
Epic Is the EHR Market: A CFO's Guide to Contract Strategy When Leverage Is Limited
What Judy Faulkner's "profit is a side effect" philosophy actually means for your next Epic negotiation.
Epic's CEO Judy Faulkner recently told a podcast that profit is "a side effect, not a goal," and her company's $6.7 billion in 2025 revenue suggests the side effect is doing just fine. For every CFO sitting across a contract table from Epic, that philosophy has a financial translation: the rules are set, the market is consolidated, and the leverage most vendors leave on the table simply does not exist here. Understanding what that structure actually means for your organization is the first step toward protecting your margins.
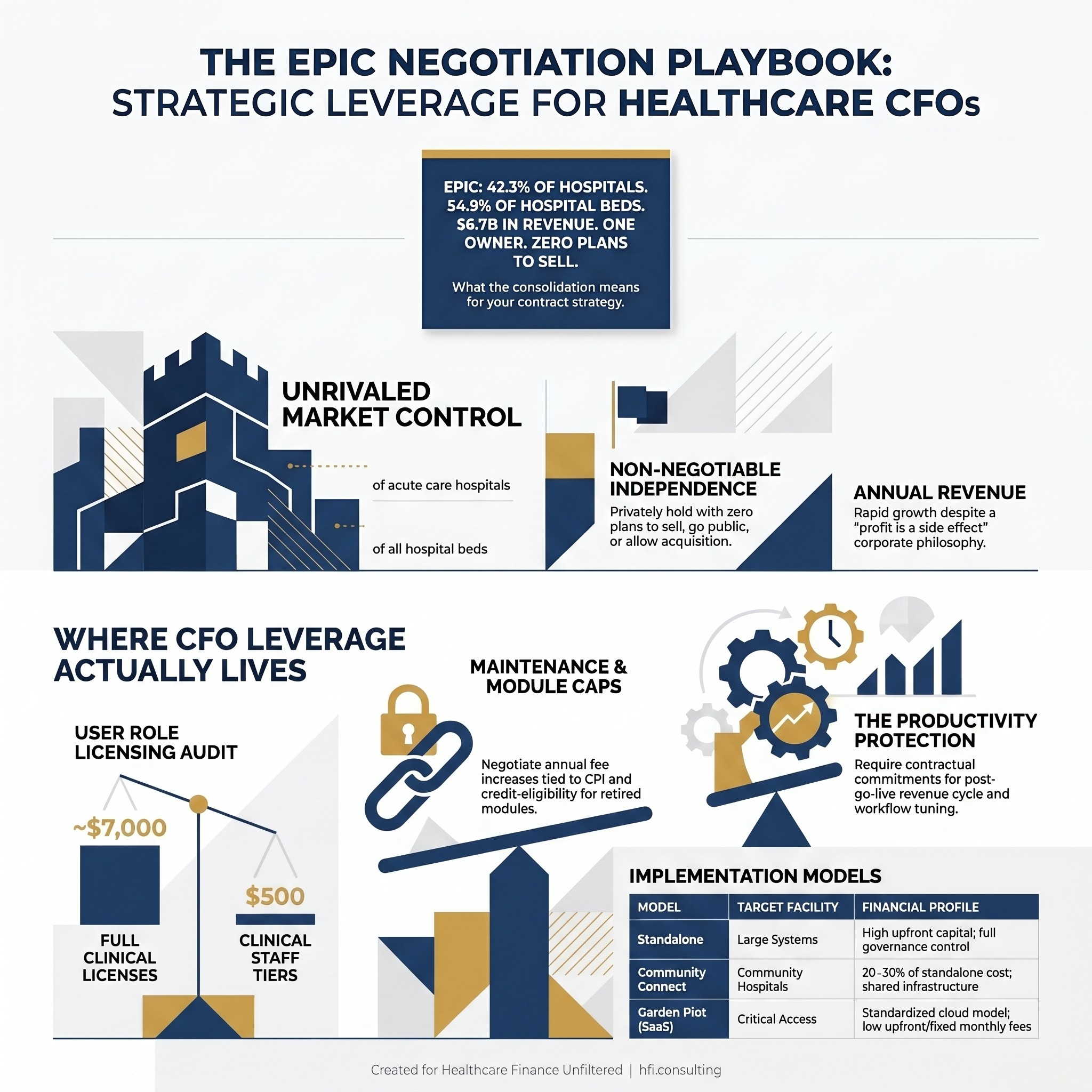
Infographic showing Epic's 2025 market statistics, 42.3% hospital market share, 54.9% of beds, $6.7B revenue, privately held
Epic's founder and CEO Judy Faulkner recently said something that stopped a lot of finance leaders mid-scroll. In an interview with Freakonomics Radio, she agreed with the host's observation that Epic is "not profit maximizing at all." Her explanation: "Our customers need it more than we do, and so we don't want to misuse them."
Sounds generous. But Epic's revenue climbed from $5.7 billion in 2024 to $6.7 billion in 2025. And the company just had its largest net gain of hospital customers on record, adding 108 hospitals across 10 major health systems in a single year.
Faulkner's framing is genuine. It also does not change the negotiating dynamics you are facing.
The Market Reality Every CFO Needs to Internalize First
Per KLAS Research, Epic now holds 42.3% of acute care hospitals and 54.9% of hospital beds in the United States. Its nearest competitor, Oracle Health (formerly Cerner), sits at 22.9% of hospitals and 22.1% of beds. MEDITECH holds 14.8%.
In 2024, Epic's Community Connect program alone captured nearly 70% of all hospitals involved in an EHR decision. That figure tells you everything about the gravitational pull of Epic's ecosystem. Health system giants including Trinity Health, Northwell Health, UPMC, and Intermountain Health are either implementing or recently went live with the platform.
This is not a vendor with competitive pressure forcing concessions. Epic has famously never gone public, never taken venture capital or private equity, and has never acquired another company. Faulkner has already structured her succession plan to keep it that way permanently. A trust governed by family members and senior managers, backed by a group of health system CEOs legally committed to enforcing her wishes, will ensure Epic remains private and independently owned after she is gone.
She also rejected a $30 billion acquisition offer. The answer was: "Not now and not in the future."
CFOs who approach an Epic contract assuming competitive tension will drive price down are working from the wrong model. The leverage that exists elsewhere in healthcare vendor negotiations simply does not apply here. What does exist is a different kind of leverage, and it is worth knowing precisely where to find it.
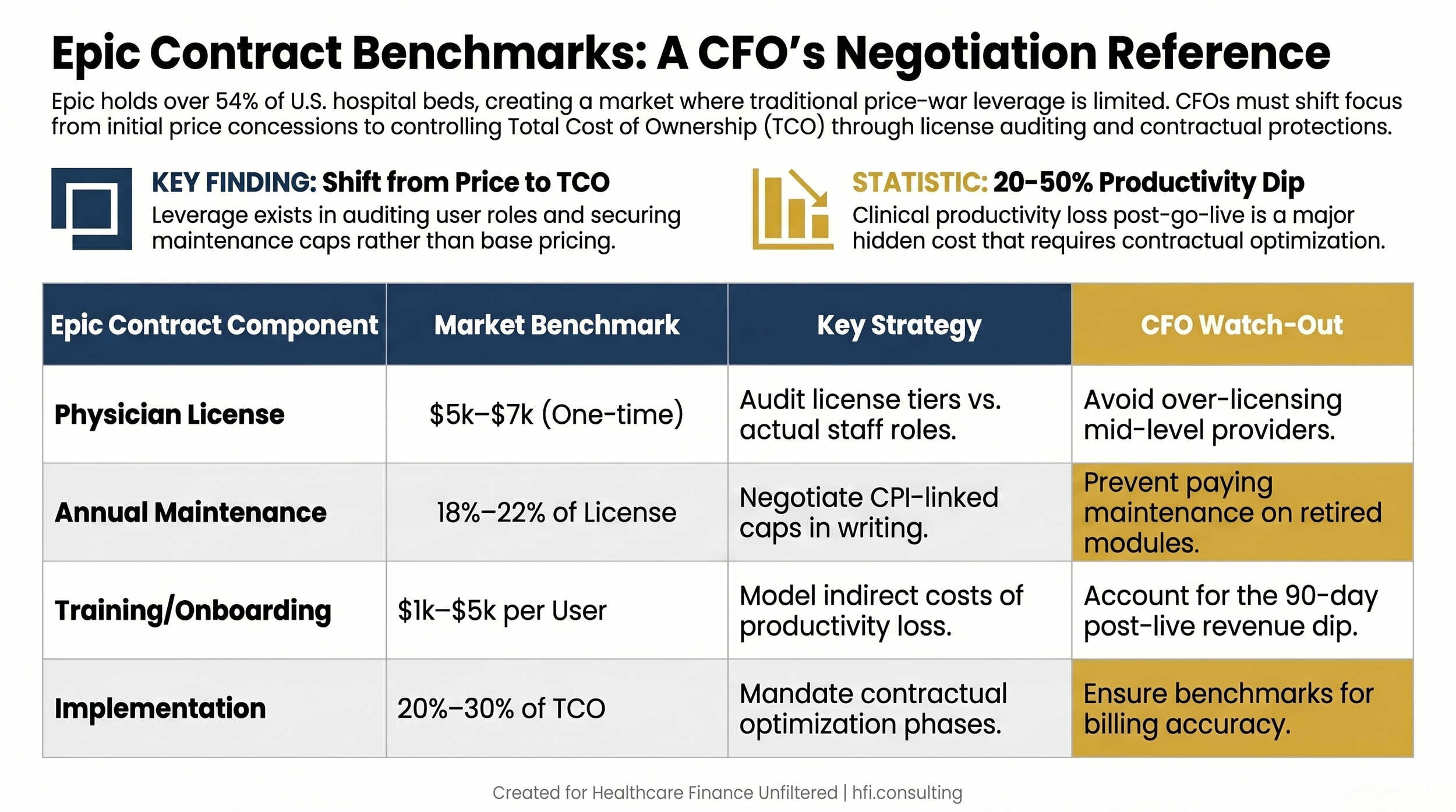
Table comparing Epic contract pricing benchmarks with CFO watch-out considerations for each component
Where CFO Leverage Actually Lives in an Epic Negotiation
The mistake most finance teams make is treating Epic contract strategy the same as a supply chain negotiation. It is not. The opportunity is not in winning a price war. It is in controlling total cost of ownership over a multi-year implementation cycle. That is a different discipline.
User role auditing is where most systems leave the most money. Epic's pricing is heavily anchored to "Full Clinical Access" physician licenses, which typically run $5,000 to $7,000 as a one-time perpetual cost. Clinical staff licenses, used by medical assistants, billing clerks, and residents who do not require full access, typically range from $500 to $3,000. In my work at Ascension across seven hospitals, the gap between what a system licensed and what staff actually needed for their daily workflow was consistently wider than leadership expected.
Before signature, your team should audit every planned user role against Epic's license tiers. This is not a theoretical exercise. On a 500-physician implementation, the difference between appropriate licensing and default over-licensing can reach seven figures.
Annual maintenance fee language matters more than the initial contract price. Epic's standard maintenance and support fees run approximately 18 to 22 percent of initial licensing cost annually. Without specific contractual language, those fees grow as you add specialty modules, Beaker for Lab, Cupid for Cardiology, Willow for Pharmacy, and others in Epic's extensive ecosystem.
The goal is to negotiate a maintenance cap that ties annual increases to a fixed percentage or to the Consumer Price Index. Equally important: ensure that any modules you retire are credit-eligible toward new modules. Without this language, you will pay maintenance on shelfware.
The productivity dip is the hidden cost that never shows up in the vendor's ROI presentation. Clinical productivity typically drops 20 to 50 percent during the first 90 days post-go-live. The financial impact runs directly into your revenue cycle: charge capture integrity, coding accuracy, and claims turnaround all suffer during transition. When I was supporting McKesson's Change Healthcare Performance Analytics implementations, the systems that recovered fastest were those where the contract specified explicit optimization commitments, not just go-live support.
Before signing, require that Epic or your implementation partner commit contractually to specific at-elbow support hours and post-go-live revenue cycle workflow tuning. If the contract does not include performance benchmarks tied to charge capture and billing accuracy, you are absorbing that recovery cost entirely.
Module sprawl is the budget leak that compounds over time. Epic's ecosystem is broad. It is easy for department leaders to assume that buying more Epic modules eliminates integration costs, but that logic does not always hold financially. Before purchasing any new Epic module, run a functional gap analysis comparing the module cost against maintaining your current best-of-breed solution with an integration fee. Keeping a specialized third-party analytics or pharmacy tool and paying the FHIR integration cost is sometimes the better financial outcome.
A Different Equation for Smaller Organizations
The calculus changes significantly depending on your facility type and size. What works for a 400-bed regional system is not the same playbook for a 25-bed Critical Access Hospital.
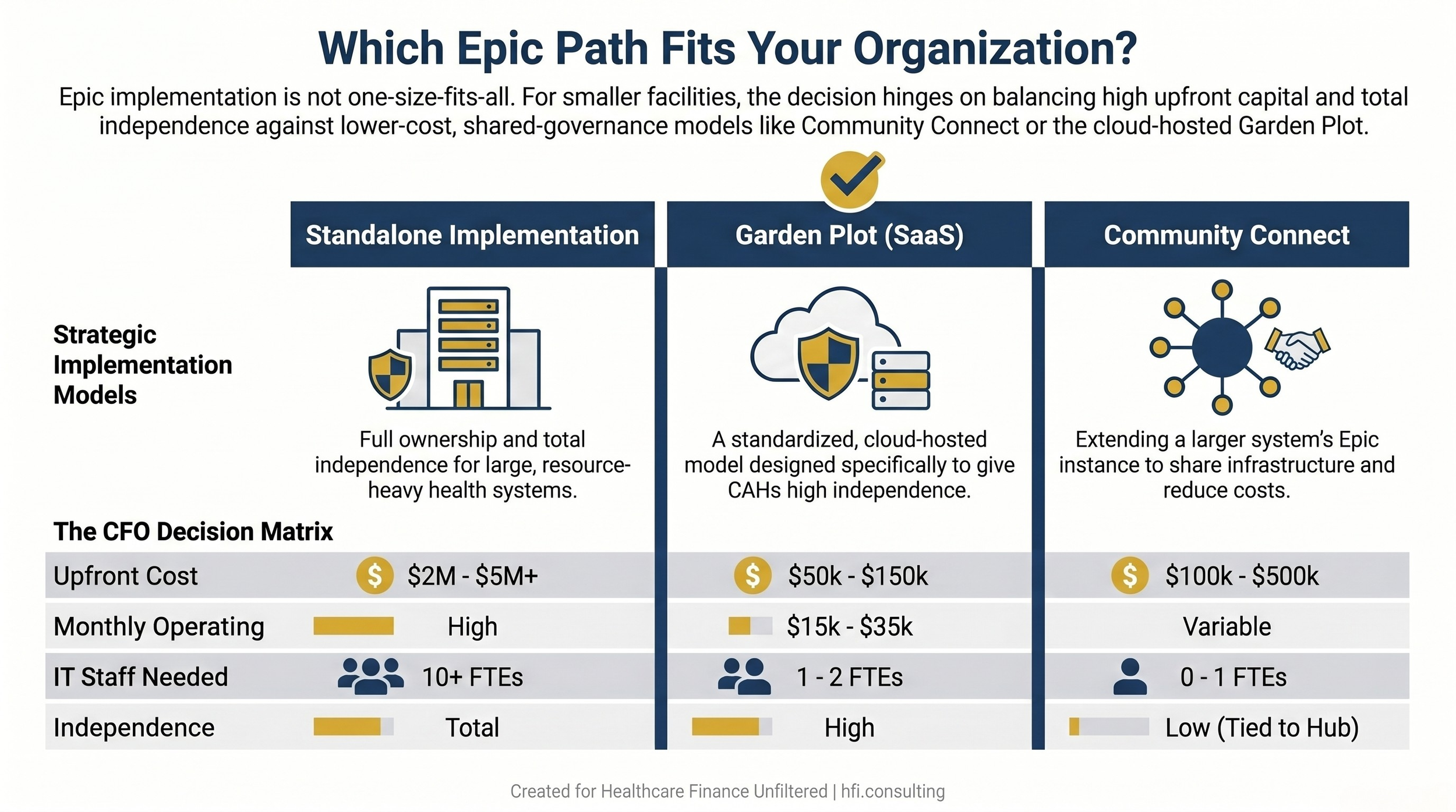
Comparison table of three Epic implementation models, standalone, Garden Plot SaaS, and Community Connect, with cost and staffing data
For community hospitals, the most financially sound path in 2026 is often not a standalone Epic implementation. Epic's Community Connect program allows smaller organizations to extend a larger regional system's existing Epic instance. The cost is typically 20 to 30 percent of what a standalone implementation would require, with shared IT infrastructure and support absorbed by the hub system.
The strategic tradeoff is real: you are tying your organization to the hub system's roadmap and governance decisions. For a facility that is already part of a larger system or has a clear affiliation path, that is often acceptable. For an independently governed community hospital, the dependency question deserves careful board-level discussion before signing.
For Critical Access Hospitals, Epic's Garden Plot SaaS model has changed the access equation. Garden Plot shifts the delivery to a standardized cloud-hosted model where Epic handles hosting, security, and updates. Upfront costs typically run $50,000 to $150,000 with monthly operating fees in the $15,000 to $35,000 range, compared to the $2 million to $5 million or more required for a standalone implementation. The trade is flexibility: Garden Plot is a standardized build with limited customization.
The Rural Health Transformation Program, funded at $10 billion annually starting in 2026, is creating new financial pathways for CAHs pursuing EHR modernization. CMS has capped direct EHR replacement funding at 5% of total award allocations, which means CFOs are categorizing related spend under interoperability modernization and cybersecurity infrastructure to close the gap. If your organization has RHTP funding in the pipeline, your finance team should be working closely with your compliance and grant management teams to structure Epic-related expenditures appropriately within those frameworks.
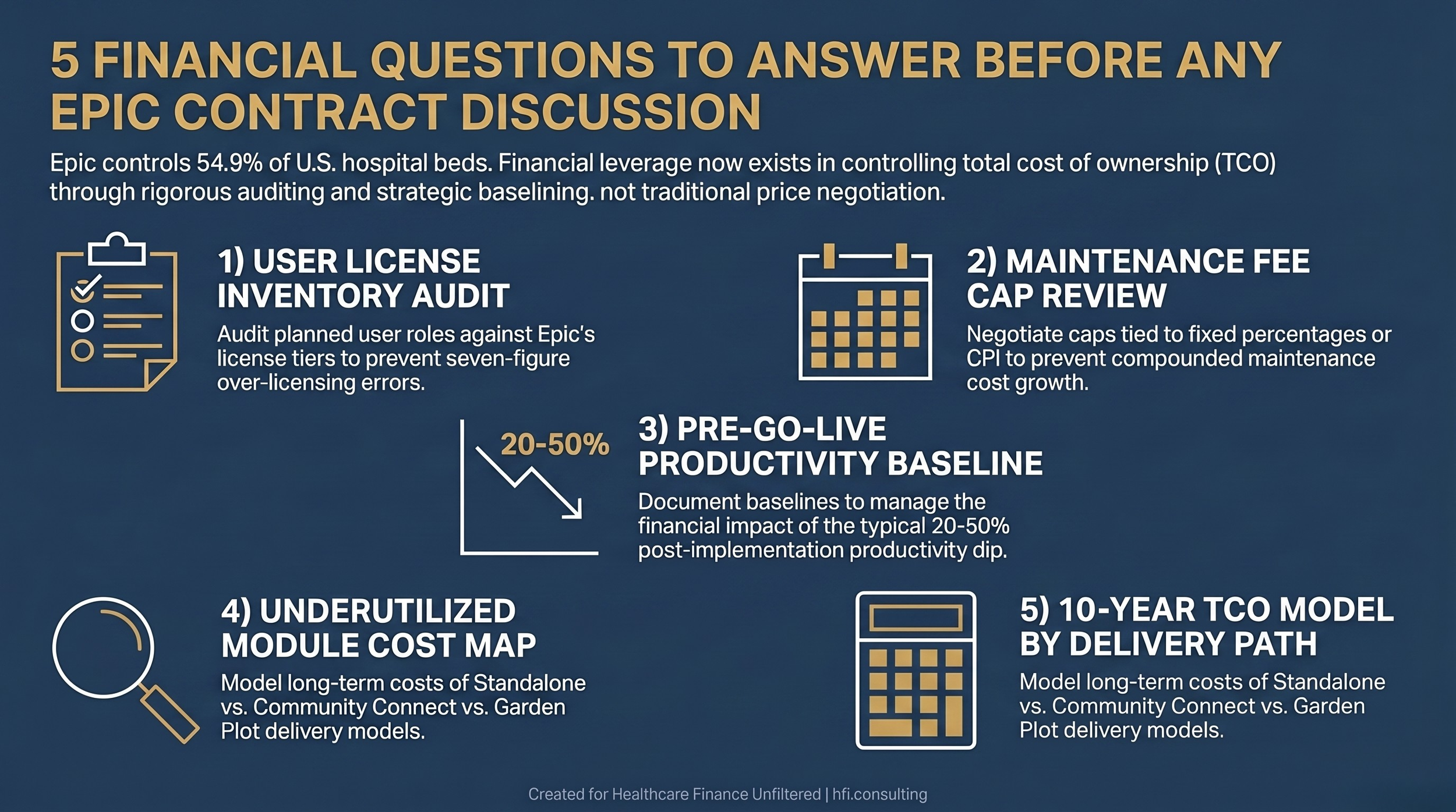
Five-step checklist for healthcare CFOs to prepare for Epic contract negotiations, covering licensing, maintenance, productivity, and total cost of ownership
The Competitive Landscape Is Worth Understanding Even If It Does Not Change Your Decision
Epic's dominance does not mean the alternatives have stopped competing. Oracle Health is actively investing in cloud infrastructure and AI-enabled simplification, particularly in the mid-market. MEDITECH Expanse remains a credible enterprise option for mid-sized systems at significantly lower implementation cost and with a "clinician-first" positioning that has real workflow advantages for nursing-heavy environments.
For organizations not yet on Epic, the value of understanding these alternatives is not necessarily in choosing them. It is in having a credible alternative narrative that occasionally moves the needle in your Epic discussions. The alternative options also matter for subsidiary entities and joint ventures: a community clinic affiliate or behavioral health subsidiary may be far better served by Athenahealth's cloud-native revenue-sharing model than by a Community Connect extension that carries more administrative overhead than the entity can absorb.
The emerging ambient AI layer, platforms like Abridge and Suki that sit on top of any EHR to handle documentation, deserve specific mention in your capital planning conversations. These tools do not replace Epic, but they significantly reduce the clinician friction that drives adoption resistance and productivity loss post-implementation. The CFOs who are getting the best ROI on their Epic investments are increasingly bundling ambient AI into the implementation budget, not treating it as a separate future consideration.
The Faulkner Philosophy and What It Means Operationally
Understanding Faulkner's philosophy is not an academic exercise. It provides real operational guidance for how to manage the relationship over time.
Epic's stated position is that customers should be able to work with any third-party vendor they choose. Faulkner has said explicitly that a consistent part of Epic's job is helping customers understand what they already bought, because organizations frequently purchase third-party tools that duplicate capabilities already in their Epic license.
That framing is an invitation. Before your next contract renewal or module add, pull your existing Epic license inventory and have your IT team audit what is active, what is unused, and what new vendor pitches you are receiving for capabilities already in your build. You are likely sitting on unlicensed value, and identifying it costs nothing.
Epic has also been notably consistent on two things that CFOs should bank on: the company does not litigate against customers (Faulkner has stated no customer has ever sued Epic, and only one has ever left, before eventually returning), and the private structure means you will never face the pricing pressure dynamics that come from a publicly traded vendor needing to hit quarterly targets.
That consistency is worth something. Long-term planning assumptions about this vendor relationship are more stable than for most large technology partners. Model it accordingly.
The financial exposure you are managing with Epic is less about the initial contract and more about implementation quality, adoption, and total cost optimization over a seven to ten-year horizon. Finance leaders who focus there, rather than on a negotiation posture that the market structure does not support, will protect more margin.
If your organization is currently in an Epic contract cycle and you want to think through the financial modeling on a Community Connect versus standalone versus Garden Plot decision, that is exactly the kind of analysis my practice focuses on. Visit hfi.consulting to start a conversation.
Building Your Internal Epic Financial Framework
Before you enter any negotiation or renewal discussion, your finance team should be able to answer five questions:
What is your current user license inventory by tier, and does it match your actual clinical workflow map?
What is the contractual cap, if any, on annual maintenance fee increases, and when does it expire?
What is your documented productivity baseline before go-live, and what is your contractually committed recovery timeline?
Which modules in your current build are underutilized, and what is the annual maintenance cost on those licenses?
If you are a CAH or community hospital, have you modeled the true ten-year TCO comparison between standalone, Garden Plot, and Community Connect including IT staffing, infrastructure refresh, and affiliation risk?
These are not questions Epic will answer for you. They are the financial foundation of a well-managed relationship with the market's dominant EHR vendor.
For deeper analysis on healthcare technology investment ROI and EHR financial modeling, see our earlier work on AI-Powered Revenue Leakage Prevention: The CFO's Implementation Guide and our coverage of CMS Medicaid Fraud Crackdown 2026: What Hospital Finance Leaders Must Do Now.
If you are navigating an Epic implementation, renewal, or build optimization and want a finance-side review of your current contract structure, hfi.consulting is where that work happens.
P.S. Which Epic cost element has surprised your organization the most, the implementation productivity dip, the module sprawl, or something else entirely? Hit reply and tell me. I read every response.