitive prices. However, a very low rate should prompt the same due diligence you would apply to any other major vendor relationship.
Consider what a billing company manages on your behalf. Insurance payments. Patient balances. Adjustments and write-offs. Claims submission and resubmission. Denial appeals. Financial reporting. And the protected health information of every patient in your system.
Most practice leaders would not hand their investment portfolio or banking credentials to an unknown third party without understanding who had access. Revenue cycle management deserves the same scrutiny. Your billing company touches your cash flow and your patients' data. That warrants more than a signed business associate agreement and a rate sheet.
What U.S.-Based Billing Companies Are Not Always Disclosing
Some U.S.-based billing companies are not fully transparent about operational structure with their clients. The gap is not always intentional concealment. Sometimes it reflects the complexity of the blended model: domestic front-end staff handling patient registration and eligibility, offshore teams handling coding and back-end follow-up, and subcontractors layered on top.
The questions that should be in every vendor evaluation include who is actually working the accounts day to day, whether back-end coding or AR follow-up is subcontracted to a third party, who has access to patient data and under what data security standards, how data is transmitted and stored, and who specifically handles denial escalations and appeals.
If a billing company cannot answer those questions clearly and in writing, that is meaningful information. The inability or unwillingness to explain operational structure is not a minor gap. It is a compliance and financial risk.
The Compliance Layer: HIPAA Does Not Stop at the Water's Edge
A common misconception is that offshore billing is automatically a HIPAA violation. It is not, provided the offshore vendor operates under a properly executed business associate agreement. However, a BAA is a contractual protection, not an operational guarantee.
The practical compliance risks in offshore billing arrangements are real. Data security standards, breach notification timelines, and enforcement mechanisms vary significantly across geographies. In 2024, major global cybersecurity incidents demonstrated that international data flows carry elevated exposure even when contracts are in order.
The denial rate environment makes this more urgent. Denial rates have reached as high as 46 percent in some reporting periods. High denial volumes generate high-stakes back-end work: complex appeals, payer-specific escalations, and claims that require judgment calls on clinical documentation. That is precisely the work that most requires domestic expertise, payer familiarity, and direct accountability.
I covered the full cost of the denial management problem in The Denial Loop Is Breaking Healthcare. The offshore billing structure makes that problem harder to solve, not easier.
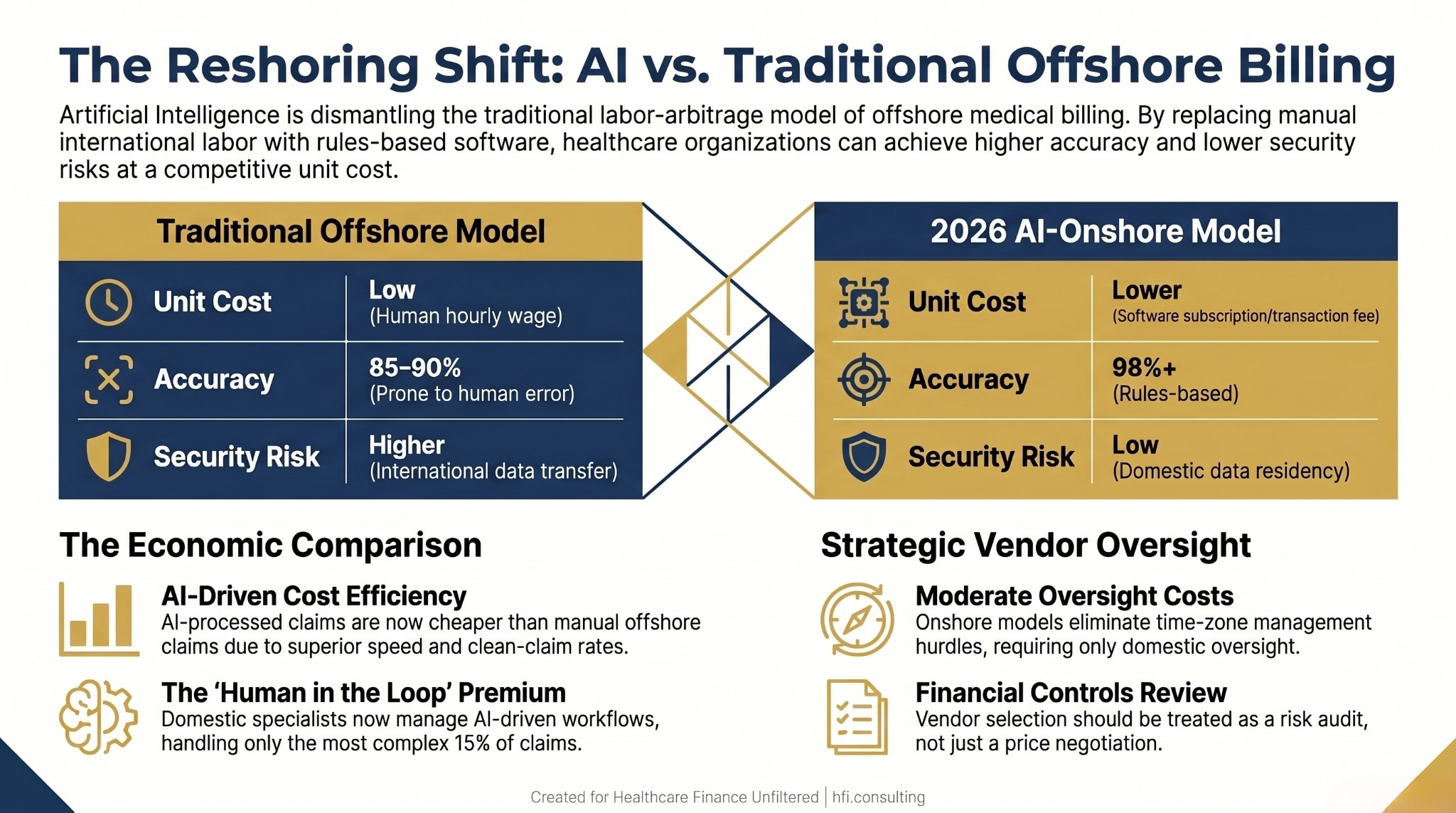
Comparison table showing legacy offshore billing model versus 2026 AI-onshore model across unit cost, accuracy, oversight cost, and security risk dimensions.
AI Is Changing the Math That Made Offshore Billing Attractive
For decades, the primary lever for reducing cost-to-collect was labor arbitrage. Moving manual billing tasks to lower-cost labor markets was the standard operating model for large RCM companies. AI is disrupting that model at the foundation.
Natural language processing tools can now examine clinical documentation and assign ICD-10, CPT, and HCPCS codes with accuracy rates above 95 percent. Processing times have been cut by 50 to 95 percent depending on claim type. AI-driven systems can identify high-risk claims before submission and flag errors proactively, reducing denial rates by 85 to 90 percent in documented deployments. Administrative cost reductions of 15 to 20 percent overall, with RCM cost reductions up to 25 to 40 percent, are appearing in early enterprise implementations.
The unit economics have shifted. An AI-processed claim is now cheaper than a manually processed offshore claim when you factor in speed, clean claim rates, and denial avoidance. Approximately 72 percent of revenue cycle leaders have moved or are actively planning to move outsourced functions to AI-driven tools within the next 24 months, according to industry surveys.
The "Great Reshoring" is not a hiring wave. It is an infrastructure shift. Health systems are not replacing 500 offshore staff with 500 domestic staff. They are returning data and oversight to U.S. soil and deploying smaller, highly skilled domestic teams to manage AI-driven workflows.
I covered the AI implementation framework for health systems in detail in AI in Revenue Cycle Management: The Enterprise Implementation Framework. The financial case for moving in this direction is no longer speculative. It is showing up in cost-per-claim calculations at systems that have made the transition.
The "Human in the Loop" Premium
Here is the nuance that makes the reshoring economics complicated: the humans left in the AI-enabled revenue cycle are more expensive, not less. Because AI now handles the routine 85 percent of claims, the remaining 15 percent are the hardest cases. Experimental procedures, complex multi-payer denials, appeals requiring clinical documentation review, and high-dollar implant billing disputes fall to the exception team.
That team is domestic, senior, and increasingly hard to find. Salaries for elite coders and revenue integrity managers have risen 20 to 30 percent in recent reporting periods. A single qualified domestic specialist can manage the output of an AI system doing the equivalent work of 20 to 30 offshore staff members. That math works at scale. At smaller practices, it is a more complicated calculation.
The bottom line: cost-to-collect is actually dropping for organizations making the AI transition. But the per-person cost of the humans in that system has gone up. That is not a contradiction. It is the new model.
"Your billing company isn't just doing data entry. They're managing insurance payments, patient balances, appeals, adjustments, financial reporting, and protected health information. Most practices treat vendor selection like a price negotiation. It should be treated like a financial controls review."
What to Ask Before You Sign
Cheaper is not always cheaper. Compliance exposure, revenue leakage, coding inaccuracy, communication delays across time zones, and lack of accountability in denial escalation all carry real financial cost. Those costs do not appear on the billing company's rate card. They show up in your AR aging, your denial write-offs, and your audit findings.
Before signing with any billing company, or before your current contract renews, the following questions deserve documented answers.
Who is actually working my accounts? Get a clear description of operational structure: who handles front-end registration and eligibility, who handles coding, who handles payment posting, and who handles denials and appeals. Ask specifically whether any of those functions are subcontracted to third parties.
Where is patient data stored and transmitted? Ask for documentation of data residency, transmission protocols, and the security standards applied to offshore data handling if applicable. Request the most recent SOC 2 Type II audit report if available.
What happens when a claim is denied? Understand the escalation path for denials. Ask how complex appeals are handled, whether that work stays domestic, and what turnaround standards apply.
What are the BAA terms if offshore work is involved? Review the BAA for breach notification requirements, indemnification language, and audit rights. A standard form BAA with an offshore subcontractor is not the same risk profile as a domestic arrangement.
In my time at Ascension across seven hospitals and later working on the payer side, I watched revenue cycle vendor relationships succeed or fail based primarily on transparency. The organizations that asked the hard questions upfront almost always had better outcomes than those that optimized on rate alone.
For a broader view of how AI is changing revenue integrity, AI-Powered Revenue Leakage Prevention: The CFO's Implementation Guide covers the implementation framework in detail.
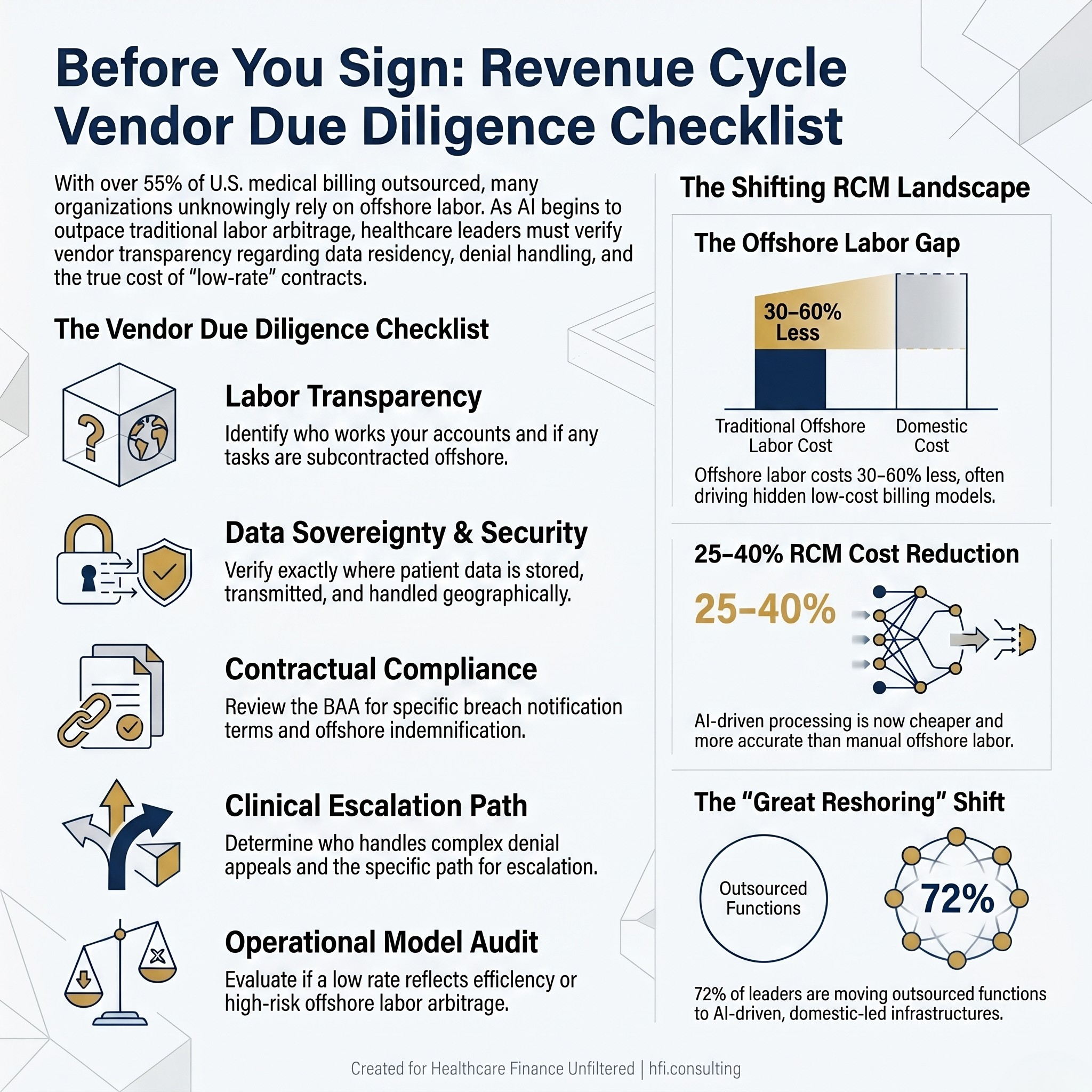
Five-item revenue cycle vendor due diligence checklist for evaluating offshore billing risk before contract signature.
The Financial Risk Framework for CFOs and Practice Leaders
Revenue cycle management is not a commodity function. It is compliance, cash flow, and financial protection for your organization. The vendors you select for that function have access to your most sensitive operational data and your most direct revenue stream.
For CFOs evaluating billing vendor relationships or preparing for contract renewal, the financial risk framework has three layers. First, revenue integrity: is coding accurate, are clean claim rates at or above 97 percent, and is denial volume being tracked with root cause analysis? Second, compliance exposure: is PHI handling documented, are BAA terms enforceable, and is audit trail integrity maintained regardless of where work is performed? Third, operational accountability: can you reach someone with authority when there is a problem, and are escalation paths clear?
The AI transition in revenue cycle management is real and accelerating. Organizations that understand the shift will make better vendor decisions and be better positioned to evaluate AI-driven alternatives when they come to market. Those that treat billing vendor selection as a pure price exercise will pay for it in ways that do not show up until the audit.
If you want to evaluate your current revenue cycle vendor relationships against these standards, or assess whether your cost-to-collect benchmarks are where they should be, HFI Consulting works directly with provider organizations on revenue cycle due diligence and performance benchmarking. Start the conversation at hfi.consulting.
The Bottom Line
The offshore medical billing market exists because labor arbitrage worked for a long time. AI is dismantling the economic foundation of that model by making software-based processing faster, more accurate, and cheaper than manual human labor regardless of geography.
That does not mean every offshore billing arrangement is a problem. It means that the market is changing quickly, that transparency requirements should be going up, and that low rates alone are no longer sufficient justification for a vendor relationship that touches your patients' data and your cash flow.
Ask who is touching your claims. Ask where your data is going. Ask what happens when a claim gets denied and it has to go to a human. Those are not hostile questions. They are the questions any competent financial steward should be asking.
For a detailed look at how AI is reshaping denial management specifically, read AI in the Revenue Cycle: How Hospitals Are Fighting Back Against Payer Take-Backs.
P.S. Have you ever discovered that your billing company was routing work offshore without disclosing it? Or have you had to go back to a vendor to ask hard questions about who was handling your accounts? Hit reply and tell me what you found. These conversations shape the next article.