
Before Your AI Investment Delivers, Your Data Has to Be Ready: A CFO Guide to Governance, Readiness, and Federal Rules That Cut Both Ways
AI ROI depends on data quality, not model sophistication. Here is the governance framework healthcare CFOs need before the next budget cycle.
If your organization is evaluating AI investments this budget cycle, the most important question is not which vendor to choose. It is whether your underlying data is accurate enough to make the AI work. Industry research now shows that 84 percent of healthcare organizations believe data mismatches already contribute to lost revenue, and 81 percent of providers and payers acknowledge they cannot deliver personalized care or communications without complete, accurate patient data. Every AI tool you layer on top of that problem will inherit it.
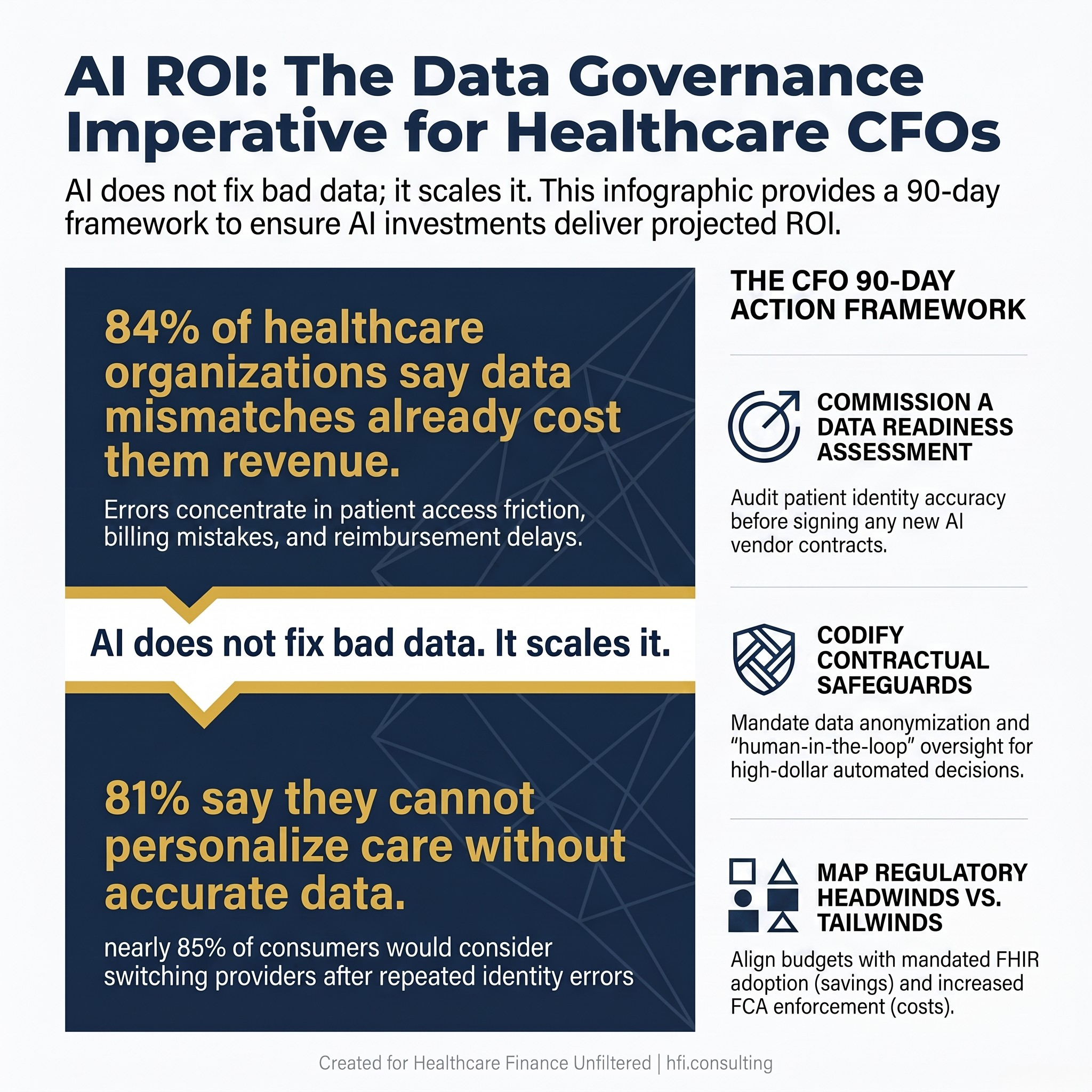
Infographic showing 84 percent of healthcare organizations report revenue loss from data mismatches and 81 percent cannot personalize care without accurate data, framed as an AI readiness warning for CFOs.
The Governance Problem That Predates Your AI Vendor Contract
Healthcare organizations have spent two years evaluating and deploying artificial intelligence. Revenue cycle automation, clinical documentation tools, predictive risk stratification, prior authorization workflows. The market has moved faster than the finance and governance structures supporting it. That execution gap is already showing up in real financial results, as detailed in The AI Automation Trap: Why Healthcare Finance Leaders Are Quietly Walking Back Their Biggest Bets.
The fundamental problem is not the technology. It is the data feeding it.
When patient records contain duplicates, mismatched identities, or incomplete demographic and insurance information, those flaws do not disappear inside an AI system. They get operationalized. A predictive model trained on inaccurate risk stratification data will consistently misidentify high-risk patients. An automated prior authorization tool running on mismatched member records will generate claim errors at scale. An AI-assisted billing workflow built on top of duplicate patient accounts will produce billing errors across multiple applications simultaneously, and the source of those errors will not be immediately obvious to the teams relying on the output.
This is the garbage-in, garbage-out problem applied to a sector where the downstream consequences include denied claims, delayed care, and regulatory exposure.
Before your next AI vendor conversation, the CFO's job is to ask a specific question: what is the state of our patient identity data, and what does fixing it cost compared to what we are projecting in AI-driven savings?
What Data Governance Actually Costs When You Ignore It
The financial case for data governance investment is easier to make than most CFOs expect, because the cost of ignoring it is already showing up in existing line items.
Research cited by identity data specialists at Verato puts the revenue exposure in concrete terms. Eighty-four percent of healthcare organizations say data mismatches contribute to lost revenue. The losses concentrate in three areas: patient access friction that reduces engagement and follow-through on care plans, revenue cycle errors including billing mistakes, duplicate claims, and reimbursement delays, and CRM and marketing failure where 83 percent of providers and payers agree that data quality problems undermine their ability to effectively communicate with the patients and members they are trying to reach.
Nearly 85 percent of consumers say they would consider switching providers after repeated identity or data errors. Eighty-one percent report having to provide the same personal or health information multiple times across visits and departments.
Patient dissatisfaction from data friction is not a clinical operations problem in isolation. It is a volume and retention problem with a direct revenue cycle consequence.
The CFO frame here is straightforward. If your organization is projecting 15 to 20 percent administrative cost savings from AI-driven revenue cycle automation, and your underlying patient identity data has a 10 to 15 percent error rate across key fields, the realistic ROI is materially lower than the projection. Your finance team should be modeling both scenarios before the board presentation.
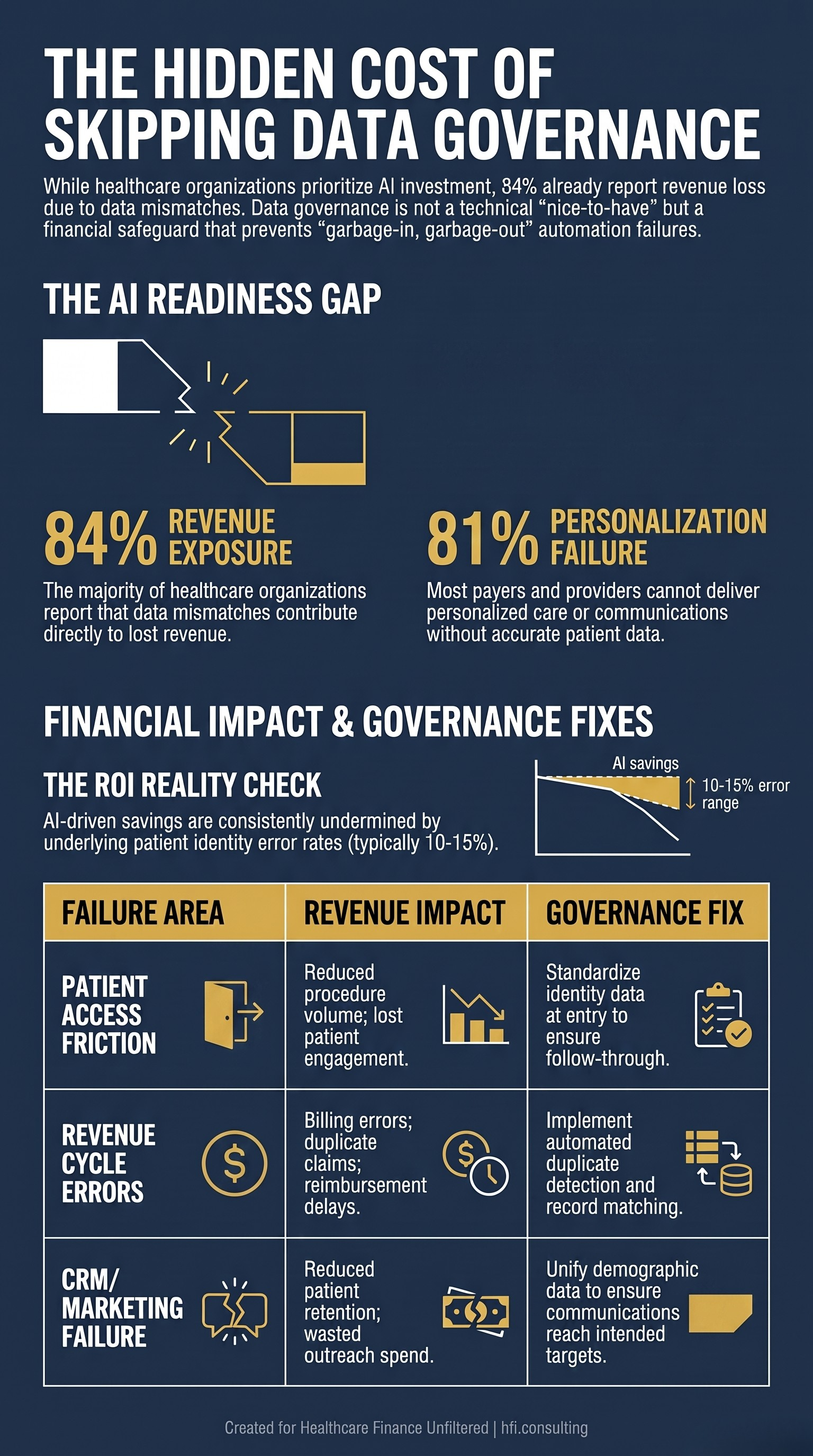
Three-row CFO financial impact table showing how patient data governance failures create revenue losses in patient access, revenue cycle, and CRM for healthcare organizations.
Three AI Risk Categories CFOs Are Not Pricing Into Their Contracts
Most AI vendor contracts in healthcare are negotiated as software agreements. They address uptime, implementation timelines, and support tiers. They rarely address the financial exposure created by the AI itself operating on bad data, or by the data pipelines feeding the AI being compromised. If your organization is still assessing what AI complexity means before signing a vendor contract, Healthcare Application Complexity: What CFOs Need to Know Before the Next AI Investment is a useful starting framework.
There are three risk categories that belong in your AI governance framework and your vendor contracts.
PHI leakage through unauthorized AI ingestion. When clinical or administrative teams use frontier AI tools to summarize claims data, analyze patient records, or draft clinical documentation, they often input Protected Health Information into platforms that do not have explicit non-training clauses or enterprise-grade data handling agreements. If that data is absorbed into an external training dataset, the organization faces a reportable HIPAA breach. The CFO control here is mandatory data anonymization and tokenization requirements written into every AI vendor agreement, with contractual penalties for breach.
Agentic identity risk and lateral access. Advanced AI does not operate through a single login. It operates through automated agents, APIs, and plugins that pull data across systems to automate workflows. If one third-party AI dependency is compromised, an attacker can use that connected agent's permissions to move across your environment. This is the same lateral movement risk covered in Part 1 of this series, now applied specifically to AI-connected systems. The CFO control is requiring Zero Trust architecture for machine identities in your AI vendor agreements, where AI agents are granted only the minimum access required for each specific task.
Model drift and automated execution errors. AI models degrade over time as the data environment changes around them. A prior authorization model trained on last year's payer mix will produce different outputs as that mix shifts. An auto-adjudication tool running without oversight will execute those drifted outputs at scale. The financial exposure from model drift is not a one-time event. It compounds across every transaction the model touches. The CFO control is mandatory human-in-the-loop requirements for high-dollar decisions, and contractual rights to algorithmic audits at defined intervals.
From my work on analytics implementation at health systems through McKesson and Change Healthcare, the organizations that got the most value from their analytics investments were the ones that treated data governance as a precondition, not an afterthought. The tool is only as useful as the data architecture it sits on. That lesson has only become more consequential as AI has replaced static reporting with automated decision-making.
Federal Regulation: What Is Actually Helping and What Is Not
CFOs navigating AI adoption also have to navigate a federal regulatory environment that is moving in multiple directions simultaneously. The honest assessment is that some of it helps and some of it creates significant operational burden.
What is helping.
CMS mandates forcing adoption of standardized FHIR APIs and electronic claims attachments are reducing administrative friction in data exchange. For both payers and providers, this is real cost reduction. Faster claims adjudication, lower documentation overhead, and reduced manual intervention in prior authorization workflows all flow from interoperability standardization.
CMS has also permanently authorized expanded telehealth models, including virtual direct supervision for incident-to billing. That permanency matters for provider finance teams. A predictable, long-term virtual care revenue stream changes capital planning assumptions. Payers benefit from a lower-cost site-of-care alternative that is now structurally embedded in coverage models.
On the cybersecurity side, legislative momentum around a Healthcare Cybersecurity and Resiliency framework is attempting to reward proactive organizations with explicit legal safe harbors during a breach event. The financial logic is that organizations demonstrating implementation of recognized security frameworks face reduced penalties and liability exposure when an attack occurs. This is not yet law, but it is the direction of travel and it changes the ROI calculation on cybersecurity investment.
The White House's most recent AI executive order promotes security coordination between the federal government and private sector, with a specific focus on evaluating frontier models before public release. For healthcare CFOs, the operative guidance from security experts is clear: a federal AI security evaluation is not a HIPAA compliance certification. An organization cannot point to a government pre-release review as a substitute for its own due diligence on AI vendor contracts and data governance.
Also signed on June 12, NSPM-12 establishes formal cybersecurity governance for National Security Systems, re-establishes the Committee on National Security Systems under NSA leadership, and sets implementation timelines of 30, 60, and 90 days for policy harmonization, incident reporting standards, and compliance frameworks. NSPM-12 governs federal systems, not healthcare organizations directly. But the memo's explicit reference to public-private partnerships and its mandate that NSS meet or exceed NIST standards signals that federal agencies healthcare organizations interact with daily, including CMS, VA, and DOD-affiliated payers, will be tightening their own security and data exchange requirements on a documented timeline. If your organization has contracts, data feeds, or API connections with any federal agency, the downstream compliance pressure from NSPM-12 is worth tracking in your vendor risk calendar now.
What is hurting.
The No Surprises Act's independent dispute resolution process has been an administrative headache for provider billing teams. Hyper-specific coding requirements for Claim Adjustment Reason Codes and Remittance Advice Remark Codes, combined with strict portal timeline controls, have created significant operational burden for contesting underpayments. Payers face their own compliance overhead managing the process consistently at scale.
DOJ enforcement intensity around the False Claims Act has increased, with healthcare cases representing a significant share of recent recoveries. The enforcement focus on documentation integrity, particularly within Medicare Advantage programs, means CFOs are spending more on continuous defensive coding audits. The Aetna settlement earlier this year is a concrete benchmark for that exposure: Aetna $117.7M False Claims Act Settlement 2026: Risk Adjustment Compliance Guide for Payer CFOs. This is not optional overhead. It is a cost of operating in federal programs.
Recent CMS rate adjustments have also increased Medicare Part B deductibles and inpatient Part A costs. Higher patient cost-sharing shifts the initial financial burden to the patient, spiking self-pay collections challenges and bad debt risk for provider billing teams while creating customer service friction for payer member services operations.
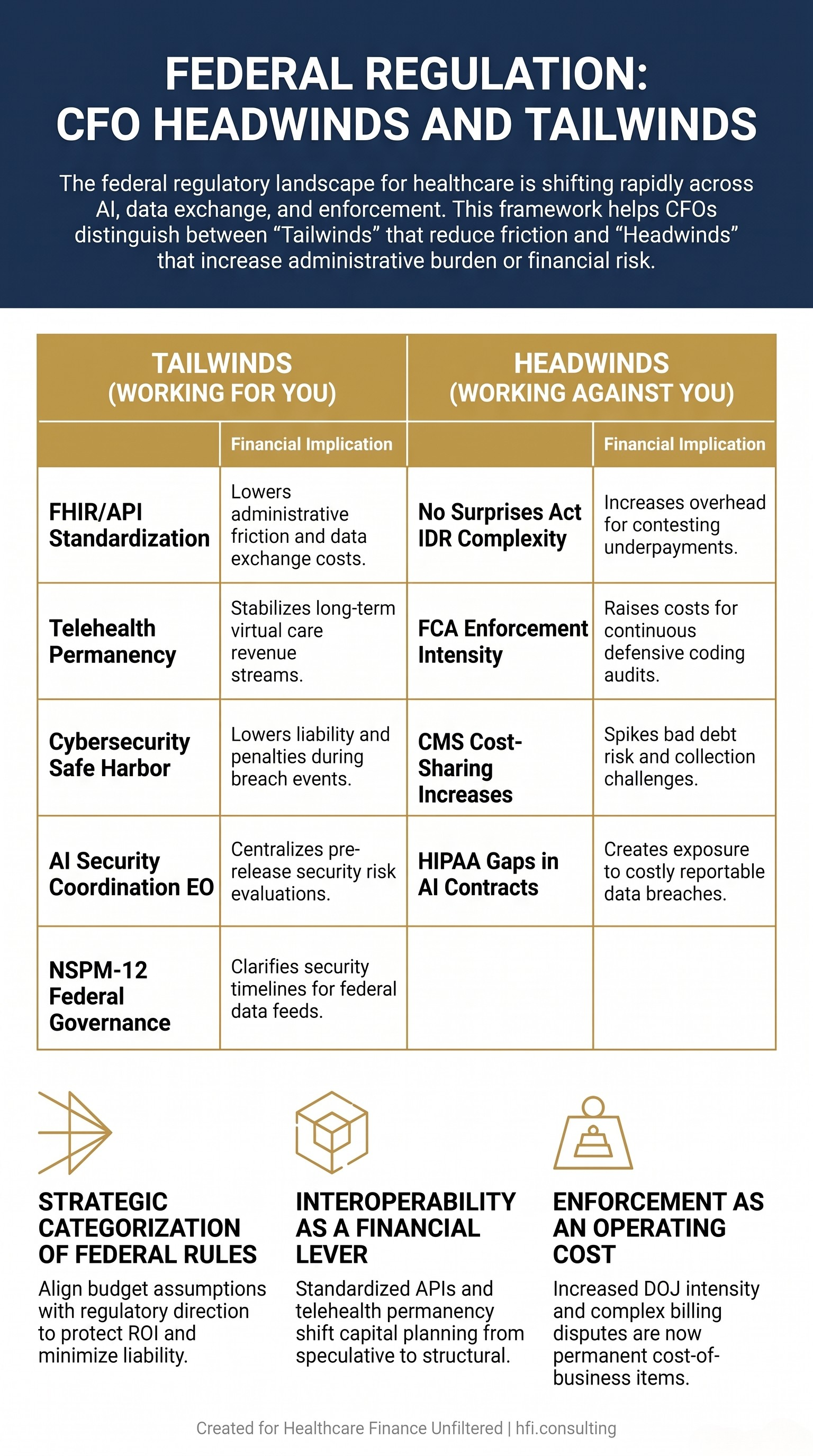
Two-column CFO framework table showing federal healthcare regulatory tailwinds including FHIR standardization and telehealth permanency alongside headwinds including No Surprises Act complexity and False Claims Act enforcement.
The CFO Action Framework: What to Do in the Next 90 Days
The convergence of AI adoption pressure, data governance gaps, and a shifting regulatory environment creates a specific planning problem. There is too much to address at once, and the urgency signals are coming from too many directions simultaneously.
The 90-day frame helps. Three priorities belong at the top.
First, commission a data readiness assessment before any new AI vendor contract is signed. This does not have to be a six-month engagement. A focused audit of patient identity data accuracy, duplicate record rates, and insurance information completeness across your primary systems will tell you whether your projected AI ROI is realistic. If the data quality problem is material, that assessment gives you negotiating leverage on implementation timelines and success metrics in the vendor contract.
Second, build AI governance into your existing vendor management framework rather than treating it as a separate workstream. Every AI tool your organization uses should have documented answers to three questions: where does the data come from and who owns its accuracy, what human oversight exists for high-dollar or high-risk automated decisions, and what are the contractual remedies if the tool produces material errors at scale.
Third, map your regulatory headwinds and tailwinds to your current budget assumptions. If your FY2027 budget includes projected savings from interoperability improvements, verify which of those savings are driven by mandated FHIR adoption versus operational changes your team still needs to execute. If your MA revenue projections assume stable documentation audit overhead, revisit that assumption in light of current FCA enforcement trends. And if your organization has data exchange relationships with CMS, VA, or any DOD-affiliated payer, add NSPM-12's 60 to 90-day federal compliance implementation timeline to your vendor risk monitoring calendar — changes to federal security requirements on those connections can surface quickly.
If your organization is building an AI governance framework or preparing for a data governance assessment and you want a finance-side perspective on structuring the vendor contracts and ROI modeling, that is exactly the kind of work HFI Consulting does with healthcare finance teams. Visit hfi.consulting to learn more or start a conversation.
The Part 1 Connection: Why These Two Articles Belong Together
If you read Part 1 of this series, you saw how the Epic interoperability lawsuit and the ransomware threat environment are creating new financial liabilities through the same vendor API ecosystems that AI tools also rely on.
The data governance problem in this article and the cybersecurity risk problem in Part 1 share a common root: healthcare organizations have moved faster on technology adoption than on the governance structures required to manage the financial exposure that technology creates. Your EHR Is Now a Legal Liability: What the Epic Lawsuit and 460 Ransomware Attacks Mean for Your Budget
The CFOs who will be in the strongest position two years from now are not the ones who adopted AI earliest. They are the ones who built the governance infrastructure to make AI perform as projected and to limit the liability when it does not.
That is not a technology strategy. It is a finance strategy.
The regulatory environment, the AI vendor landscape, and the cybersecurity threat picture are all moving quickly enough that quarterly reassessment of these frameworks is not overcautious. It is appropriate. If your team is working through any of these planning questions and wants a sounding board from someone who has sat on both the provider and payer side of these decisions, reach out at hfi.consulting.
P.S. When your organization evaluates a new AI tool, does the finance team participate in the vendor due diligence, or does that process sit entirely with IT and clinical leadership? I am curious whether CFOs are at the table before the contract is signed or after the budget impact is already locked in. Hit reply and tell me how your organization handles it.
HFI Consulting works with healthcare finance leaders on AI governance, vendor risk, data strategy, and strategic finance advisory. Learn more at hfi.consulting.