
Hospital Price Transparency 2026: The CFO's Guide to Publishing Data Patients Can Use
CMS enforcement is live. Here's how to move from MRF compliance to patient utility.
CMS enforcement of the updated hospital price transparency requirements began April 1, 2026. Your machine-readable file likely meets the new technical specifications. The median allowed amounts are posted. The 10th and 90th percentile figures are encoded. A named senior official has signed the attestation.
And yet, the patient who just received a bill for a 90-minute emergency department visit still cannot tell you what they will owe before it arrives.
That gap between regulatory compliance and patient utility is where healthcare finance leaders need to focus their attention right now. Not because CMS is watching, but because the cost of confusion has become a measurable operational and clinical risk.
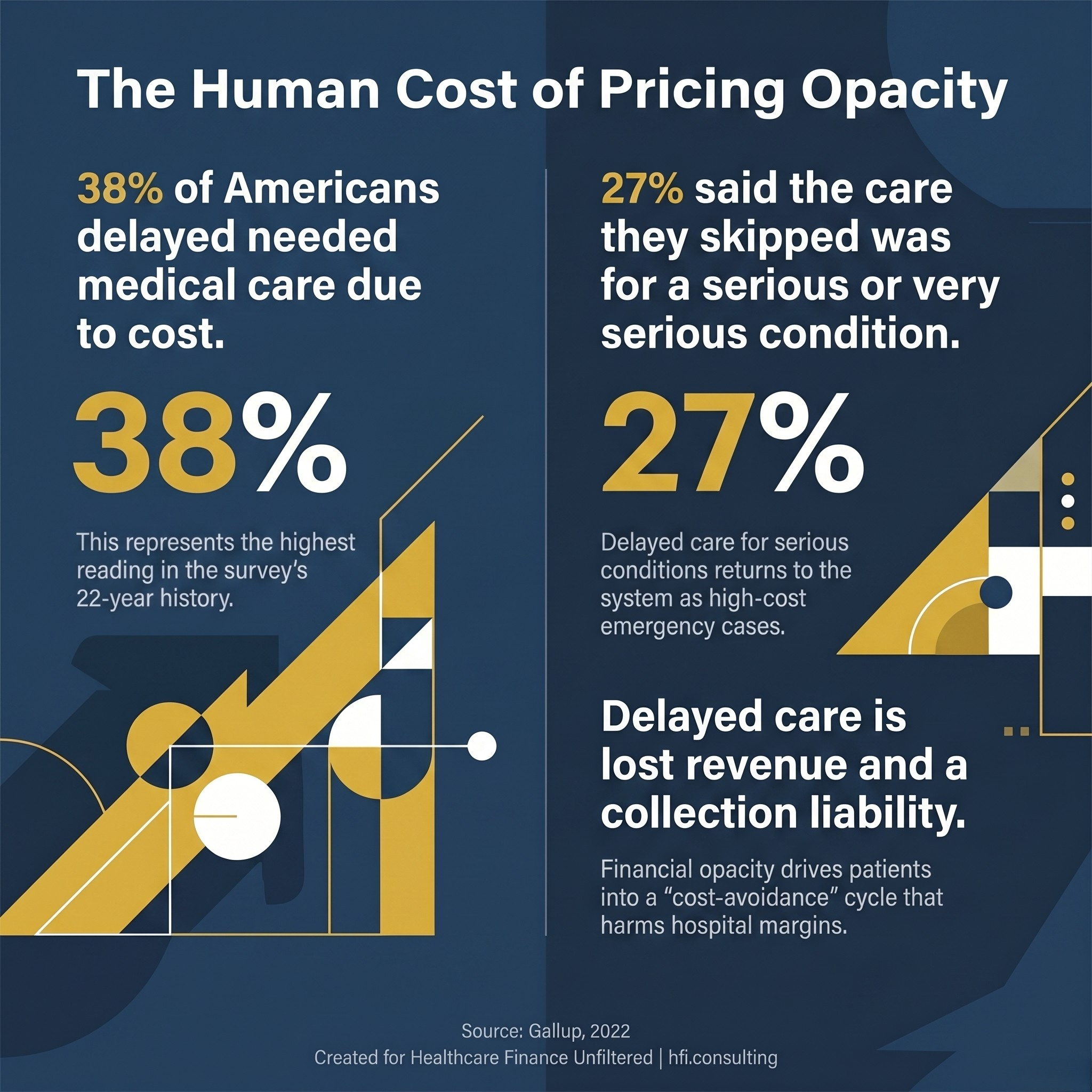
Gallup stat card showing 38 percent of Americans delayed care due to cost in 2022, with 27 percent reporting the condition was serious.
What CMS Actually Changed in 2026
The CY 2026 OPPS Final Rule, effective January 1, 2026 and actively enforced since April 1, 2026, made several meaningful upgrades to what hospitals must publish. The changes target a long-standing problem: hospitals were posting estimated allowed amounts that bore little relationship to what payers actually paid.
Under the new requirements, hospitals must replace the estimated allowed amount with the median allowed amount, calculated from actual EDI 835 remittance data, and disclose the 10th and 90th percentile allowed amounts. The lookback period for these calculations must be 12 to 15 months. Hospitals are also now required to include Type 2 National Provider Identifiers in their machine-readable files, enabling better cross-system comparability.
CMS also finalized an attestation requirement. A named hospital CEO, president, or designated senior official must certify that the data is true, accurate, and complete. That named accountability is new, and it matters operationally.
The penalty structure has also shifted. CMS will reduce civil monetary penalties by 35 percent when a hospital waives its right to an ALJ hearing. Hospitals that fail to post a machine-readable file entirely, or fail to make shoppable services available in a consumer-friendly format, are ineligible for that reduction.
Compliant Does Not Mean Useful
Here is the honest assessment: most hospitals will meet the letter of these requirements without meaningfully improving what patients experience.
The machine-readable file is exactly that. Machine-readable. The median allowed amount for a knee replacement at your facility, expressed as a data element in a CSV or JSON file, does not tell a patient with a $4,000 deductible, 20 percent co-insurance, and a high-deductible health plan what they will owe after the claim processes.
That is not a critique of the regulation. It is a structural reality about how healthcare pricing works.
The file captures what the hospital and payer negotiated. It does not tell a patient where they sit in their deductible cycle, whether their specific plan applies the negotiated rate or a separate methodology, whether the anesthesiologist in the room is in-network, or whether the facility fee and physician fee will arrive as two separate bills from two separate billing entities.
The Billing Maze No Single File Solves
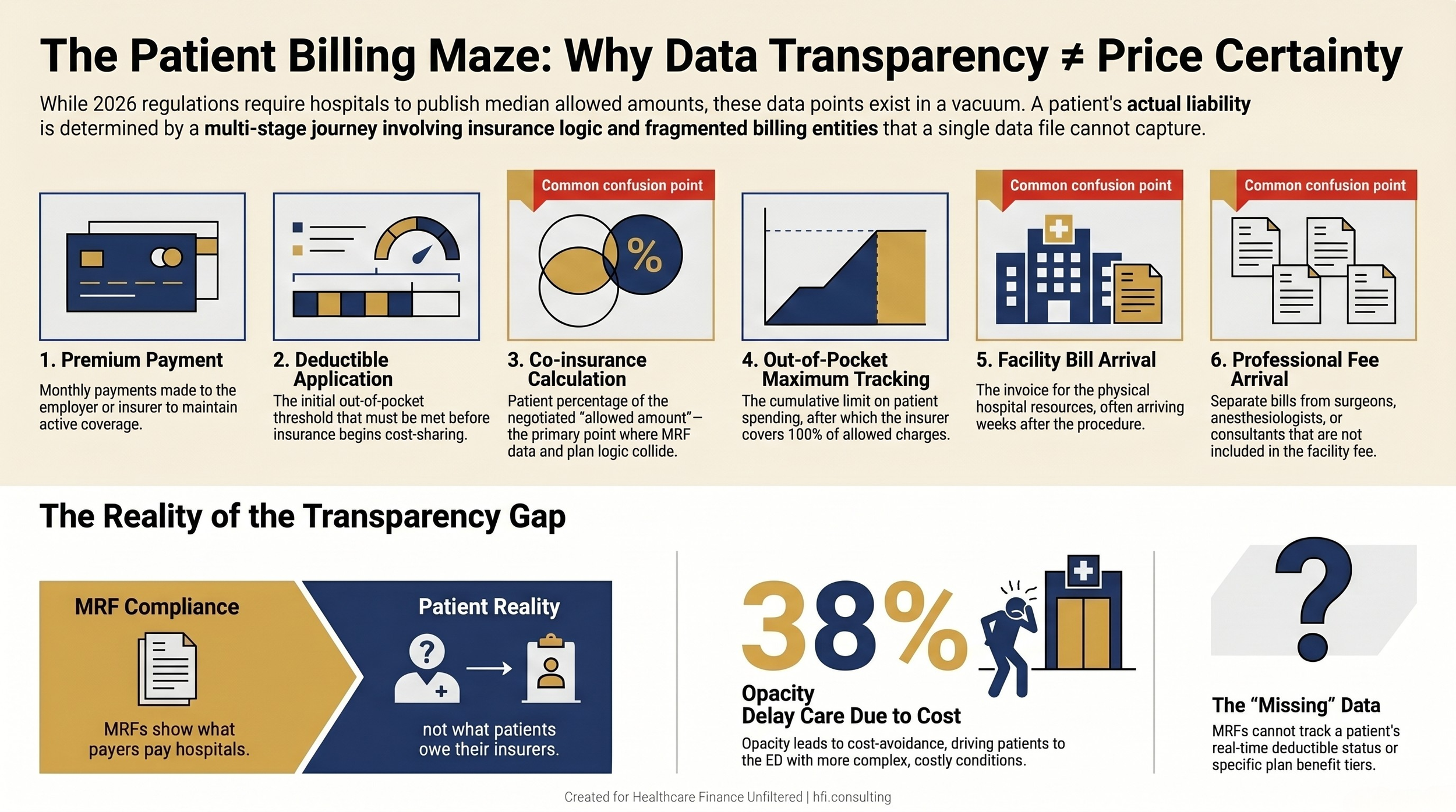
Patient billing journey flowchart showing six stages from premium payment to final bill, with three primary confusion points marked at co-insurance calculation, facility billing, and separate physician billing.
Working in Medicare Advantage operations at Florida Blue Medicare, I heard this play out in a way that is difficult to quantify in a revenue cycle dashboard. During health risk assessments, members over 65, many on fixed incomes, would disclose in writing that they had made choices between their medications and groceries. Not hypothetically. On surveys designed to capture their clinical risk.
The pharmacy coverage gap, still commonly called the Donut Hole even after the Inflation Reduction Act modified it, is technically disclosed in plan documents. That disclosure does not make it understandable to a beneficiary managing a monthly budget on Social Security. Price transparency regulations do not reach the complexity of pharmacy benefit tiers, step therapy requirements, or the lag between when a patient pays for a medication and when the coverage calculation updates.
Seniors on fixed incomes are not an outlier population in healthcare finance. They are among the highest-utilization, highest-complexity patients in your system. And they are making cost-avoidance decisions that directly affect when and where they seek care.
Gallup data from 2022 found that 38 percent of Americans reported delaying needed medical care due to cost, a 12-point increase from the prior year and the highest reading in the survey's 22-year history. Among those who delayed care, 27 percent said the treatment they skipped was for a very or somewhat serious condition.
For hospital CFOs, that statistic has a direct operational translation. Patients who delay care for serious conditions do not disappear from the system. They return through the emergency department, often sicker, with more complex presentations, less coverage, and a worse financial starting position. The cost of delayed care lands back inside the health system. Internal links: See AI-Powered Revenue Leakage Prevention: The CFO's Implementation Guide for 2026 for the operational cost of upstream gaps in patient financial engagement.
What Finance Leaders Are Not Saying Out Loud
There is a reason hospital-published price data stays opaque even when hospitals invest in compliance. System complexity is part of it. But there is a quieter tension that rarely gets named in a boardroom.
Employers chose a health system because of a negotiated rate structure built into their annual benefit plan. Publishing granular, easily comparable allowed-amount data gives large insurers a clearer view of where a hospital's floor actually sits before the next contract renewal. That is a real concern for CFOs, and it explains why technical compliance has remained the ceiling rather than the starting point.
"The data hospitals are publishing is designed to satisfy a regulation. It is not yet designed to answer the question a patient is actually asking."
The HFMA has documented a related gap. In a 2024 survey, nearly 83 percent of healthcare finance and revenue cycle leaders said their organization does a good job explaining financial matters to patients. The patient experience data suggests a different picture.
One of the most underappreciated sources of patient frustration is the co-insurance refund cycle. Some providers still collect cost-sharing at the point of service, then issue a refund after the claim adjudicates and the calculation reveals an overcollection. That refund goes back to the patient's personal checking account. If the original payment came from an HSA, the patient cannot simply deposit the refund back without navigating contribution limits and account rules that most patients do not understand.
This is a micro-level example of a macro-level structural problem. The billing system was designed by and for operational insiders. Finance leaders who have spent careers inside it often cannot perceive it from the outside. See CMS Medicaid Fraud Crackdown 2026: What Hospital Finance Leaders Must Do Now for additional context on how CMS is using named accountability requirements to shift operational culture across compliance domains.
A Framework for Moving Beyond Compliance
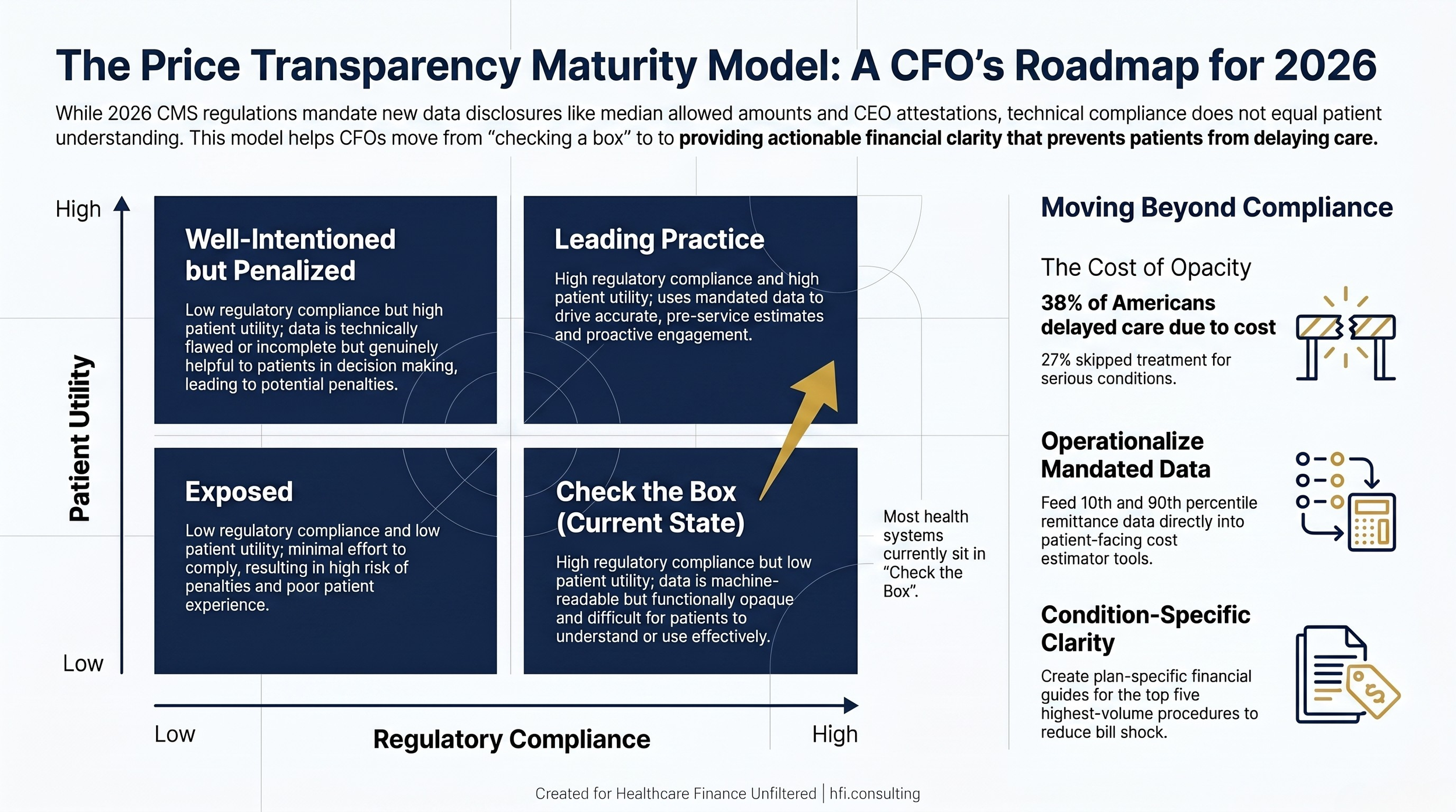
Price Transparency Maturity Model 2x2 matrix showing four quadrants from Exposed to Leading Practice, with most health systems currently in the Check the Box quadrant.
Hospital finance leaders have operational options that do not require renegotiating payer contracts or rebuilding the charge description master.
Start with the gap between your MRF and a plain-language patient estimate. Your median allowed amount data is now calculated from actual remittance data. That same data can feed a patient-facing cost estimator that shows a real dollar range, by insurance plan, for your most common procedures. The compliance work you just completed for the MRF is the input your estimator needed.
Audit your facility and professional billing split communications. One of the most consistent sources of patient shock is receiving two or more bills from what felt like a single encounter. When a procedure generates separate bills from the facility, the surgeon, the anesthesiologist, and a consulting physician, the patient experiences four unexpected charges. A pre-service financial communication that names all expected billing entities with estimated amounts for each closes a gap that no MRF requirement touches.
Use your 10th and 90th percentile data as a financial counseling tool. The new CMS requirements give you a range based on actual claims. The difference between the 10th and 90th percentile allowed amount for a given procedure is an honest representation of variability a patient might face. A patient with an HDHP deserves to know whether they are likely to pay $800 or $3,200 for an outpatient procedure before they schedule it.
Build condition-specific financial literacy content for your highest-volume procedure categories. You do not need to explain all of healthcare billing to every patient. You need to explain clearly what a patient with a specific plan type will experience during a knee replacement, a colonoscopy, or a cardiac stress test. Condition-specific financial guides are more actionable than general insurance education.
Healthcare Finance Unfiltered covers price transparency, revenue cycle strategy, and operational finance for CFOs and finance leaders across health systems. If you are working through a patient-facing pricing strategy and want a framework for the conversations ahead, subscribe for weekly analysis at hfi.consulting
What Good Actually Looks Like
Heart and Vascular Care in Georgia achieved a 95 percent net collection rate and reduced denials to 3.7 percent by shifting from post-claim revenue cycle response to pre-service patient education. The operational change was not a new technology platform. It was three-way calls between the practice, the patient, and the health plan before care was delivered.
That model is not scalable at identical volume for a 500-bed health system. The principle is. Pre-service financial outreach, by service line, targeting patients with high-deductible health plans or known cost-sensitivity markers in their claims history, is operationally achievable. The 2026 MRF data gives your team the baseline cost structure. Revenue cycle infrastructure already handles pre-authorization. Adding a financial clearance step that communicates actual expected liability is an extension of existing workflow.
Vanderbilt University Medical Center built a cost estimator with a 98 percent accuracy rate by monitoring the delta between pre-service estimates and actual claim adjudication outcomes over time. That feedback loop is what drives accuracy. It is also how you identify where payer contract terms and claim processing behaviors are diverging from what patients were told to expect at the front end.
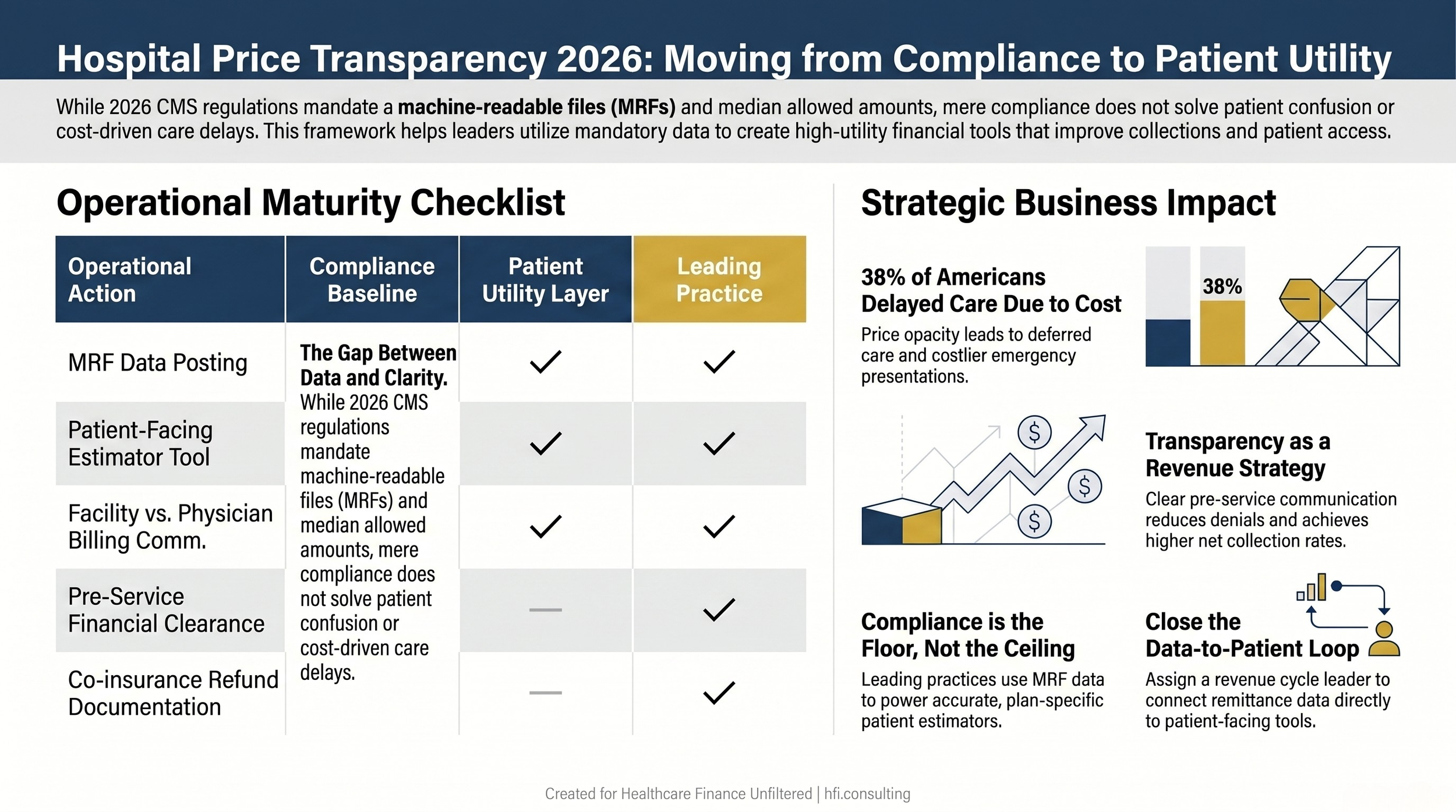
Three-column table comparing compliance baseline, patient utility layer, and leading practice actions for hospital price transparency implementation.
The finance leaders moving ahead of this issue are not waiting for a stronger regulation. They are treating price transparency as a patient access strategy. Delayed care is lost revenue. Confused patients are a collections liability and a community health risk. Clear pre-service financial communication reduces denials, improves collections, and strengthens the community benefit argument that not-for-profit systems need to make every year.
The 2026 rule gives your team better data than has ever been publicly required. The question for every CFO in this space is whether that data gets used.
The Operational Ask
Assign a revenue cycle leader to own the gap between MRF compliance and patient-facing utility. That person's job is to connect remittance data to your cost estimator tool and build a feedback loop between what patients are told and what claims actually adjudicate.
Create one patient-facing financial guide for your top five procedure categories by volume. Make it plan-specific where possible. Publish it on the same page as your price estimator tool.
Brief your board on the connection between price transparency, patient access, and downstream volume. When patients delay serious care because they cannot predict what they owe, they return more complex and more costly to treat. This is a margin conversation, not only a compliance conversation.
The patients choosing between groceries and medication are in your service area, making those calculations right now. The data your organization is now required to publish could help them plan. The question is whether it is presented in a way that allows them to use it.
Healthcare Finance Unfiltered is published weekly for CFOs and finance leaders navigating operational finance and healthcare policy. Subscribe and access the full archive at hfi.consulting
P.S. I am curious what your team's biggest internal obstacle is to publishing patient-readable price data. Is it the payer contract concern, CDM complexity, or something else? Hit reply and tell me where you are getting stuck.