
Medical Group Revenue Cycle: CFO and Director Strategies for the High-Deductible Patient Era
When patients owe more than ever, your collections strategy has to close the gap. Here's the framework.
Twenty-nine percent of American adults now rank healthcare costs as the most urgent problem facing the U.S. healthcare system. That number matters to your revenue cycle because it signals exactly how your patients feel before they walk into your waiting room. When patients are already anxious about what they owe, every friction point in your billing process is a collections risk you cannot afford.
High-deductible health plans have fundamentally changed the revenue cycle math for medical groups. What used to be a straightforward payer relations problem has become a consumer finance problem. Your front desk is now a bank teller. Your billing department is a loan servicer. And your CFO is accountable for a self-pay accounts receivable balance that will keep growing unless your strategy evolves to meet it.
This is not a theoretical concern for future planning cycles. It is the operating reality of 2026.
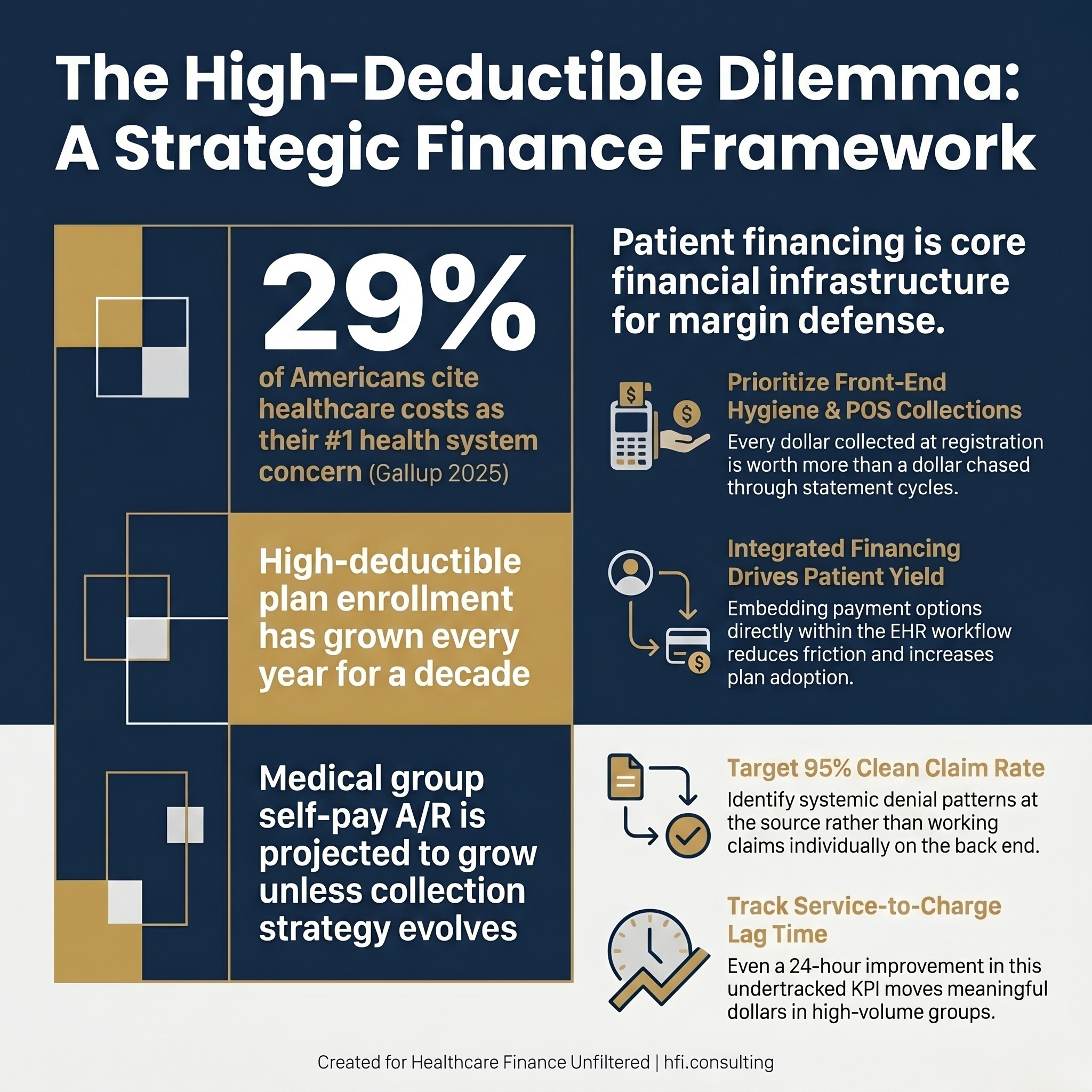
Three statistics about high-deductible health plans and patient financial responsibility in medical group revenue cycle management
The Medical Group Revenue Cycle Is a Different Animal
Before tackling patient payment strategy, it helps to understand what makes medical group revenue cycle operationally distinct from hospital billing. These are not the same problem at different scales.
A hospital revenue cycle is built around high-dollar, low-frequency events. A surgical case or an inpatient admission is complex, but the individual charge justifies the labor cost of working it. A medical group runs the opposite model: high-frequency, lower-dollar transactions across dozens or hundreds of providers, often across multiple specialties and locations.
When a hospital misses a $50,000 charge, that is a significant problem. When a medical group has a 5% error rate on $200 office visits across 500 providers, that is a catastrophe that compounds daily. The margin on each encounter is thin, and the cost of re-working a claim can sometimes approach the margin of the visit itself.
This is why the five priorities for a Revenue Cycle Director in a large medical group look different from a hospital billing director's agenda. Front-end hygiene and point-of-service collections are not aspirational goals. They are margin defense.
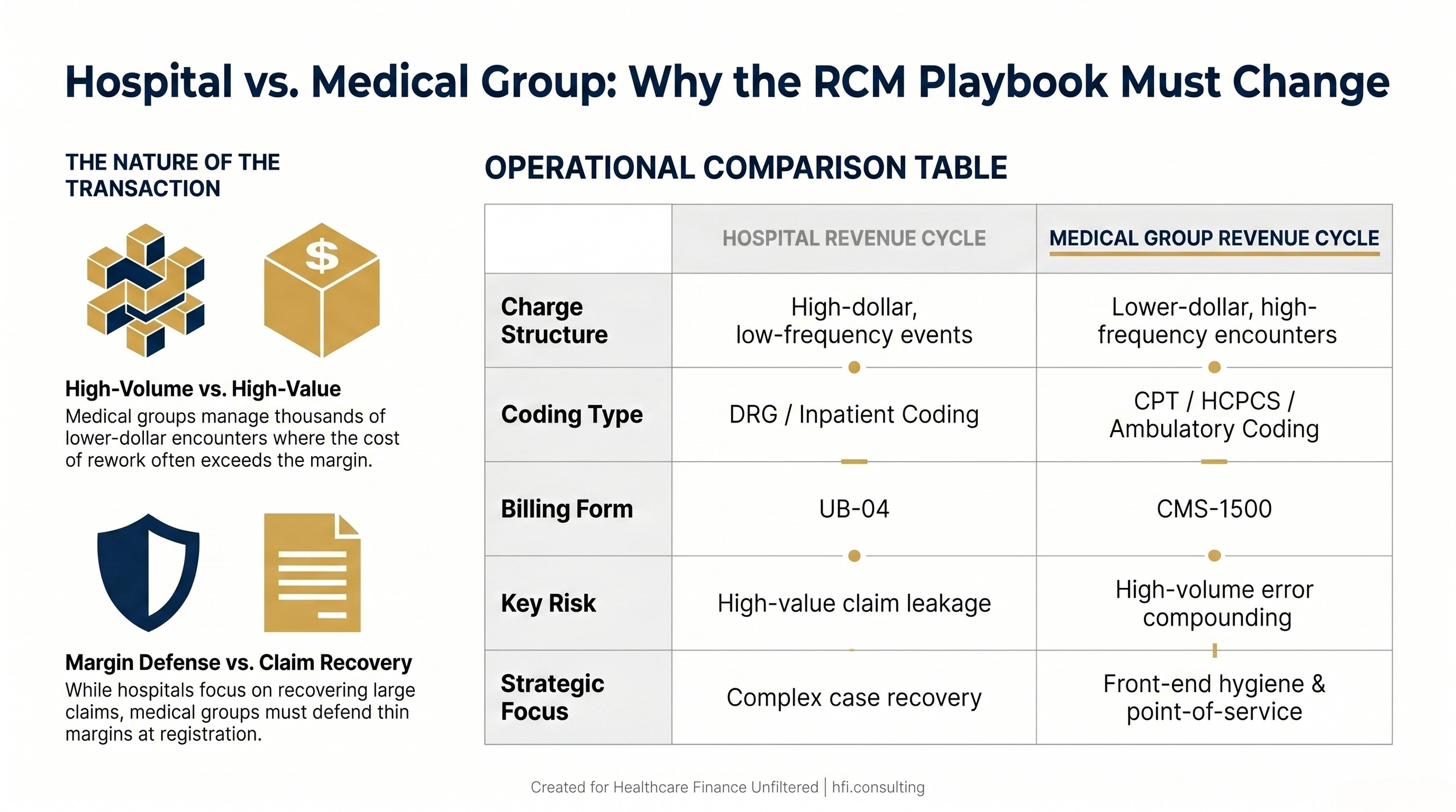
Comparison table showing the key operational differences between hospital revenue cycle management and medical group revenue cycle management for healthcare finance leaders
The Five Priorities Every Medical Group Revenue Cycle Director Is Managing Right Now
Front-End Hygiene and Point-of-Service Collections
Because medical groups operate on thinner per-encounter margins, the cost of claim rework relative to the value of the claim is disproportionately high. The financial logic is straightforward: if you do not collect at or before the point of service, you are financing patient balances at your own expense.
The practical goal is to capture accurate insurance information and collect patient responsibility before the patient leaves the building. Every dollar collected at registration is worth more than a dollar chased through a statement cycle. Methodist Health System's model, collecting 3-4% of patient responsibility upfront during pre-collections, illustrates what a deliberate front-end strategy looks like at scale.
Provider Productivity and RVU Tracking
Medical groups frequently compensate physicians on a productivity basis tied to work RVUs. This creates a direct link between clinical documentation quality and financial performance that many groups underestimate. If providers are not closing charts within a reasonable lag window, charges cannot be dropped and revenue sits uncaptured.
The Revenue Cycle Director's role here is to bridge clinical operations and financial output, not just process claims. Lag time from date of service to charge entry is one of the most undertracked KPIs in ambulatory billing, and in a high-volume group, even a 24-hour improvement in that metric moves meaningful dollars.
Payer Contract and Provider Enrollment Management
A single provider not properly credentialed with a major payer can generate months of out-of-network denials for their entire patient panel. In a growing medical group that hires regularly, this is not an edge case. It is a recurring operational risk. The enrollment pipeline from signed offer letter to billable provider must be managed as actively as the clinical onboarding process.
Denial root-cause analysis almost always reveals that provider enrollment and contract management gaps are driving a disproportionate share of write-offs, often far more than coding or documentation errors.
Denial Management and Pattern Identification
Medical group denials tend to be repetitive. The same modifier is missing across fifty claims. The same authorization step was bypassed for the same payer. These are not random errors; they are systems failures that need to be corrected at the source rather than worked individually on the back end.
A clean claim rate of 95% or higher is the target. Getting there requires pushing denial root-cause findings back to clinical staff and front desk teams with enough specificity to change behavior at the workflow level, not just at the billing level.
Patient Financial Experience and Self-Pay Collections
This is where 2026 is materially different from five years ago. As deductibles have risen and more financial responsibility has shifted to patients, the medical group's relationship with its patients has evolved into something that resembles consumer lending. The question is no longer whether to offer payment flexibility. It is how to structure it without compromising cash flow or operational capacity.
The Patient Payment Reality: What Finance Leaders Are Actually Facing
Working on revenue cycle projects at UF Health Jacksonville, a Level 1 Trauma and Level 3 NICU safety-net facility, I saw firsthand what happens when patient financial responsibility outpaces a community's capacity to pay. The populations most dependent on safety-net institutions are often the least equipped to navigate a billing statement, let alone a deductible explanation. That experience shaped how I think about the patient financial experience as a strategic finance problem, not just a collections problem.
A 2025 Gallup survey found that healthcare cost concerns are the top-of-mind healthcare issue for nearly a third of American adults. HFMA's own research found that cost anxiety prevents many patients from seeking care altogether. For a medical group, that means deferred care leads to deferred revenue, and eventually to worse outcomes that generate higher-acuity encounters down the line.
The financial imperative and the patient experience imperative are aligned here. When patients have manageable, transparent payment options, they are more likely to seek care, more likely to complete their course of treatment, and more likely to pay their balance.
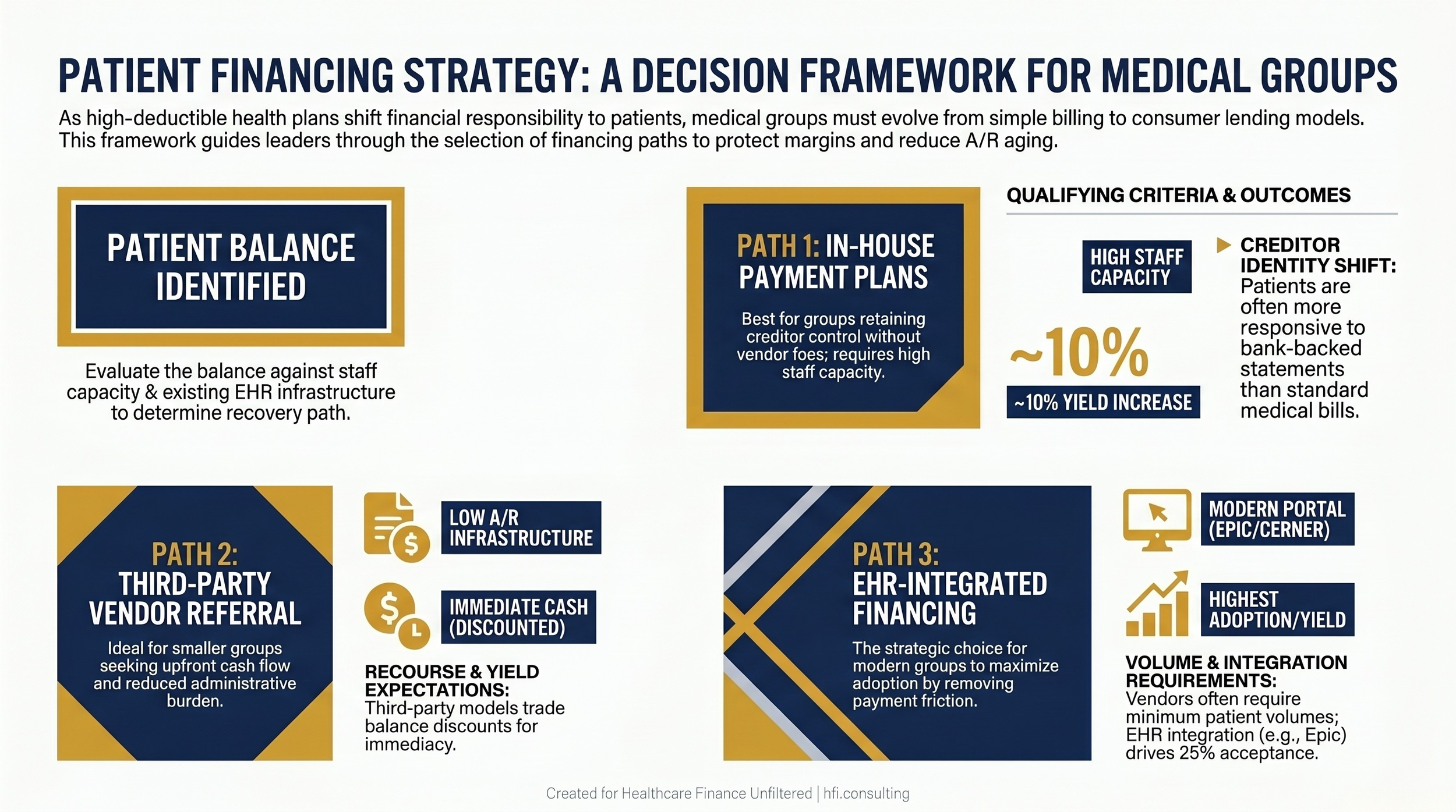
Decision flowchart for medical group CFOs selecting between in-house payment plans, third-party financing vendors, and EHR-integrated financing based on patient balance thresholds
Patient Financing: The Options Finance Leaders Are Evaluating
There is no single right answer for patient financing strategy. The right model depends on your group's size, payer mix, EHR infrastructure, and the financial profile of your patient population. Here is the framework for evaluating your options.
In-House Payment Plans
The simplest model. Your billing system manages the plan, and your organization retains the creditor relationship. The advantages are control and no vendor fees. The disadvantages are staff burden, collections risk if patients default, and the accounts receivable carrying cost. Endeavor Health's integrated Epic model, which saw a 10% yield increase and 25% patient acceptance on new financing plans, demonstrates what a well-designed in-house program can achieve when embedded directly into the patient workflow rather than offered as an afterthought.
Third-Party Vendor Programs
Outsourcing the financing relationship to a vendor removes your organization as the creditor and typically provides upfront payment for transferred balances. The tradeoff is that you accept a discount on those balances in exchange for immediacy and reduced staff burden. For smaller or rural groups with limited collections infrastructure, this model can be genuinely better than in-house alternatives.
Clark Fork Valley Hospital in Montana has run a third-party program successfully for seven years, including through periods when patient financing was not yet mainstream. The CFO there noted something operationally significant: patients are sometimes more responsive to a bank statement than a hospital bill. That shift in creditor identity changes the collections dynamic in ways that matter to your A/R aging.
For medical groups, the key evaluation criteria for vendor programs are: volume minimums (some vendors will not engage below a certain patient base), recourse terms if patients default, and the prescriptiveness of plan terms relative to your patient population's actual financial reality.
EHR-Integrated Financing
This is the direction the market is moving, and it matters because integration determines whether patients actually use the financing option you offer. If a patient has to navigate away from your payment portal to a separate vendor experience, acceptance rates drop. When financing is embedded in the same digital environment where they would otherwise make a standard payment, friction decreases and adoption increases.
Epic's integration capabilities have become a reference point for how EHR-based financing should work. The goal is a trigger built into the existing payment experience, not a separate link that sends patients somewhere else. This is not a technology preference; it is a collections strategy, because an unused option has zero yield.
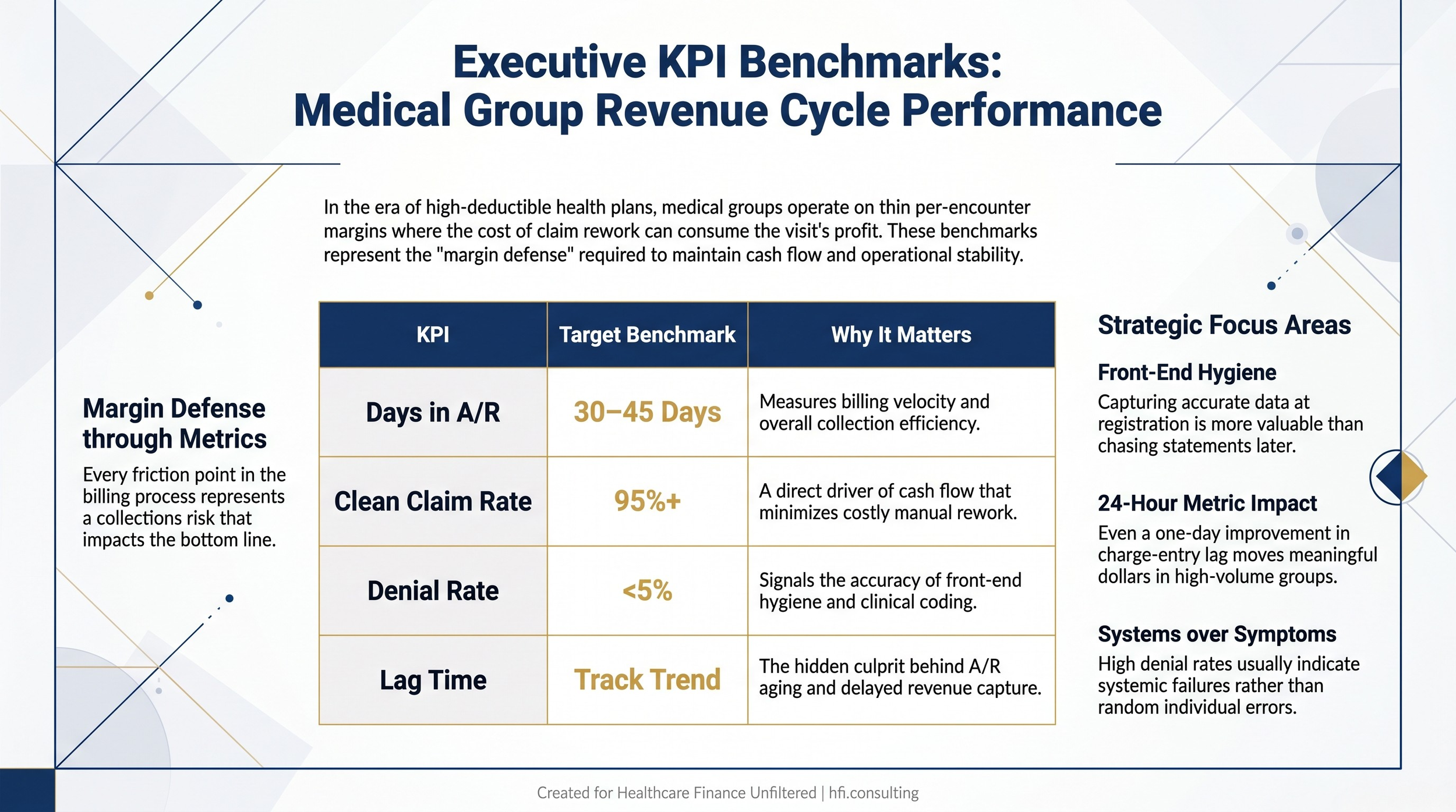
KPI benchmark table for medical group revenue cycle directors showing target ranges for days in A/R, clean claim rate, denial rate, and charge lag time
What CFOs Need to Be Planning for Right Now
The patient financing conversation is moving from discretionary program to core infrastructure. HFMA roundtable participants were direct about this: patient financing is no longer a nice-to-have. It is becoming an expected element of the provider-patient financial relationship, especially as high-deductible plans continue to push more responsibility onto individuals.
For CFOs, this requires a few specific planning actions.
First, project your self-pay A/R trajectory over the next three to five years using your current payer mix trends. High-deductible enrollment has been growing for a decade and shows no sign of reversing. Your self-pay A/R will grow proportionally unless your collections strategy improves.
Second, evaluate your current patient financing offering against the criteria above: integration, recourse structure, volume thresholds, and plan flexibility. If you do not have a documented financing option, you are already behind peer groups.
Third, train your front-desk and financial counseling staff on the patient communication side. Accurate financial estimates provided before service is a documented driver of payment plan adoption. UW Health's experience with pre-service payment plan enrollment, while not achieving the adoption rates they hoped for initially, reflects the right directional strategy. Getting the estimate right before the visit changes the conversation entirely.
Fourth, consider your KPI dashboard. Days in A/R for a medical group should be 30 to 45 days. Clean claim rate should be 95% or higher. Denial rate should be under 5%. Lag time from service to charge entry is the undertracked metric that often explains why the other numbers are not where they should be.
The Vendor Evaluation Question Finance Leaders Keep Avoiding
One of the consistent patterns I observed during Performance Analytics implementations at McKesson, now Change Healthcare, was that finance leaders often evaluate revenue cycle vendors on feature lists rather than operational fit. A vendor with a compelling demo and a shallow integration capability will create reconciliation problems that cost more to fix than the program saves.
For patient financing vendors specifically, ask for live demonstration of the EHR integration, not a slide deck. Ask what happens when a patient defaults and whether the recourse terms are clearly defined in the contract. Ask what your volume floor is and what the program looks like for your lowest-balance accounts, because those are often the ones your front desk will be most tempted to skip.
The reconciliation burden is real. Clark Fork Valley Hospital noted that recourse accounts returning from their vendor are an operational challenge precisely because it does not happen often enough to make the workflow automatic. Design your process before you need it, not after.
If you are evaluating patient financing vendors or redesigning your medical group's revenue cycle strategy, the Patient Collections Strategy Workbook I developed covers the key decision criteria, KPI benchmarks, and vendor evaluation framework in a format your team can work through before your next leadership meeting. You can access it at hfi.consulting
The Bottom Line for CFOs and Revenue Cycle Directors
The patient is now your most complex payer. They arrive with anxiety about what they owe, limited financial literacy about their own insurance, and a low tolerance for billing friction. Your revenue cycle strategy has to account for all of that without adding labor costs you cannot sustain on 2-3% margins.
The medical groups that will protect their revenue in this environment are not the ones with the most sophisticated billing software. They are the ones whose patient financial experience is clear, flexible, and integrated from the first encounter estimate through the final payment. That is a CFO-level strategic decision, not a billing department tactical issue.
Treating patient financing as core infrastructure rather than a program option is the mindset shift this environment requires.
Healthcare Finance Unfiltered covers the operational and financial decisions that rarely make it into the trade press. If you are working through a revenue cycle restructuring or evaluating your patient payment strategy, reach out through hfi.consulting The frameworks are free. The thinking is yours to apply.
P.S. What is the single biggest gap in your medical group's patient collections process right now? Is it front-end hygiene, payment plan adoption, or something else entirely? Hit reply and tell me. I read every response.